
Abstract
Background
The aim of this study was to analyze the impact of bariatric surgery on the body composition of patients suffering from class III obesity at different postoperative time intervals.
Methods
The body composition of 114 patients undergoing Roux-en-Y gastric bypass surgery was measured prior to surgery (T0) and then 30 (T30) and 180 (T180) days following surgery. Body composition was evaluated using the following parameters: total body mass, body mass index, excess weight, percentage of excess weight loss, relative body fat (%F), lean body mass (LBM), and fat tissue mass (FTM). To determine these variables, validated formulas and equations proper to obese men and women were employed.
Results
A significant reduction in %F (41.5%), LBM (20.3%), FTM (37.9%) was noted at each time interval (p ≤ 0.01).
Conclusions
Bariatric surgery proved to be effective in reducing total body mass and body fat at every time interval. However, dietary measures emphasizing adequate protein intake may be implemented in order to reduce loss of LBM and, coupled with frequent physical activity, may help curtail the impact the surgery has on morphological variables.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity is regarded as a public health problem and is defined as being the excessive accumulation of body fat to the point of harming a person's health [8, 40], leading to cardiovascular disease, dyslipidemia, diabetes, and certain types of cancer [1]. According to the Brazilian Institute of Geography and Statistics [10], 49% of the Brazilian population is overweight and 14.8% has been diagnosed as being obese.
Class III obesity, defined by a body mass index (BMI) over 40 kg/m², is considered one of the diseases with the highest mortality rate in the world—12 times higher in people between 25 and 40 years old, when compared to the non-obese [7]. Our findings show that over the last decade, prevalence of the class II obesity group has grown the most. These findings match those of research performed in Canada, where a 225% increase in obesity was noted over a period of 13 years [13].
According to the National Institute for Health and Clinical Excellence [23] and the National Institute of Health [24], in patients suffering from class III obesity for whom conservative treatment proved ineffective, surgery is the best option for achieving and maintaining weight loss over the long term.
Bariatric surgery is now regarded as the most effective way of controlling class III obesity. The outstanding benefits of this procedure are long-term weight loss and maintenance, recovery from excess weight-related illnesses, improvement and understanding of proper eating habits, and a subsequent improvement in quality of life [27, 38, 39]. The impact of surgery on patients' health also, directly or indirectly, brings down the cost of health care [38].
Of the techniques currently practiced, laparoscopic Roux-en-Y gastric bypass (RYGBP) is considered to be the gold standard in bariatric surgery, for being highly effective and having a low mortality rate.
Patients who undergo RYGBP show a 65% to 80% loss in excess weight over a 12- to 18-month postoperative period [33, 37]. These changes are the result of a calorie deficit, low protein intake, and quick weight loss, with patients who undergo bariatric surgery likely to see changes in body composition over the course of treatment.
The aim of this study was to investigate the impact this procedure has on body composition in class III obesity patients over a period of 6 months following RYGBP.
Material and Methods
We studied 19- to 60-year-old patients suffering from class III obesity [45] who underwent RYGBP at a private hospital in Rio de Janeiro and were treated and cared for by a multidisciplinary team at the hospital. We performed testing during the preoperative period (T0), 30 days (T30) post surgery and 180 days (T180) post surgery. This study contains exploratory analysis carried out using a thorough and in-depth approach developed by the Federal University of Rio de Janeiro's Nucleo de Pesquisa em Micronutrientes/Nucleus of Micronutrient Research [25]. All the patients signed a consent form in order to take part in the project, and the study has the approval by the Research Ethics Committee from Clementino Fraga Filho University Hospital (Research Protocol # 011/06–CEP).
Anthropometric assessment adhered to the norms set forth by the International Society for Advancement in Kinanthropometry [26], and the following measurements were taken: total body mass (TBM), obtained using an electronic platform scale with a capacity for up to 300 kg (Filizola, 100 g), with the patients shoeless and lightly dressed; and height was taken using a Lange® stadiometer, with the patients shoeless and in orthostatic state [29]. BMI was then measured according to the cut-points established by the WHO [45]. The patients were sorted into subclasses of 5 kg/m2 BMI intervals, yielding four groups between 40 and 60 kg/m2.
