
Abstract
Obesity is a major public health concern around the world, including Asia. Bariatric surgery has grown in popularity to combat this rising trend. An e-mail questionnaire survey was sent to all the representative Asia-Pacific Metabolic and Bariatric Surgery Society (APMBSS) members of 12 leading Asian countries to provide bariatric surgery data for the last 5 years (2005–2009). The data provided by representative members were discussed at the 6th International APMBSS Congress held at Singapore between 21st and 23rd October 2010. Eleven nations except China responded. Between 2005 and 2009, a total of 6,598 bariatric procedures were performed on 2,445 men and 4,153 women with a mean age of 35.5 years (range, 18–69years) and mean BMI of 44.27 kg/m2 (range, 31.4–73 kg/m2) by 155 practicing surgeons. Almost all of the operations were performed laparoscopically (99.8%). For combined years 2005–2009, the four most commonly performed procedures were laparoscopic adjustable gastric banding (LAGB, 35.9%), laparoscopic standard Roux-en-Y gastric bypass (LRYGB, 24.3%), laparoscopic sleeve gastrectomy (LSG, 19.5%), and laparoscopic mini gastric bypass (15.4%). Comparing the 5-year trend from 2004 to 2009, the absolute numbers of bariatric surgery procedures in Asia increased from 381 to 2,091, an increase of 5.5 times. LSG increased from 1% to 24.8% and LRYGB from 12% to 27.7%, a relative increase of 24.8 and 2.3 times, whereas LAGB and mini gastric bypass decreased from 44.6% to 35.6% and 41.7% to 6.7%, respectively. The absolute growth rate of bariatric surgery in Asia over the last 5 years was 449%.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The epidemic of obesity has escalated globally over the past few years [1]. The WHO reports that globally in 2008, approximately 1.5 billion adults (over the age of 20) were overweight (BMI > 25 kg/m2), and of these, over 200 million men and nearly 300 million women were obese (BMI > 30 kg/m2) [2]. Overweight and obesity are independent risk factors for diabetes, cancer, cardiovascular disease, and premature death [3, 4]. The health burden of obesity, as measured by quality-adjusted life years lost, has more than doubled from 1993 to 2008 [5]. Obesity has thus become one of the greatest public health concerns, and Asia has not been spared. The different fat distribution in Asian patients and their susceptibility to obesity-related disease at lower BMI have led to a reduction in BMI threshold to 23 kg/m2 and above for overweight and 27.5 kg/m2 and above for obesity [6]. For obese individuals, bariatric surgery has emerged as the most effective and viable tool for sustainable weight loss [7, 8]. Bariatric surgery has significantly decreased overall mortality with a marked survival advantage [9, 10]. The growth of the laparoscopic approach to bariatric surgery has made it more acceptable to patients in the Asia-Pacific region, prompting increased numbers of cases and making it important to audit the state of bariatric surgery [11] by answering certain basic questions regarding the number and details of bariatric procedures being performed.
Keeping this in mind, we discussed the data for bariatric surgery for the past 5 years with representative Asia-Pacific Metabolic and Bariatric Surgery Society (APMBSS) members of leading Asian countries at the 6th International APMBSS Congress held in Singapore from 21st to 23rd October 2010. We thus present a bariatric surgery audit for the past 5 years (2005–2009), with year 2004 as comparison in an Asian context based discussions during the congress.
Methods
Questionnaire
An e-mail survey, consisting of three questions (Table 1), was sent to representative APMBSS members practicing bariatric surgery in 12 Asian countries. The following procedures were queried: open and laparoscopic sleeve gastrectomy (LSG), open and laparoscopic adjustable gastric banding (LAGB), open and laparoscopic standard Roux-en-Y gastric bypass (LRYGB), laparoscopic mini-gastric bypass (LMGB), open and laparoscopic long-limb and very long-limb gastric bypass (>100 cm), open and laparoscopic biliopancreatic diversion (Scopinaro procedure), open and laparoscopic duodenal switch, open and laparoscopic vertical banded gastroplasty, intragastric balloon, electronic pacers, and others. If deemed necessary, a second e-mail was sent for further data and clarifications. The individual members (listed in the Acknowledgements) did their local survey and provided the data discussed vide infra.
