
Abstract
There is no standardized definition of “weight loss success” after bariatric surgery. The current study was designed to evaluate if various patient factors differed between those with successful and unsuccessful weight loss; and if these findings varied depending upon which definition of weight loss success was used. A chart review of psychiatric and medical files was conducted for 110 patients who had Roux en-Y Gastric Bypass and at least 1 year of follow-up data. Data were analyzed for four weight loss success criteria: body mass index (BMI) < 30 kg/m2 (n = 60 patients), BMI < 35 kg/m2 (n = 86), ≥70% excess weight loss (EWL; n = 75), and ≥ 50% EWL (n = 103). For each success criterion, we examined the differences in demographics, physical co-morbidities, and psychological conditions before surgery and behavioral noncompliance after surgery between patients who had and had not achieved successful weight loss. Weight loss success rates with these patients ranged from 55% to 94%, depending upon which criterion was used. Having sleep apnea before surgery differentiated successful and unsuccessful patients when using BMI < 30 kg/m2 and ≥70% EWL only. A success criterion of ≥50% EWL can be used for any patient, although a more stringent definition of success (BMI < 30 kg/m2) could be used for patients with BMI 40-50 kg/m2. Future research should be done to examine how patient health and behavior predicts differing definitions of weight loss success.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is associated with higher rates of mortality among adults, with an estimated 300,000 deaths a year in the US alone [1]. In 2004, the prevalence of obesity reached 28-33%, representing 72 million obese adults [2], 5% of whom were severely obese (body mass index (BMI) 40 kg/m2; [3]). The prevalence of severe obesity may be misleading as the number of these adults increased by as much as 75% from 2000 to 2005 [4]. The medical community has now turned to bariatric or gastric bypass surgery as a viable option for weight loss in the severely obese [5]. By 2020, it is estimated that up to 13% of the US population will be eligible for bariatric surgery (BMI ≥ 40 m/kg2). In addition, bariatric surgery is gaining popularity as a treatment for severe type 2 diabetes mellitus (T2DM) in people with a BMI of ≥35 kg/m2 [6, 7]. The American Society for Metabolic and Bariatric Surgery reported that the number of surgeries nearly doubled from 2003 to 2007 (103,000-205,000). Given these statistics, there may be over one million people who have undergone bariatric surgery by 2020 [8].
We recently published findings describing how psychological and physical health, behavioral compliance, and demographic factors before and after gastric bypass surgery were related to weight loss [9]. As part of the literature review for this work, we found that “weight loss success” had been operationalized in a variety of ways including movement from obesity (≥30 kg/m2) to overweight (<30 kg/m2) [10], movement from class II/III obesity (≥35 kg/m2) to class I obesity or less (<35 kg/m2) [11], achieving ≥40% excess weight loss (EWL) [12, 13], achieving ≥50% EWL [14], and achieving ≥70% EWL [15]. Investigators would then examine how a number of demographic, health, and insurance factors predicted this arbitrarily chosen definition of “weight loss success”. Not surprisingly, different factors were found to be important in each investigation. It is difficult to conclude whether these are true differences or they are simply a result of using different criteria for defining “weight loss success”.
The current study was designed to evaluate if psychological and physical health before surgery, behavioral compliance after surgery, and demographic factors differed between patients with successful and unsuccessful weight loss; and if these results varied depending upon which definition of weight loss success was used. These findings may be used to recommend a more standardized definition of “weight loss success” after gastric bypass and to encourage others to examine various metrics of “weight loss success” in their own studies when trying to predict whether or not a set of patients are more or less likely to be successful.
Methods
This study was part of a larger investigation, the details of which have been published elsewhere [9]. For the current study, data were obtained from a retrospective chart review of gastric bypass patients in a Scripps Clinic Center for Weight Management program who had surgery between January 1997 and December 2002. Patients’ medical and mental health records were examined and information on relevant variables was abstracted onto chart review forms and then entered into an electronic spreadsheet. Data abstraction was done by the second author and any ambiguous information was resolved with the last author who was the attending physician for all patients. Diagnoses for a mental or physical health condition were taken directly from the chart. No diagnosis was entered onto the chart review form unless it was noted by the physician in the patient’s chart. All study procedures were approved by the Institutional Review Board for Human Subjects at Scripps Clinic.