To calculate ideal weight (IW), the following formula specifically for class III obese patients who have undergone bariatric surgery [5] was used:
Excess weight (EW) was calculated according to the formula [5]:
The percentage of excess weight loss (%EWL) was established according to the formula: \( \% {\text{EWL}} = \left( {100 \times {\text{weight}}\;{\text{loss}}} \right)/{\text{EW}} \).
Abdominal circumference was measured using a Sanny® flexible and nonextendable 200-cm measuring tape accurate to the 0.1 cm and was obtained by averaging measurements taken at two different points on the abdomen with the patient in orthostatic state and after exhaling normally [17]: measurement 1, laterally from the midpoint between the last rib and the iliac crest to the midpoint between the xiphoid process and the umbilicus; measurement 2, laterally from iliac crest level to the navel.
To circumvent the difficulty of accommodating obese persons (particularly the class III obese) in body composition measurement equipment, such dual energy x-ray absorptiometry, magnetic resonance imaging, and CT scan equipment, we used Weltman regression equations [43, 44] for determining fat percentage (%F), fat tissue mass (FTM), and lean body mass (LBM) based on average waist circumference, TBM, and height measurements (Table 1), which closely correlate to hydrostatic weighing [4] and are more affordable and readily available, making them accessible in underfunded places.
Statistical analysis was carried out using SPSS (Statistical Package for the Social Sciences) version 13.0 for Windows, with a descriptive breakdown of the group under study and checking the relationship between the variables TBM, BMI, EW, %EWL, %F, FTM, LBM and follow-up times by measuring central tendency, dispersion, minimum and maximum values for continuous variables, and frequency tables for categorical variables. In comparing continuous data between two groups, we used the Mann–Whitney test; and to explain measurement variation over time, we did analysis of variance (ANOVA). The significance level we adopted was p ≤ 0.05.
Results
The sample group was composed of 114 patients—28 (24.6%) of them were male and 86 (75.4%) were female. Average age was 36.9 ± 11.6 years old, varying from 19 to 60 years of age with 57.9% in the 31- to 50-year-old sample group (Table 2).
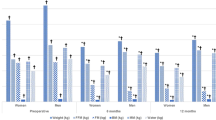
Analysis of the sample group revealed a 35-kg drop in ponderal index over the 180-day postoperative period. Percent EWL was 24.95 and 58.95 kg at 30 and 180 days post surgery, respectively. At T0, patient average BMI was 44.26 ± 5.03 kg/m2. At T30 and T180, average BMI was 38.95 ± 4.64 and 31.65 ± 4.16 kg, respectively. A significant difference (p ≤ 0.01) was noted between the variables TBM and BMI over the three periods of testing (Table 3).
Patient body composition was found to have a %F of 48.76% at T0, progressing to 45.83% and 41.49% at T30 and T180, respectively. Average TBM was 58.41 ± 9.28, 49.29 ± 8.72, and 36.40 ± 7.41 kg at T0, T30, and T180, respectively. A drop was also noted when comparing pre- and postoperative LBM—64.43 ± 16.69, 58.54 ± 13.64, and 51.39 ± 10.94 kg. There was a significant difference (p ≤ 0.01) in the variables %F, FTM, and LBM over the three periods when data was recorded (Table 4).
Discussion
Average age of the sample group was 36.9 ± 11.6 years. This data was similar to that collected by Ogden et al. [27], showing a high prevalence of class III obesity among those between 20 and 39 years of age. We found women to have the highest rate of obesity, at 75.4%.
In Brazil, according to the IBGE [10], approximately 50.1% of the male and 48% of the female population have been diagnosed as carrying excess weight, while 12.5% of the male population and 16.9% of the female population was diagnosed as obese. The frequency of both excess weight and obesity increased with age up to the 45- to 54-year-old age range in men and the 55- to 64-year-old age range in women and dropping off in the later age groups, suggesting it has a major impact on public health.
In assessing the rising rate of obesity in Brazil over the last 34 years, since the first study of its kind in 1974–1975, the prevalence of obesity has increased fourfold among men (from 2.8% to 125%) and twofold among women (from 8.0% to 16.9%), while the fact there is data showing the prevalence of obesity has risen across the board is noteworthy, with every socioeconomic group, in urban and rural settings, male and female all showing rising rates of obesity [10].
