
Abstract
Purpose
Ectopic fat is often identified in obese subjects who are susceptible to the development of type 2 diabetes mellitus (T2DM). The ectopic fat favours the decrease in insulin sensitivity (IS) and adiponectin levels. We aimed to evaluate the effect of biliopancreatic diversion (BPD) on the accumulation of ectopic fat, adiponectin levels and IS in obese with T2DM.
Materials and Methods
A nonrandomised controlled study was performed on sixty-eight women: 19 lean-control (23.0 ± 2.2 kg/m2) and 18 obese-control (35.0 ± 4.8 kg/m2) with normal glucose tolerance and 31 obese with T2DM (36.3 ± 3.7 kg/m2). Of the 31 diabetic women, 20 underwent BPD and were reassessed 1 month and 12 months after surgery. The subcutaneous adipose tissue, visceral adipose tissue, epicardial adipose tissue and pericardial adipose tissue were evaluated by ultrasonography. The IS was assessed by a hyperglycaemic clamp, applying the minimal model of glucose.
Results
One month after surgery, there was a reduction in visceral and subcutaneous adipose tissues, whereas epicardial and pericardial adipose tissues exhibited significant reduction at the 12-month assessment (p < 0.01). Adiponectin levels and IS were normalised 1 month after surgery, resembling lean-control values and elevated above the obese-control values (p < 0.01). After 12 months, the improvement in IS and adiponectin was maintained, and 17 of the 20 operated patients exhibited fasting glucose and glycated haemoglobin within the normal range.
Conclusions
After BPD, positive physiological adaptations occurred in grade I and II obese patients with T2DM. These adaptations relate to the restoration of IS and decreased adiposopathy and explain the acute (1 month) and chronic (12 months) improvements in the glycaemic control.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Adiposopathy is characterised by the pathological accumulation of adipose tissue, due to environmental factors in genetically and epigenetically susceptible individuals. One of the anatomical manifestations of adiposopathy is the accumulation of ectopic fat, which is commonly found in obese individuals prone to the development of type 2 diabetes mellitus (T2DM) [1].
The accumulation of ectopic fat helps to reduce insulin sensitivity (IS) and adiponectin and increases inflammation in adipose tissue, increasing the expression and secretion of pro-inflammatory cytokines and contributing to the development of T2DM [2]. The ectopic fat depots can be grouped according to their metabolic effects: the first group consists of those with predominantly systemic effects, such as visceral abdominal adipose tissue (VAT); the second group consists of those with predominantly local toxic effects, including epicardial (EAT) and pericardial adipose tissue (PAT) [3–6].
The treatment of T2DM involves dietary and behavioural interventions as therapies of choice. In subjects with BMI ≥35.0 kg/m2 in whom glycaemic control does not reach acceptable levels with drug therapy and associated changes in lifestyle, bariatric surgery is considered a treatment option. Specially, if T2DM is associated with other comorbidities, surgery could be considered for individuals with BMI ≥30.0 kg/m2 [8]. The surgical treatment is based on weight loss, calorie restriction and hormonal and metabolic changes resulting from anatomical-functional changes in the digestive tract [7–9].
In a recent meta-analysis, the remission of T2DM were more pronounced in patients undergoing biliopancreatic diversion (BPD) surgery compared with other techniques [10]. To date, the mechanisms that modulate the remission of T2DM after BPD are only partially known. Although some studies have reported significant improvements in IS [11–13], the effect of BPD on the deposition of EAT and PAT fat has not yet been explored.
To identify additional evidence concerning the underlying pathophysiological mechanisms related to the remission of T2DM after BPD, the objectives of this study were as follows: (1) to evaluate the effect of BPD on ectopic fat accumulation (visceral, epicardial and pericardial), plasma adiponectin levels and IS in grade I and II obese women with T2DM and (2) to compare the accumulation of ectopic fat, adiponectin levels and IS in the surgical group (pre- versus post-surgery) with two control groups consisting of normal weight and obese grade I and II women, both with normal glucose tolerance.