Patient Care
All patients were seen by the same medical team throughout their treatment. This included the last author (a physician), a psychologist, a registered dietitian, and the bariatric surgeon. All patients had three appointments before surgery (−12 months, −6 months, and just prior to surgery) with the treatment team (the surgeon only saw patients once right before surgery). After surgery, patients had regular appointments with the last author (+1 month, +3 months, +6 months, +12 months, +18 months, and +24 months) and two appointments with a dietitian and two with a psychologist.
During visits with the second author, all patients were asked about their exercise behaviors, diet behaviors, medical complaints, and existing medical conditions. Following surgery, questions were added regarding vomiting, nausea, specific diet restrictions (i.e., not drinking soda or large quantities of liquids, not eating foods high in carbohydrates and fats), and any other symptoms of surgical complications.
At the time of surgery, each patient underwent an extensive screening process to determine if patients were physically and psychologically prepared for surgery. Psychological assessment consisted of a 90-min semi-structured interview. During this interview, the eating disorders portion of the Structured Interview for DSM-IV (SCID-I) was administered as well as the Million Behavioral Medicine Diagnostic Test (Pearson Assessments) and the Beck Depression Inventory (BDI II; Harcourt Assessments).
Study Population
Exclusion criteria for the study were patients with a revisional procedure and patients with procedures other than Roux en-Y Gastric Bypass (RYGBP). Revisional procedures were excluded because many of the patients had considerable weight loss already and we did not have access to their pre-surgical information. Patients with banding procedures were excluded because of the varying weight loss patterns and results compared to patients with RYGBP [16]. Both genders and all ethnicities were included in the study. We chose a minimum of 1 year follow-up based upon the shortest follow-up period reported in previous studies of weight loss success [12, 13, 15].
Study Variables
Height, Weight, and BMI
The main dependant variables measured in the medical charts were body weight and height. These were then used to calculate BMI (kg/m2) and percent of excess weight loss (%EWL) based on the recommendations of Bray and colleagues [17].
Demographics
Demographic variables included education, age, socioeconomic status (SES), gender, and ethnicity. Education was self-reported as total years of schooling completed as well as categorized into levels of schooling completed (elementary school, middle school, high school, and post-graduate). Ethnicity was dichotomized into white versus non-white due to the small sample size of ethnic minorities in the study. Occupation descriptions and education were used to create an SES score with the validated Hollingshead four-factor index of social status [18]. To calculate SES, years of education was multiplied by three and job classification was multiplied by five and then these quantities were summed, resulting in score ranging from 8 (unskilled workers) to 66 (professionals and proprietors of large buisnesses).
Co-morbid mental health
Axis I disorders included all mood disorders, such as depression and anxiety, as well as eating disorders, such as anorexia, bulimia, binge eating, purging, emotional eating, compulsive overeating, and eating disorders not otherwise specified. For the purposes of this investigation, eating disorders were separately analyzed from other axis I disorders such as depression and anxiety because of the importance of eating disorders to the etiology of severe obesity [19]. They were coded as either present or absent. Continuous variables were also created for the total number of axis I diagnoses (separate from eating disorders) and total number of eating disorders for each participant.
In addition to the axis I diagnosis, history of abuse—physical and sexual—was coded as a separate mental health category. Based upon the literature, abuse history was separated into sexual or physical and coded as present or absent for analyses [20, 21].
Co-morbid physical health
Physical-health conditions were noted based upon diagnosis of co-morbid conditions and medication utilization. Participants were only coded as having a disorder if they were receiving treatment for the condition as noted in the medical charts. Co-morbid conditions were selected based on the literature and their associations with severe obesity [22], and were analyzed in the following categories: cardiovascular disorders, metabolic (diabetes) type disorders, digestive disorders, cancer, hormonal disorders, physical activity-limiting disorders, fibromyalgia, and sleep apnea. Each disorder variable was coded as present or absent for data analyses. A continuous variable was also created as the total number of co-morbid conditions for each participant.
Behavioral Compliance
Compliance was operationalized for this study as the necessary steps or behaviors a patient had to adhere to in order to finish any treatment plan or health-improvement strategy. As mentioned, all patients had the same treatment team who designed these treatment plans. Any incomplete compliance data were due to the patient missing his/her appointment. A total of 156 different types of noncompliance issues were identified from patient records (as noted in the chart by the second author) and were reduced to four major categories based upon work conducted by the second and third authors [23, 24]. These categories were exercise adherence, weight loss plan adherence, medication adherence, missed appointments, and poor food choices. These categories have also been used in other studies to create composite scores across a wide range of behaviors and conditions [25, 26]. Examples of specific behaviors within these categories can be found elsewhere [9]. Each compliance category was assessed before surgery and after surgery. Noncompliance issues were coded as present or absent for data analyses.