Average TBM taken at T0 was 122.81 ± 19.81 kg, with average ponderal loss of 35.0 kg at T180. These findings are similar to those of Mônaco et al. [20], where 90 patients undergoing gastric bypass were evaluated and found to have average TBM of 128.22 ± 28.62 kg during the preoperative period and average weight loss of 34.0 kg 6 months post surgery.
MacLean et al. [18] classifies bariatric surgery as being unsatisfactory if patients show ponderal losses under 25% of their preoperative weight; satisfactory when 25% of their preoperative weight is lost; and good when they weigh within 30% of their ideal weight.
The patients we studied saw 11.8% and 28.5% weight loss at T30 and T180, respectively. Surgery could thus be classified as having been satisfactory. These results corroborate the findings of Santos et al. [32], where a 30.4% loss in weight was documented during a period of 6 to 11 months post surgery.
Patient BMI was found to average 44.26 ± 5.03 kg/m2 at T0, a nutritional state classified as being class III obesity by the WHO [45]. At T30 and T180, average BMI was 38.95 ± 4.64 and 31.65 ± 4.16 kg, respectively, showing the patient outlook to have improved to obesity classes II and I, respectively. Our findings pertaining to decreases in BMI are similar to those of Velasco and Haberle [42], who studied weight loss following gastric bypass surgery.
Average excess weight at T0 was 60.61 ± 16.15 kg. Thirty and 180 days following surgery, %EWL was 24.95% and 58.95%, respectively. Skroubis et al. [35] found a similar %EWL value of 53.6% 6 months post surgery, contrasting with other existing research, where %EWL was reported to be 61.2% 180 days after surgery [21, 34]. A 160-patient study carried out in Brazil found %EWL to be 61.2% after 6 months post surgery [6].
Bariatric surgery can be justified largely for its impact on comorbidities associated with obesity. A slight drop in weight is enough to have a positive effect on type 2 diabetes, hypertension, and dyslipidemia [2, 11]. Along the same lines, a 10% drop in weight leads to better long-term control of these same conditions [15].
Patient body composition showed %F of 48.76% at T0, progressing to 45.83% and 41.49% at T30 and T180, respectively. Average FTM at T0, T30, and T180 was 58.41 ± 9.28, 49.29 ± 8.72, and 36.40 ± 7.41 kg, respectively. Percent FTM was found to drop from 15.5% at T30 to 37.9% at T180, respectively
A drop in LBM between pre- and postoperative periods was also observed, with 64.43 ± 16.69, 58.54 ± 13.64, and 51.39 ± 10.94 kg recorded on the three testing periods. The percentage of LBM loss recorded at T30 was 9.4% and at T180, 20.3%.
According to Hill et al. [9], large drops in weight are usually followed by a significant drop in basal metabolic rate (BMR), to the tune of hundreds of kilocalories. Hypocaloric diets often prescribed post surgery boost proteolysis to meet metabolic demands, which explains the drop in LBM. When this reduced dietary intake is not followed by physical exercise, which among other benefits boosts resting metabolic rate and stimulates protein synthesis [36, 3], BMR drops by 15% to 30%, making it harder to maintain body composition in the long term [30].
In a study where stable isotope techniques (40 K) were used to evaluate 82 patients following bariatric surgery, an 18% drop in lean mass and 82% drop in fat was found to have occurred over the first postoperative trimester [28]. van Gemert et al. [41] found a 20–30% loss in lean mass by the end of the first year post surgery. Adipose tissue accounted for between 70% and 80% of total weight loss.
At the end of the first postoperative year, greater protein intake is conducive to the weight lost being primarily in fat. By the same token, physical activity can speed up weight loss and preserve LBM. Individuals who undergo bariatric surgery and follow up with physical exercise see gains of 15% LBM, while those who remain sedentary lose 11% LBM by the end of the first year of observation. The practice of physical exercise thus was a determining factor in the drop in body weight and gains in LBM [19].
Information as to how %F and FTM are more direct indicators of the gravity of obesity than BMI [22] has generated interest in the medical community, as has the revelation that the likelihood of premature death is inversely proportional to gains in FTM and reductions in LBM [12, 31] Furthermore, a significant drop in LBM results in a drop in basal metabolic rate [14], which deserves attention during postoperative nutritional follow-up, given how adequate protein intake and recommending physical exercise may curb the negative effects of a carbohydrate-restrictive diet and play an important role in the maintenance or gains of lean muscle mass that physical activity provokes [16, 36].