Data Analysis
A tabular and graphic presentations of the data received were prepared and certain derived data were calculated. The data were collected and analyzed using SPSS software.
Results
Response Rate
Out of potential 12 APMBSS representatives of major Asian nations, there were 11 responders (91.6%). Except China, all major Asian nations responded (Table 2).
Number of Procedures
In response to the first question, the Asian total came out to 6,598 procedures during a 5-year period from 2005 to 2009, with Taiwan and South Korea performing more than 4,000 procedures in total (Table 2). These procedures were performed on 2,445 men and 4,153 women with mean age at surgery of 35.5 years (range, 18–69 years) and mean BMI of 44.27 kg/m2 (range, 31.4–73 kg/m2).
Number of Metabolic/Bariatric Surgeons
In response to the second question, the Asian total came out to be 155 surgeons (Table 2). India (n = 50) and South Korea (n = 23) have the most number of bariatric surgeons.
Types of Procedures Performed
In response to our third question, the distributions of bariatric procedures during the last 5 years, from 2005 to 2009, are shown in Table 3. The four most commonly performed procedure were LAGB (35.9%), LRYGB (24.3%), LSG (19.5%), and laparoscopic mini-gastric bypass (15.4%), respectively.
Classification of Procedures Performed
Almost all bariatric procedures were done laparoscopically (99.8%).
Type of Procedure
Fifty-eight percent of bariatric procedures were purely restrictive (AGB, SG, vertical band gastroplasty (VBG), intragastric balloon), 41% of procedures were restrictive and malabsorptive (RYGB, mini-gastric bypass, long-limb bypass), and only 1% of the procedures were primarily malabsorptive (duodenal switch, BPD; Table 3).
Asian Trends
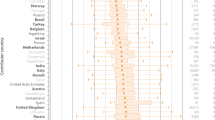
Comparing the 5-year trend from 2004 to 2009, the absolute number of procedures for all bariatric surgeries in Asia over the last 5 years increased from 381 to 2,091, an increase of 5.5 times (Fig. 1). LSG increased from 1% to 24.8% and LRYGB from 12% to 27.7%, thus a relative percentage increase of 24.8 and 2.3 times, respectively. However, LAGB and mini-gastric bypass decreased from 44.6% to 35.6% and from 41.7% to 6.7%, respectively (Fig. 2). The absolute growth rate of bariatric surgery in Asia over the last 5 years was 449%.

Total number of bariatric procedures

Trends of bariatric procedures (%)
Discussion
The Asian perspective of bariatric surgery was first discussed in the 1st Asia-Pacific Bariatric Consensus Meeting held in Taipei, 27 February 2005, by the Asia-Pacific Bariatric Surgery Group (APBSG) founded in Seoul, Korea, on October 6, 2004 [12]. It was found that bariatric surgery in Asia has undergone a paradigm shift since Taiwan performed the first bariatric surgery, Jejuno ileal bypass in the 1970s, followed by VBG in 1981. Laparoscopy in the form of LVBG was first started in 1998 in Taiwan, followed by the first LAGB in Singapore in 1999 and LRYGBP and LMGB in Taiwan in 2000 and 2001, respectively [12]. The 2005 APBSG Consensus Meeting modified the indication for bariatric surgery for Asian people to: obese patients with BMI > 37, obese patients with BMI > 32 with the presence of diabetes or two significant obesity-related comorbidities, patients unable to lose or maintain weight loss by dietary or medical measures, and patients >18 and <65 years of age. LAGB and LRYGB were the two most common procedures performed at that time in Asia.