Statistical Analysis
Data analyses were done with SPSS statistical software, version 11.5. We present data analyses for four weight loss success criteria: achieving BMI < 30 m/kg2, achieving BMI < 35 m/kg2, achieving ≥50% EWL, and achieving ≥70% EWL for comparison. These weight loss success criteria were chosen because they were the most commonly used in the literature and are often used in clinical practice [8, 11, 14, 15]. Study variables are presented in four categories: demographics, physical co-morbidities before surgery, psychological conditions before surgery, and behavioral noncompliance in the first 6 months and the second year after surgery.
For each success criterion, we examined the differences in demographics, physical co-morbidities before surgery, psychological conditions before surgery, and behavioral noncompliance between successful and unsuccessful patients. T tests were used for continuous variables and chi-square for categorical variables. Because of the exploratory nature of these analyses, a Bonferroni adjustment was made for the number of paired comparisons made within a success criterion for each category of variables. For demographics and physical co-morbidities, the alpha level was adjusted to 0.008 (0.05/6); for psychological conditions it was adjusted to 0.006 (0.05/9); and for compliance to 0.004 (0.05/12).
Results
Participants
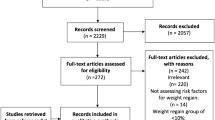
A total of 172 charts were reviewed. Using the exclusion criteria, 13 patients had either revisional procedures or procedures other than RYGB. Of these patients, 110 had at least 1 year of follow-up data. Patients who were excluded from analyses because they had procedures other than RYGB were significantly older than those who had RYGB (50.1 vs. 43.5 years old; p = 0.04), but did not differ with respect to SES, gender, ethnicity, or BMI at the time of surgery. Patients who were excluded from analyses because they had less than 1 year of follow-up were more likely to be male (63% vs. 85%; p = 0.02) than those with at least 1 year of follow-up, but did not differ with respect to age, SES, ethnicity, or BMI at the time of surgery.
Demographics for the study’s participants are shown in Table 1 by weight loss success criterion. A total of 110 participants, primarily women (86%) and white (80%), were used for the pre-surgery descriptive statistics. The participants’ average age at the time of surgery was 44.4 (SD = 10.6) years, and they had an average of 14 (SD = 2) years of school completed. Most participants had either a high school/GED (31%) or some college education (55%). The mean SES was 42 (SD = 14), indicating upper middle class participants with mostly managerial or professional occupations. The average BMI at time of surgery for this sample of patients was 49.47 kg/m2 (SD = 7.68). The lowest average BMI after surgery was 30.19 kg/m2 (SD = 6.19) which occurred an average of 21 months (SD = 10) post-surgery. Finally, participants were followed for an average of 32 months (SD = 12) with a range of 12-48 months.
Weight Loss Success
The weight loss success rates for the various criteria were as follows: 55% (n = 60) for BMI < 30 kg/m2, 78% (n = 86) for BMI < 35 kg/m2, 68% (n = 75) for ≥70% EWL, and 94% (n = 103) for ≥50% EWL. For all criteria except 50% EWL, BMI was significantly lower at baseline for successful patients in comparison to unsuccessful patients (p < 0.001). There were no differences in age, gender, ethnicity, SES, and months of follow-up between unsuccessful and successful patients for any of the criteria.
Tables 2, 3, and 4 show the physical co-morbidities, psychological conditions, and compliance data, respectively, for all patients by weight loss success criterion. The only differences between patients with successful and unsuccessful weight loss were found for sleep apnea before surgery, exercise noncompliance in the second year after surgery, and dumping syndrome in the first 6 months after surgery. These differences were not seen with all success criteria. For sleep apnea, only the criteria of BMI< 30 kg/m2 (p = 0.007) and ≥70% EWL (p = 0.003) differentiated patients. A difference in exercise noncompliance was seen only for the BMI < 30 kg/m2 (p = 0.004) and for dumping syndrome it was only with the ≥50% EWL (p = 0.005).
Discussion
Weight loss success rates with this population of RYGBP mostly white, middle-aged women were different, ranging from 55% to 94%, depending upon which criterion was used to assess success. In addition, some health and compliance factors were different between patients who did or did not have weight loss success depending upon which criterion was used. Having sleep apnea before surgery differentiated successful and unsuccessful patients when using BMI < 30 kg/m2 and ≥70% EWL but not when using the other criteria. In addition, lower exercise noncompliance was seen only for patients who achieved weight loss success using the BMI < 30 kg/m2 criteria, while dumping syndrome was less likely only for patients who achieved weight loss success using the ≥50% EWL criteria. We found that BMI at the time of surgery was significantly lower for patients who achieved success using three of the four criteria.