Conclusion
Bariatric surgery proves to be effective in achieving absolute weight loss and reducing fat tissue. However, dietary measures emphasizing adequate protein intake should be undertaken to minimize the loss of LBM and, coupled with regular physical activity, may curtail the impact the operation has on morphological variables.
References
Bender R, Zeeb H, et al. Causes of death in obesity: relevant increase in cardiovascular but not in all-cancer mortality. J Clin Epidemiol. 2006;59:1064–71.
Busseto L, Pisent C, Rinaldi, et al. Variation in lipid levels in morbidly obese patients operated with the Lap-Band® adjustable gastric banding system: effects of different levels of weight loss. Obes Surg. 2000;10:569–77.
Ciolac EG, Guimarães GV. Exercício físico e síndrome metabólica. Rev Bras Med Esporte. 2004;10(4):319–24.
Das SK. Body composition measurement in severe obesity. Curr Opin Clin Nutr Metab Care. 2005;8(6):602–6.
Deitel M. Overweight and obesity worldwide now estimated to involve 1.7 billion people. Obes Surg. 2003;13:329–30.
Faria OP, Pereira VA, Gangoni CMC, et al. Obesos mórbidos tratados com gastroplastia redutora com bypass gástrico em Y de Roux: análise de 160 pacientes. Brasília Méd. 2002;39(1/4):26–34.
Freedman DS, Khan LK, Serdula MK, et al. Trends and correlates of class 3 obesity in the United States from 1990 to 2000. JAMA. 2002;188:1758–61.
Halpen A. Fisiologia da Obesidade. In: Garrido Júnior AB, Ferraz EM, Barroso FL, et al., editors. Cirurgia da obesidade. São Paulo: Ed. Editora Atheneu; 2003. p. 9–12.
Hill JO, Sparling PB, Shields TW, et al. Effects of exercise and food restriction and body composition and metabolic rate in obese women. Am J Clin Nutr. 1987;46:622–30.
Instituto Brasileiro de Geografia e Estatística—IBGE. Pesquisa de Orçamentos Familiares 2008–2009: Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil. Rio de Janeiro: Ministério do Planejamento, Orçamento e Gestão/IBGE; 2010.
Inge TH, Xanthakos SA, Zeller MH. Bariatric surgery for pediatric extreme obesity: now or later? Int J Obese (Lond). 2007;31:1–14.
Jackson AS, Stanforth PR, Gagnon J, et al. The effect of sex, age and race on estimating percentage body fat from body mass index: the heritage family study. Int J Obes. 2002;26:789–96.
Katzmarzyk PT, Mason C. Prevalence of class I, II and III obesity in Canada. CMAJ. 2006;174(2):156–7.
Karhunen L, Franssila-Kallunki A, Rissanen A, et al. Determinants of resting energy expenditure in obese non-diabetic Caucasian women. Int J Obes, London. 1997;21:197–202.
Kuhlmann HW, Falconi RA, Wolf AM. Cost-effective bariatric surgery in Germany today. Obes Surg. 2000;10:549–52.
Liou YM, Liou TH, Chang LC. Obesity among adolescents: sedentary leisure time and sleeping as determinants. Journal of Advanced Nursing. 2010;66(6):1246–56.
Loghman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Abridged edition, 1988;90
Maclean LD, Rhode BM, Shizgal HM. Gastroplasty for obesity. Surg Gynecol Obstet. 1981;153(2):200–8.
Metcalf B, Rabkin RA, Rabkin JM, et al. Weight loss composition: the effects of exercise following obesity surgery as measured by bioelectrical impedance analysis. Obes Surg. 2005;15:183–6
Mônaco DV, Merhi VAL, Aranha N, et al. Impacto da cirurgia bariátrica tipo capella modificado sobre a perda ponderal em pacientes com obesidade mórbida. Rev Ciênc Méd Campinas. 2006;15(4):289–98.
Muscelli E, Mingrone G, Camastra S, et al. Differential effect of weight loss on insulin resistance in surgically treated obese patients. Am J Med. 2005;118(1):51–7.
Nagaya T, Yoshida H, Takahashi H, et al. Body mass index (weight/height2) or percentage body fat by bioelectrical impedance analysis: which variable better reflects serum lipid profile? Int J Obes. 1999;23:771–4.
National Collaborating Centre for Primary Care. Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children. London: National Institute for Health and Clinical Excellence; 2006. p. 2590.