Materials and Methods
Study Design and Subjects
A nonrandomised controlled study was performed with 68 premenopausal women divided into three groups: lean normal glucose tolerant (LeanNGT) (n = 19; BMI 23.0 ± 2.2 kg/m2), obese normal glucose tolerant (ObeseNGT) (n = 18; BMI 35.0 ± 4.8 kg/m2) and obese with overt type 2 diabetes (ObeseT2DM) (n = 31; BMI 36.3 ± 3.7 kg/m2). Of the 31 ObeseT2DM subjects, 20 underwent BPD surgery. The surgical group was studied at baseline and 1 and 12 months post-surgery.
Diabetes was diagnosed according to the American Diabetes Association criteria [14]. In the ObeseT2DM group, the mean duration of diabetes was 4.7 ± 4.5 years. Of the patients who underwent BPD surgery, 12 were treated exclusively with metformin, seven were treated with metformin and sulfonylureas, and one was treated with diet and exercise.
The inclusion criteria were age over 20 years old, premenopausal and negative islet autoimmunity. The exclusion criteria were the use of incretin mimetics, dipeptidyl peptidase-4 inhibitors or insulin; significant kidney or liver dysfunction; recent neoplasia (<5 years) and the use of oral or injectable corticosteroids for more than 14 consecutive days in the last 3 months.
This study was approved by the Ethics Committee of the State University of Campinas, Brazil. All participants provided written informed consent before participation.
Biliopancreatic Diversion Surgery
The original technique reduces the total length of intestinal absorption to 250 cm with a 50-cm common channel, increasing malnutrition risk, particularly in less-obese individuals, like the patients of the present study [15]. Therefore, this study uses an adapted BPD technique to avoid nutritional complications. The BPD is performed with an approximately 60 % distal gastric resection and a long Roux-en-Y reconstruction. The volume of the stomach after surgery is approximately 300 ml. The small bowel is transected at 2.8–3.2 m from the ileocecal valve, and its distal end is anastomosed to the remaining stomach. The proximal end of the ileum, comprising the remaining small bowel (involved in carrying biliopancreatic juice but excluded from food transit), is anastomosed to the bowel in an end-to-side fashion 80–120 cm proximal to the ileocecal valve. Consequently, the total length of absorbing bowel is reduced to 280–320 cm, of which the final 80–120 cm, the common channel, is where biliopancreatic juices and ingested food mix.
Anthropometrical Assessment
All of the subjects underwent detailed anthropometric examination, according to standard procedures, by the same examiner while wearing light clothing and no shoes. Height, weight and waist circumference at the umbilicus level were measured. All measurements were taken in duplicate and averaged.
Assessment of Subcutaneous Adipose Tissue and Ectopic Fat Depots: Intra-Abdominal Visceral Adipose Tissue, Epicardial Adipose Tissue and Pericardial Adipose Tissue
The measurements of the different adipose tissues were performed by the same professionals throughout the period of data collection.
The thickness of subcutaneous and VAT in the abdominal region were evaluated by ultrasonography using a 3.5 MHz transducer positioned 1 cm above the umbilicus. The subcutaneous adipose tissue thickness was defined as the distance between the skin and the outer surface of the abdominal rectus muscle. The VAT was defined as the distance between the internal surface of the rectus abdominis muscle and the anterior wall of the aorta. The reading was performed in duplicate directly from frozen images on the screen [16].
The evaluation of EAT and PAT was performed by two-dimensional guided M-mode transthoracic echocardiography, using the high-resolution equipment (Vivid 3, GE Healthcare) with a linear transducer 10 L H40412LG (4–11 MHz). During the examination, the patients were in the left lateral decubitus position. The EAT was defined as the relative space echo located between the outer wall of the myocardium and visceral layer of the pericardium. The PAT was defined as the space located between the echo parietal and visceral pericardium. The thicknesses were measured in the parasternal long and short axis frozen B-mode images, perpendicular to the free wall of the right ventricle at end systole in three cardiac cycles using the aortic ring as a point of reference for the long parasternal anatomical axis and the level of the papillary muscles for the short axis [17, 18]. All measurements were taken in triplicate, and the mean value was used for the analyses. To ensure the precision of the measurements obtained, the intraclass coefficients of correlation (ICC) were calculated. The ICC for EAT was 0.95 (95 % CI 0.92–0.97) and for PAT was 0.88 (95 % CI 0.82–0.92), p < 0.001 for all.