Lower BMI, being female, better exercise adherence, and fewer problems with food intake (dumping syndrome) have all been associated with better weight loss [16, 26–29]. We are one of the first studies to find that patients who had sleep apnea before surgery were less likely to be successful with weight loss. A recent meta-analysis found that even though bariatric surgery resulted in a 71% reduction in the apnea-hypopnea index, 62% of patients had some residual API that indicated persistent sleep apnea [30]. The authors suggested that this may lead to poor weight control after surgery. The relationship between sleep apnea and weight loss success warrants further study and should be examined using different criteria for weight loss success as we have done.
There has been some debate in the medical community concerning realistic weight loss goals for bariatric patients. It has been suggested that for RYGB patients, achieving a BMI < 30 kg/m2 is unrealistic, especially for those patients starting with BMI ≥ 40 kg/m2. However, 55% of the patients in our sample achieved a BMI < 30 kg/m2. Of those who were successful using this criterion, 81% had a BMI ≥ 40 kg/m2 at the time of surgery (data not shown). Although the mean BMI was higher for patients who did not achieve a BMI < 30 kg/m2 (54 vs. 47), it may be reasonable to set this as a goal for the majority of RYGB patients. Initial BMI did not differ significantly between successful and unsuccessful patients when using the success criterion of ≥50% EWL. For extremely obese patients (BMI ≥ 50 kg/m2), this may be a much more realistic criterion for successful weight loss in RYGB patients. The ≥50% EWL criterion was relatively “easy” to achieve as 94% of all patients in our study were successful using this criterion.
This study had many limitations. Because this was an exploratory study with few a priori hypotheses, it was necessary to adjust the level of significance to reduce reporting spurious results. This in combination with a relatively small sample size (n = 110) may have decreased the statistical power to detect differences for successful and unsuccessful patients. For example, without the Bonferroni correction for multiple comparisons, successful patients using the <30 kg/m2 criterion were less likely to have a binge eating disorder before surgery (33% vs. 54%; p = 0.03) and missed appointments (8% vs. 26%; p = 0.01) than unsuccessful patients; patients with successful weight loss using the <35 kg/m2 criterion were less likely to have exercise noncompliance (30% vs. 54%; p = 0.03); and patients with ≥50% EWL success had fewer compliance issues in the 6 months after surgery when compared to those patients who were not successful using this criteria (2 vs. 3; p = 0.04). Replicating our work with targeted hypotheses and larger sample sizes is recommended.
Another limitation of our study is that we may not have examined factors that are most closely related to weight loss success. The literature is still ambiguous about a number of these factors. However, it is very likely that there are other factors such as social support that are more strongly related to how much excess weight a person loses and thus the relationship between different success criteria and these variables would be more likely to vary [31, 32]. Finally, patients who were excluded from analyses were more likely to be older and male, limiting the generalizability of our findings to these populations of RYGB patients. We also did not examine any relationships for patients with laparoscopic banding or laparoscopic gastric sleeve.
We present evidence that patient predictors of weight loss success differ slightly depending upon which criterion is used to decide success. A success criterion of ≥50% EWL can be used for any patient, regardless of BMI at time of surgery, although a more stringent definition of success (BMI < 30 kg/m2) could be used for patients with BMI 40-50 kg/m2. More work is needed to determine how different success criteria may predict resolution of chronic disease post-surgery such as type 2 diabetes mellitus and sleep apnea.
References
Flegal KM, Graubard BI, Williamson DF, et al. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861–7.
Ogden CL, Carroll MD, McDowell MA, et al. Obesity among adults in the United States—no statistically significant chance since 2003-2004. NCHS Data Brief. 2007; 1–8.
Shinogle JA, Owings MF, Kozak LJ. Gastric bypass as treatment for obesity: trends, characteristics, and complications. Obesity Research. 2005;13:2202–9.
Sturm R. Increases in morbid obesity in the USA: 2000-2005. Public Health. 2007;121:492–6.
Buchwald H. Consensus conference statement bariatric surgery for morbid obesity: health implications for patients, health professionals, and third party payers. Surgery for Obesity and Related Diseases. 2005;1:371–81.
Dixon JB, O'Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–23.
Vetter ML, Cardillo S, Rickels MR, et al. Narrative review: effect of bariatric surgery on type 2 diabetes mellitus. Annals of Internal Medicine. 2009;150:94–103.
Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Obesity (Silver Spring). 2009;17 Suppl 1:S1-70, v.
Toussi R, Fujioka K, Coleman KJ. Pre- and Postsurgery behavioral compliance, patient health, and postbariatric surgical weight loss. Obesity. 2009;17:996–1002.
Patterson EJ, Urbach DR, Swanstrom LL. A comparison diet and exercise therapy versus laparascopic Roux-en-Y gastric bypass surgery for morbid obesity: a decision analysis model. Journal of the American College of Surgeons. 2003;196:379–84.
Christou NV, Look D, MacLean LD. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Annals of Surgery. 2006;244:734–40.
Campos GM, Rabl C, Mulligan K, et al. Factors associated with weight loss after gastric bypass. Archives of Surgery. 2008;143:877–84.
Melton GB, Steele KE, Schweitzer MA, et al. Suboptimal weight loss after gastric bypass surgery: correlation of demographics, comorbidities, and insurance status with outcomes. Journal of Gastrointestinal Surgery. 2008;12:250–5.
Chevallier JM, Paita M, Rodde-Dunet MH, et al. Predictive factors of outcome after gastric banding: a nationwide survey on the role of center activity and patients’ behavior. Annals of Surgery. 2007;246:1034–9.
Still CD, Benotti P, Wood C, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Archives of Surgery. 2007;142:994–8.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review of the literature. JAMA. 2004;292:1724–37.
Bray GA, Bouchard C, Church TS, et al. Is it time to change the way we report and discuss weight loss? Obesity. 2009;17:619–21.
Hollingshead AA. Four-factor index of social status, Unpublished manuscript. New Haven, CT: Yale University; 1975.
Saunders R, Johnson L, Teschner J. Prevalence of eating disorders among bariatric surgery patients. Eating Disorders. 1998;6:309–17.
Larsen JK, Geenen R. Childhood sexual abuse is not associated with a poor outcome after gastric banding for severe obesity. Obesity Surgery. 2005;15:534–7.
Glinski J, Wetzler S, Goodman E. The psychology of gastric bypass surgery. Obesity Surgery. 2001;11:581–8.
Kenchaiah S, Evans JC, Levy D, et al. Obesity and the risk of heart failure. The New England Journal of Medicine. 2002;347:305–13.
Fujioka K. Follow-up of nutritional and metabolic problems after bariatric surgery. Diabetes Care. 2005;28:481–4.
Fujioka K, Toussi RH, Brunson ME, et al. Health care utilization before and after bariatric surgery, the managed care experience. Obesity Research. 2001;9 Suppl 3:93S.
Lanyon RI, Maxwell BM. Predictors of outcome after gastric bypass surgery. Obesity Surgery. 2007;17:321–8.
Pontiroli AE, Fossati A, Vedani P, et al. Post-surgery adherence to scheduled visits and compliance, more than personality disorders, predict outcome of bariatric restrictive surgery in morbidly obese patients. Obesity Surgery. 2007;17:1492–7.
Colles SL, Dixon JB, O'Brien PE. Hunger control and regular physical activity facilitate weight loss after laparoscopic adjustable gastric banding. Obesity Surgery. 2008;18:833–40.
King WC, Belle SH, Eid GM, et al. Physical activity levels of patients undergoing bariatric surgery in the Longitudinal Assessment of Bariatric Surgery study. Surgery for Obesity and Related Diseases. 2008;4:721–8.
Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Annals of Internal Medicine. 2005;142:547–59.
Greenburg DL, Lettieri CJ, Eliasson AH. Effects of surgical weight loss on measures of obstructive sleep apnea: a meta-analysis. The American Journal of Medicine. 2009;122:535–42.
Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obesity Surgery. 2006;16:1609–14.
van Hout GC, Verschure SK, van Heck GL. Psychosocial predictors of success following bariatric surgery. Obesity Surgery. 2005;15:552–60.
Conflict of Interest
Dr. Coleman received a grant from Johnson and Johnson Pharmaceutical Research and Development in 2008 to study the impact of bariatric surgery on Kaiser Permanente patients’ diabetes. This funding was unrelated to the current project. Drs. Fujioka and Toussi have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Coleman, K.J., Toussi, R. & Fujioka, K. Do Gastric Bypass Patient Characteristics, Behavior, and Health Differ Depending upon how Successful Weight Loss is Defined?. OBES SURG 20, 1385–1392 (2010). https://doi.org/10.1007/s11695-010-0223-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-010-0223-y