National Institute of Health Consensus Development Conference Statement. Gastrointestinal surgery for morbid obesity. Am J Clin Nutr. 1992;55(2):615s–9s.
Neves CE, Saboya C, Pereira SE, et al. Impact of bariatric surgery on morphological variables in the morbidly obese. FIEP Bulletin. 2007;77:692–4.
Norton K, Olds T. Antropometrica. Rosário: Biosystem Servicio Educativo; 2000.
Ogden J, Clementi C, Aylwin S, et al. Exploring the impact of obesity surgery on patients health status: a quantitative and qualitative study. Obes Surg. 2005;15(2):266–72.
Palombo JD, Maletskos CJ, Reinhold RV, et al. Composition of weight loss in morbidly obese patients after gastric bypass. J Surg Res. 1981;30(5):435–42.
Ramalle-Gómara E, Lozano DM, Hernando AB, et al. Validez de lãs medidas autodeclaradas de peso y talla en la estimación de la prevalencia de obesidad. Med Clin. 1997;716:108.
Ravussin E, Lillioja S, Knowler W, et al. Reduced rate of energy expenditure as a risk factor for body-weight gain. N Engl J Med. 1988;318:467–72.
Residori L, Garcia-Lorda P, Flancbaum L, et al. Prevalence of co-morbidities in obese patients before bariatric surgery: effect of race. Obes Surg. 2003;13:333–40.
Santos EMC, Burgos MPA, Silva SA. Perda ponderal após cirurgia bariátrica de Fobi-Capella: realidade de um hospital universitário do nordeste brasileiro. Rev Bras Nutr Clin. 2006;21(3):188–92.
Shah M, Simha V, Garg A. Review: long term impact of bariatric surgery on body weight, comorbidities, and nutritional status. J Clin Endocrinol Metabol. 2006;91(11):4223–31.
Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683–93.
Skroubis G, Sakellaropoulos G, Pouggouras K, et al. Comparison of nutritional deficiencies after Roux-en-Y gastric bypass and after biliopancreatic diversion with Roux-en-y gastric bypass. Obes Surg. 2002;12:551–8.
Stiegler P, Cunliffe A. The role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss. Sports Med. 2006;36(3):239–62.
Sugarman HJ. Bariatric surgery for severe obesity. J Assoc Acad Minor Phys. 2001;12(3):129–36.
Suter M, Giusti V. Surgical options of obesity treatment: results and complications. Rev Med Suisse. 2005;1(12):832–6.
Szego T, Mendes CJL, Bitran A. Derivaçao gastrojejunal por laparoscopia com e sem anel. In: Garrido Jr AB, editor. Cirurgia da obesidade. Sao Paulo: Atheneu; 2002. p. 189–96.
USDA (US Department of Agriculture). Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans. 2010
van Gemert WG, Westerterp KR, van Acker BA, et al. Energy, substrate and protein metabolism in morbid obesity before, during and after massive weight loss. Int J Obes Relat Metab Disord. 2000;24:711–8.
Velasco MN, Haberle TS. Tratamiento cuirúrgico de la obesidad mórbida. Rev Chil Cir. 2003;55(2):155–9.
Weltman A, Levine S, Seip R, et al. Accurate assessment of body composition in obese females. Am J Clin Nutr. 1988;48:1179–83.
Weltman A, Levine S, Seip R, et al. Practical assessment of body composition in adults males. Hum Biol. 1987;59(3):523–35.
WHO (World Health Organization). Obesity: preventing and managing the global epidemic. Report of WHO consultation on obesity. Geneva: World health organization; 1998.
Acknowledgments
We would like to thank Professor Maria das Graças Tavares do Carmo (INJC/UFRJ) for her cooperation, without which this article would not be possible. L. A. Aquino receives a grant for technical assistance from the National Council for Scientific and Technological Development (CNPq proc. 371704/2008-1).
Conflict of interest statement
LA Aquino, SE Pereira, JS Silva, CJ Saboya, and A Ramalho declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
de Aquino, L.A., Pereira, S.E., de Souza Silva, J. et al. Bariatric Surgery: Impact on Body Composition After Roux-en-Y Gastric Bypass. OBES SURG 22, 195–200 (2012). https://doi.org/10.1007/s11695-011-0500-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0500-4