Oral Glucose Tolerance Test (OGTT)
After a 12-h overnight fast, an intravenous catheter was placed into the antecubital vein. The subjects ingested a 75-g glucose load. Blood samples were collected at 0 (pre-load) and 120 min (post-load) to measure glucose [7].
Insulin Sensitivity Assessment: Hyperglycaemic Clamp Test
After a 12-h overnight fast, a cannula was retrogradely inserted into a peripheral hand vein. Glucose was infused into an antecubital vein in the opposite arm and divided into two phases: the “first dose”, which included a sufficient amount of glucose to increase the blood glucose levels to the desired plateau (180 mg/dl), and the “maintenance dose”, which was calculated every 5 min during the test and was dependent on blood glucose measurements. Blood samples were obtained every 2.5 min during the first 10 min of glucose infusion and then every 5 min up to 180 min. Glucose levels were measured in all blood samples. Insulin levels were measured at the same time as glucose under basal conditions and for the first 20 min of infusion and every 20 min thereafter [19]. The glucose minimal model was used to calculate insulin sensitivity (IS) [20].
Assays
Plasma glucose levels were measured in the fasting state and during the dynamic tests using a glucose analyser (YSI 2700) with a coefficient of variation (CV) of 2 %. Plasma insulin levels were analysed using an automated two-site chemiluminescent immunometric assay. The intra-assay and inter-assay CVs were 5.2–6 · 4 % and 5.9–8.0 % for insulin, respectively. Adiponectin levels were measured by an ELISA, and all had coefficients of variation below 10 %.
Statistical Analysis
Statistical analyses were performed using IBM SPSS-Statistics 20.0. The data are presented as the mean ± standard deviation for normally distributed data and as the median (25th–75th percentiles) for nonparametric data. The Kruskal-Wallis test was used to compare three independent groups. A post hoc analysis with Bonferroni’s multiple range test was used to determine which groups differ from the other groups. Friedman’s test was used to compare repeated measures. The Wilcoxon signed-rank test associated with Bonferroni correction was used to test the effects with a significance level of 0.0167. The correlation coefficient of Spearman was applied to test the correlation between the delta (∆ = postoperatively value–preoperatively value) of the ectopic fat deposit and its preoperative values. For all of the other tests, significance was set at p < 0.05.
Results
Clinical and Metabolic Characterisation at Baseline
The ObeseNGT and ObeseT2DM groups were in the same BMI range; nonetheless, the groups exhibited distinct distributions of body fat. The ObeseT2DM group exhibited a larger waist circumference than the ObeseNGT group, indicating the presence of an increased deposit of fat in the abdominal region. This greater accumulation of fat was explained by the greater thickness of subcutaneous adipose tissue. Both groups were similar with respect to the thickness of VAT. However, the accumulation of EAT was more pronounced in the ObeseT2DM group compared with the ObeseNGT group. Plasma adiponectin and IS were also similar between the two obese groups but were decreased in the ObeseT2DM group compared with the LeanNGT group (Table 1).
Postoperative Clinical and Metabolic Characterisation
All of the subjects who underwent BPD were studied 1 month and 12 months after the procedure. Excess body weight decreased significantly at both time points with a concurrent significant reduction in waist circumference and body fat percentage. Glycated haemoglobin was significantly reduced at both time points, whereas fasting blood glucose, blood glucose 2 h after stimulation with oral glucose and fasting insulin decreased in the first month postoperatively and maintained their reduced levels 12 months after surgery (Table 2).