This survey reports the recent 5-year trends of bariatric surgery in Asia from 2005 to 2009 and documents the number and types of bariatric procedures being performed. The data obtained from individual APMBSS representatives of the leading Asian countries were discussed and clarified at the 6th International APMBSS Congress held in Singapore. Overall, there was a 5.5 times increase in bariatric surgery with an increase in LSG and LRYGB procedures, but a decrease in LAGB and mini-gastric bypass procedures. Considering the absolute numbers, the total number of procedures being performed has increased from 381 in 2004 to 2,091 in 2009 (Fig. 1 and Table 4), an absolute growth rate of 449%. The percentage of adjustable gastric banding decreased from 44.6% in 2004 to 35.6% in 2009. This may be because of the failure of gastric banding to produce the desired long-term weight loss and associated complications like erosion, ulceration, and band migration. Moreover, the gastric band needs frequent adjustments, requiring multiple visits incurring cost and lifelong follow-up not welcomed by patients [13, 14]. LSG increased from 1% in 2004 to 24.8% in 2009. The rise in the number of sleeve gastrectomies that is seen in Asia parallels global trends [15]. The reason for this may be because of the ease and speed of this procedure compared with other bariatric procedures and no foreign body and good early results [16]. Long-term follow-up data may, however, influence the popular appeal for this procedure. LRYGB has increased in number and mini bypass has decreased. Compared with global trends, it is seen that in USA/Canada, LRYGB is losing its fame and LAGB is again gaining popularity, whereas in Europe the trend parallels Asia with an increase in LRYGB and a decrease in LAGB [15].
The main weakness of this survey is that data from China were not available. Due to the nature of the survey, as opposed to a registry, the data provided may be incomplete. Despite missing data, the clear trends indicate a significant rise in bariatric surgical procedures in Asia. The survey appears to be representative, with a response rate of 91.6% and 11 out of 12 APMBSS member representatives, except China, responding. To increase the accuracy and reliability of the data, it is important to establish a registry with compliance from all representative APMBSS surgeons of all Asian nations practicing bariatric surgery.
References
Popkin BM, Doak CM. The obesity epidemic is a worldwide phenomenon. Nutr Rev. 1998;56:106–14.
World Health Organization. Obesity and overweight. 2011. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/index.html. Cited 16 April 2011.
Haslam DW, James WP. Obesity. Lancet. 2005;366:1197–209.
Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg. 2004;14:1157–64.
Jia H, Lubetkin EI. Obesity-related quality-adjusted life years lost in the U.S. from 1993 to 2008. Am J Prev Med. 2010;39:220–7.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–63.
National Institutes of Health. Gastrointestinal surgery for severe obesity. National Institutes of Health Consensus Development Conference Draft Statement. Obes Surg. 1991;1:257–66.
Buchwald H, Avidor Y, Braunwald E, et al. A systematic review and meta-analysis. JAMA. 2004;13:1724–37.
Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240:416–24.
Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199:543–51.
World Health Organization. Obesity and overweight. 2003. Available from: http://www.who.int/hpr/NPH/docs/gs_obesity.pdf. Cited 16 April 2011.
Lee WJ, Wang W. Bariatric surgery: Asia-Pacific perspective. Obes Surg. 2005;15:751–7.
Shen R, Dugay G, Rajaram K, et al. Impact of patient follow-up on weight loss after bariatric surgery. Obes Surg. 2004;14:514–9.
Ganesh R, Leese T, Rao AD, et al. Laparoscopic adjustable gastric banding for severe obesity. Singapore Med J. 2006;47:661–9.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide: 2008. Obes Surg. 2009;19:1605–11.
Moy J, Pomp A, Dakin G, et al. Laparoscopic sleeve gastrectomy for morbid obesity. Am J Surg. 2008;196:e56–9.
Acknowledgments
We thank the following individuals and individual country obesity surgical societies for providing the data for this survey: India—Pradeep Chowbey and Muffazal Lakdawala; Indonesia—Barlian Sutedja; Hong Kong—Simon K.H. Wong; Japan—Seigo Kitano; Malaysia—Chin Kin Fah; Philippines—Hildegardes C. Dineros; Singapore—Andrew Wong, Anton Cheng and Shanker Pasupathy; South Korea—Sang Kuon Lee; Taiwan—Wei-Jei Lee and Chih-Kun Huang; Thailand—Paisal Pongchairerks; Vietnam—Tran Binh Giang.
Disclosure
All authors declare that they have no competing interest and no relevant financial interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s11695-011-0566-z.
Rights and permissions
About this article
Cite this article
Lomanto, D., Lee, WJ., Goel, R. et al. Bariatric Surgery in Asia in the Last 5 Years (2005–2009). OBES SURG 22, 502–506 (2012). https://doi.org/10.1007/s11695-011-0547-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0547-2