Of the patients who underwent surgery, 12 were exclusively treated with metformin, seven were treated with metformin associated with sulfonylureas and one subject was exclusively treated with diet and exercise. In the first month after surgery, most patients stopped using antidiabetic drugs. Only one patient was taking metformin, and another patient was in therapy with metformin associated with sulfonylurea. Twelve months after BPD, only one patient was using metformin associated with sulfonylurea. The antidiabetic medications were stopped at 1 month after surgery when the patients presented fasting plasma glucose levels <99 mg/dl and 2 h postprandial glucose levels <140 mg/dl. At 12 months medication were stopped when fasting plasma glucose levels were <99 mg/dl and 2 h postprandial glucose levels were < 140 mg/dl or glycated haemoglobin <6 %.
With respect to the evolution of the glycaemic control, 1 month after surgery, 12 of the 20 obese patients with T2DM exhibited fasting glucose levels within the normal range (<100 mg/dl), and seven exhibited glycated haemoglobin <6 %. One year after surgery, 13 exhibited fasting glucose levels within the normal range and glycated haemoglobin levels <6 %, 17 exhibited only fasting glucose levels within the normal range and 17 exhibited only glycated haemoglobin levels <6 %.
Accumulation of Subcutaneous Adipose Tissue, Ectopic Fat, Serum Adiponectin and Insulin Sensitivity After Surgery
The thickness of the subcutaneous and VAT exhibited a significant reduction 1 month and 12 months postoperatively. The thickness of EAT and PAT exhibited a significant reduction at the assessment performed 12 months after surgery (Fig. 1), with an average reduction of 21 % for EAT and of 25 % for PAT (Fig. 2). Adiponectin levels and the IS increased over the two evaluation times (Fig. 1).

Evolution of the accumulation of adipose tissue (a), insulin sensitivity (b) and serum adiponectin (c) in obese women with type 2 diabetes at baseline, 1 month and 12 months after surgery. Friedman test and Wilcoxon signed-rank test associated with Bonferroni correction. *p < 0.05 vs. pre-BPD, **p < 0.05 vs 1 month post-BPD. IS insulin sensitivity, SAT subcutaneous adipose tissue, PAT pericardial adipose tissue, EAT epicardial adipose tissue, VAT visceral adipose tissue

Evolution of the accumulation of epicardial (a) and pericardial (b) adipose tissues in obese women with type 2 diabetes at baseline and 12 months after surgery. EAT epicardial adipose tissue, PAT pericardial adipose tissue
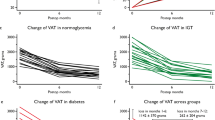
According to Fig. 3, at baseline, the patients with higher levels of VAT, EAT and PAT were the patients with a greater reduction in their respective magnitudes 12 months after BPD. No significant correlations with IS and adiponectin were identified (data not shown).

Correlation coefficients between baseline values and delta values of different ectopic fat depots. Spearman coefficient of correlation. BMI body mass index, EAT epicardial adipose, PAT pericardial adipose tissue, VAT visceral adipose tissue
In Fig. 4, it is possible to observe the comparisons between the ObeseT2DM surgical group and the control groups at all evaluation time points. The thickness of SAT and EAT in the ObeseT2DM group before the operation and 1 month after the operation was greater than the thicknesses of the two control groups. One year after surgery, the thicknesses of SAT and EAT resembled the values of the ObeseNGT group and remained higher than that of the LeanNGT group. The VAT and PAT in the ObeseT2DM group before and 1 month after BPD exhibited greater thickness with respect to the LeanNGT group and similar values compared to the ObeseNGT group. One year after the intervention, the thickness of VAT and PAT reached levels that were comparable to the LeanNGT group and reduced compared with the ObeseNGT group.

Comparison of the accumulation of adipose tissue, adiponectin and insulin sensitivity between the two control groups with the ObeseT2DM group at baseline, 1 month and 12 months after surgery. Data are presented as the mean ± standard deviation for variables with normal distributions and median (interquartile range) for variables without normal distributions. IS insulin sensitivity, SAT subcutaneous adipose tissue, PAT pericardial adipose tissue, EAT epicardial adipose tissue, VAT visceral adipose tissue. p indicates that the Kruskal-Wallis test was performed, followed by the Bonferroni test; *p < 0.05 vs. LeanNGT; **p < 0.05 vs. ObeseNGT
Preoperatively, the plasma adiponectin of the ObeseT2DM group was similar to that of the ObeseNGT group and less than the levels of the LeanNGT group. One month after surgery, the difference between the ObeseT2DM group and the LeanNGT group was no longer statistically significant. Twelve months after surgery, the adiponectin levels in the ObeseT2DM group remained similar to the levels in the LeanNGT group, with higher levels of adiponectin than the ObeseNGT group.
Before surgery, the ObeseT2DM group exhibited lower IS as measured by the hyperglycaemic clamp test compared with the LeanNGT group and similar IS compared with the ObeseNGT group. One month after BPD, the ObeseT2DM group exhibited IS levels statistically comparable to the LeanNGT group and higher than the ObeseNGT group (p < 0.05). One year after surgery, the ObeseT2DM group exhibited higher IS compared with both controls.
The patients who failed to normalise fasting glucose level or glycated haemoglobin at 1 year following BPD did not present different levels of EAT, PAT, VAT, SAT, adiponectin and IS, compared with those that normalised the blood glucose control (data not shown).
Conclusion
This is the first study to investigate the impact of BPD surgery on the accumulation of epicardial and pericardial ectopic fat. Concurrently, visceral fat, adiponectin and insulin sensitivity by the clamp technique were evaluated. The main findings of this study were the following: (1) reduction in the thickness of intra-abdominal subcutaneous and VAT 1 month after surgery, (2) reduction in the thickness of EAT and PAT 12 months after surgery and (3) normalisation of the adiponectin levels and the IS 1 month after surgery with substantial increases in the levels of IS 12 months after surgery. The reductions in the accumulation of VAT, EAT and PAT identified in this study after BPD are consistent with the findings of previous studies that evaluated the effect of Roux-en-Y gastric bypass and gastric banding in the accumulation of these fat depots. A study conducted with 33 grade III obese patients undergoing Roux-en-Y gastric bypass identified reductions in the accumulation of VAT and EAT 6 months after surgery by computed tomography [21]. Willens and colleagues evaluated the effect of gastric banding on the EAT of 23 grade III obese patients 8 months after surgery [22]. The authors identified reductions of EAT in proportion to the accumulation of EAT in the preoperative period. For comparison, no studies that have evaluated the changes in EAT and PAT 1 month after bariatric surgery were found. With respect to other ectopic fat depots, Greco and colleagues reassessed obese patients 6 months after BPD and found that lipid deprivation selectively depletes intramyocellular fat stores and induces a normal metabolic condition with respect to IS, intracellular insulin signalling and circulating leptin regardless of a persistent excess of total body fat mass [23].
Due to the common embryonic origin, the adipose tissue around the vessels and the epicardial and pericardial regions exhibit the same metabolic and inflammatory characteristics of the intra-abdominal visceral fat. In addition, the EAT and PAT have a higher lipolytic rate than the subcutaneous adipose tissue [24]. In a recent publication, our group demonstrated that VAT and EAT are highly correlated [25]. However, despite these previously mentioned embryonic and metabolic characteristics, the present study demonstrated a different response in VAT and subcutaneous adipose tissue compared with EAT and PAT after weight loss induced by BPD.
In the present study, the increase in adiponectin levels after BPD also reflects the decrease in adiposopathy in these patients, which may have contributed to the improvement in IS. Adiponectin is an insulin-sensitiser cytokine that operates in decreasing hepatic gluconeogenesis and increased muscle fatty acid oxidation. In a study conducted by Salani and colleagues, the authors observed a significantly increased serum adiponectin 1 month after BPD surgery in parallel with the 11 % decrease in body weight [26].
The findings of the present study on the improvement in IS are consistent with the results of BPD reported in previous studies that examined obese patients with T2DM [11–13, 27]. The normalisation of IS after malabsorptive procedures seems to occur partially independently of weight loss. In a study of morbidly obese patients with glucose tolerance ranging from normal to T2DM, the results revealed that the most pronounced improvement in IS was reached 7–10 days after BPD [13]. A recent study from our group found a lack of improvement in peripheral IS 1 month after Roux-en-Y gastric bypass in women, reinforcing the difference in the metabolic effects of different surgical techniques [28]. The acute improvement in IS seems to be a specific effect of the technique of BPD and is associated with the modulation of intestinal factors for surgery. The long-term improvement of IS is likely related to weight loss and improved adiposopathy [29].
The limitation of the present study concerns the use of ultrasonography methods to assess the ectopic fat depots, as computed tomography and magnetic resonance imaging are the gold standard methods, with more precision and accuracy. The ultrasound method presents lower cost and exposure risk than these methods and has been demonstrated to be the best alternative method for the evaluation of intra-abdominal adipose tissue deposition in obese women. The VAT measured by ultrasound correlates well with CT-determined VAT (r = 0.7; p < 0.001) [16]. In addition, EAT assessed by echocardiogram and by magnetic resonance image are strongly correlated (r = 0.9; p < 0.001) [17].
The findings indicate the various positive physiological adaptations after BPD in grade I and II obese patients with T2DM. These adaptations are related to the restoration of IS and decreased adiposopathy, explaining acute (1 month) and chronic (12 months) improvements in the level of glucose tolerance and glycaemic control observed. Understanding the mechanisms of changes in metabolism after BPD should contribute to the development of new clinical and surgical approaches to treating the disease.
References
Bays HE. Adiposopathy is “sick fat” a cardiovascular disease? J Am Coll Cardiol. 2011;57:2461–73.
Nolan CJ, Damm P, Prentki M. Type 2 diabetes across generations: from pathophysiology to prevention and management. Lancet. 2011;378:169–81.
Britton KA, Fox CS. Ectopic fat depots and cardiovascular disease. Circulation. 2011;124:e837–41.
Wajchenberg BL, Giannella-Neto D, da Silva ME, et al. Depot-specific hormonal characteristics of subcutaneous and visceral adipose tissue and their relation to the metabolic syndrome. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme 2002;34:616–21.
Iacobellis G, Malavazos AE, Corsi MM. Epicardial fat: from the biomolecular aspects to the clinical practice. Int J Biochem Cell Biol. 2011;43:1651–4.
Chen X, Jiao Z, Wang L, et al. Roles of human epicardial adipose tissue in coronary artery atherosclerosis. J Huazhong Univ Sci Technol Med Sci. 2010;30:589–93.
Standards of medical care in diabetes--2012. Diabetes Care 2012;35:dc12–s011.
Dixon JB, Zimmet P, Alberti KG, et al. Bariatric surgery: an IDF statement for obese Type 2 diabetes. Arq Bras Endocrinol Metabol. 2011;55:367–82.
Dixon JB, le Roux CW, Rubino F, et al. Bariatric surgery for type 2 diabetes. Lancet. 2012;379(9833):2300–11.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248–56.
Mari A, Manco M, Guidone C, et al. Restoration of normal glucose tolerance in severely obese patients after bilio-pancreatic diversion: role of insulin sensitivity and beta cell function. Diabetologia. 2006;49(9):2136–43.
Scopinaro N, Adami GF, Papadia FS, et al. The effects of biliopancreatic diversion on type 2 diabetes mellitus in patients with mild obesity (BMI 30–35 kg/m2) and simple overweight (BMI 25–30 kg/m2): a prospective controlled study. Obes Surg. 2011;21(7):880–8.
Guidone C, Manco M, Valera-Mora E, et al. Mechanisms of recovery from type 2 diabetes after malabsorptive bariatric surgery. Diabetes. 2006;55(7):2025–31.
Executive summary: standards of medical care in diabetes--2012. Diabetes Care 2012;35(Suppl 1):S4–S10
Scopinaro N, Gianetta E, Civalleri D, et al. Bilio-pancreatic bypass for obesity: II. Initial experience in man. Br J Surg. 1979;66(9):618–20.
Ribeiro-Filho FF, Faria AN, Azjen S, et al. Methods of estimation of visceral fat: advantages of ultrasonography. Obes Res. 2003;11(12):1488–94.
Iacobellis G, Assael F, Ribaudo MC, et al. Epicardial fat from echocardiography: a new method for visceral adipose tissue prediction. Obes Res. 2003;11(2):304–10.
Iacobellis G. Epicardial and pericardial fat: close, but very different. Obesity (Silver Spring). 2009;17(4):625.
Mitrakou A, Vuorinen-Markkola H, Raptis G, et al. Simultaneous assessment of insulin secretion and insulin sensitivity using a hyperglycemia clamp. J Clin Endocrinol Metab. 1992;75(2):379–82.
Cobelli C, Caumo A, Omenetto M. Minimal model SG overestimation and SI underestimation: improved accuracy by a Bayesian two-compartment model. Am J Physiol. 1999;277(3 Pt 1):E481–8.
Gaborit B, Jacquier A, Kober F, et al. Effects of bariatric surgery on cardiac ectopic fat: lesser decrease in epicardial fat compared to visceral fat loss and no change in myocardial triglyceride content. J Am Coll Cardiol. 2012;60(15):1381–9.
Willens HJ, Byers P, Chirinos JA, et al. Effects of weight loss after bariatric surgery on epicardial fat measured using echocardiography. Am J Cardiol. 2007;99(9):1242–5.
Greco AV, Mingrone G, Giancaterini A, et al. Insulin resistance in morbid obesity: reversal with intramyocellular fat depletion. Diabetes. 2002;51(1):144–51.
Capurso C, Capurso A. From excess adiposity to insulin resistance: the role of free fatty acids. Vascul Pharmacol. 2012;57(2–4):91–7.
Vasques AC, Souza JR, Yamanaka A, et al. Sagittal abdominal diameter as a marker for epicardial adipose tissue in premenopausal women. Metabolism. 2013;62(7):1032–6.
Salani B, Briatore L, Andraghetti G, et al. High-molecular weight adiponectin isoforms increase after biliopancreatic diversion in obese subjects. Obesity. 2006;14(9):1511–4.
Salinari S, Bertuzzi A, Asnaghi S, et al. First-phase insulin secretion restoration and differential response to glucose load depending on the route of administration in type 2 diabetic subjects after bariatric surgery. Diabetes Care. 2009;32(3):375–80.
Lima MM, Pareja JC, Alegre SM, et al. Acute effect of Roux-en-Y gastric bypass on whole-body insulin sensitivity: a study with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(8):3871–5.
Laferrere B. Diabetes remission after bariatric surgery: is it just the incretins? Int J Obes. 2011;35(3):143.
Acknowledgments
The funds were provided by the Sao Paulo Research Foundation—FAPESP, grants n. 2008/09451-7 and n. 2008/07312-0.
Conflict of Interest
The authors Ana Carolina Junqueira Vasques, José Carlos Pareja, José Roberto Mattos Souza, Ademar Yamanaka, Maria da Saúde de Oliveira, Fernanda Satake Novaes, Élinton Adami Chaim, Francesca Piccinini, Chiara Dalla Man, Claudio Cobelli and Bruno Geloneze declare that they have no conflict of interest reported.
“All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.”
Author information
Authors and Affiliations
Corresponding author
Additional information
UTN Number: U1111-1137-0489/Brazilian Registry of Clinical Trials—ReBEC: RBR-9kdzdv.
Rights and permissions
About this article

Cite this article
Vasques, A.C.J., Pareja, J.C., Souza, J.R.M. et al. Epicardial and Pericardial Fat in Type 2 Diabetes: Favourable Effects of Biliopancreatic Diversion. OBES SURG 25, 477–485 (2015). https://doi.org/10.1007/s11695-014-1400-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1400-1