
Abstract
Background
The role of Helicobacter pylori (HP) in patients scheduled and undergoing laparoscopic sleeve gastrectomy (LSG) has not been previously evaluated.
Methods
Included were obese patients presenting to our institution for LSG over 24 months. All patients had presurgical HP breath test, and the symptomatic ones received triple therapy with symptom follow-up. Post surgery, all excluded stomachs were evaluated for HP, and those that were positive performed a second 13C-urea breath test (UBT) 3 months later.
Results
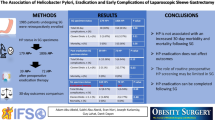
Forty patients underwent LSG. Male to female sex ratio was 1:3; mean age—42 years; mean weight—122 kg; and mean BMI of 43.4 kg/m2. Presurgical HP was positive in 15 (37.5%) patients (11 symptomatic and four asymptomatic). Only these 11 patients were given HP eradication therapy and all experienced complete subsequent symptom resolution. HP was detected in 17 out of the 40 (42.5%) cases of excluded stomachs. All performed a 13C-UBT 3 months post operation and only three (17.6%) tested positive.
Conclusions
HP infection is frequent in biopsies from patients with previous LSG and the majority of follow-up 13C-UBT were negative. In our small initial sample, we treated only symptomatic patients preoperatively. Routine screening for HP for all LSG patients and/or treatment for all positive ones would subject patients to expensive and unnecessary investigations. We propose that this stomach-reducing, pylorus-preserving surgery might even lead to HP eradication. The clinical implications of HP and this gastrectomy for a non-neoplastic, non-peptic indication deserve further study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Worldwide, the incidence of morbid obesity has increased dramatically. It has been estimated that 40% of the US population will be obese by the year 2025 if the current trend continues [1]. Surgery has been proven to be the most effective long-term treatment option for sustained weight loss and improvement in comorbidity in the morbidly obese [2]. There is a considerable increase in the number of surgeries: from 13,000 in 1998 to an overwhelming 177,600 people in 2006, reported by the American Society for Bariatric Surgery (ASMBS) [3].
Helicobacter pylori (HP) is a global pathogen that causes severe gastrointestinal diseases leading to a significant morbidity and mortality. The majority of individuals colonized by HP are asymptomatic although histologically they will have gastritis. A proportion of patients will develop peptic ulcers and a smaller proportion will develop gastric cancer [4]. Most peptic ulceration is due to chronic infection with H. pylori, and antibiotic treatments can generally cure both the infection and the ulceration [5].
The sleeve gastrectomy (SG), also called greater-curvature, vertical, or longitudinal gastrectomy, is a new tool in the surgical treatment of the morbidly obese. Gagner and coworkers introduced the concept of the staged approach to very obese patients with the LSG being the first step [6]. As laparoscopic sleeve gastrectomy (LSG) proved to be effective in the short term in achieving considerable weight loss, it has been proposed by some to be used solely as a bariatric procedure. LSG involves an 85% longitudinal resection of the stomach on the greater curvature from the antrum starting opposite of the nerve of Latarjet up to the angle of His.
The interaction between HP and patients scheduled and undergoing sleeve gastrectomy for morbid obesity is unknown. A search of the Medline database with the terms sleeve gastrectomy and Helicobacter led to nil results. This is the first paper addressing the topic HP infection in this relatively novel group of patients post non-neoplastic, non-peptic partial gastrectomy. Do patients scheduled for this operation require HP assessment? And does this extensive gastrectomy lead to HP eradication?
Materials and Methods
A retrospective review of a prospectively maintained database and patient medical record review of all morbidly obese patients presenting to our institution for LSG as a primary restrictive one-stage procedure over a 24-month period from January 2006 to December 2007 was performed. This study was approved by the local ethical committees.
LSG was offered in the presence of the following criteria: patient preference. Contraindications for the procedure included extensive previous surgery and Crohn’s disease, elderly patients with significant comorbidity, adolescents, patients on anticoagulant medications, recalcitrant smokers, and patients with low body mass index (BMI) of 35–40 kg/m2 with comorbidity. All patients had routine laboratory investigations including nutritional parameters, HP breath test, chest X-ray, electrocardiogram, abdominal ultrasound, psychiatric evaluation, and additional investigations as deemed necessary determined by their comorbid conditions.
The patients are evaluated and are followed up in the Health and Nutrition clinic at the Bnai Zion Medical Center, Haifa, Israel. This clinic is under the unique auspices of a physician specializing in gastroenterology and nutrition. The clinic visits included a routine history and physical exam with specific questions aimed at evaluating gastrointestinal symptoms, a nutritional consultation (including a 3-day dietary recall), anthropometric measurement, and periodic laboratory exams.
At each clinic, including presurgical evaluation, they were asked to report if they had any of the following symptoms: abdominal pain, dyspepsia or indigestion, bloating and fullness, nausea or vomiting, belching and regurgitation, heartburn, feeling very hungry 1 to 3 h after eating, and constipation or diarrhea.
If anyone of the patients reported one of the mentioned symptoms (except for constipation and diarrhea) for longer than a month prior to surgery patients and had a positive HP test, they were treated with a 2-week course of triple therapy (clarithromycin, amoxycillin, and omeprazole). And symptoms were followed in clinic visits before surgery.
Post surgery patients were followed up beginning on a weekly basis for a month and then every month for another 3 months and then every other month for the year.
The biopsy specimens for histology were fixed in 10% buffered formalin, embedded in paraffin, sectioned and stained with hematoxylin eosin and stained with Wright–Giemsa, and also processed for immunohistochemistry as reference [7, 8]. Each biopsy specimen was examined for the presence of H. pylori by a single experienced pathologist. The extent of inflammation (mononuclear cell infiltration) and cellular activity (neutrophil infiltration) were also categorized and scored according to the updated Sydney system (0 = none, 1 = mild, 2 = moderate, and 3 = marked) [9].
All patients with pathologies that were positive for HP infection performed a C-13 urea breath test 3 months after the surgery after a 7-day wash out period from the proton pump inhibitors they were taking routinely, to help treat and prevent expected reflux symptoms after surgery.
Statistical Analysis
Data analysis was performed using the statistical software package SPSS 10.0 for Windows. The chi-square test was used when appropriate. P < 0.05 was considered statistically significant.
Results
Over the 2-year period, 40 patients underwent LSG as a single-stage restrictive procedure for morbid obesity (Fig. 1).

This flow diagram shows the number of patients and their progress from presurgical evaluation to post operative breath test. LSG Laparoscopic sleeve gastrectomy, Neg negative, Pos positive, HP Helicobacter pylori
Of the patients who had LSG as a primary restrictive procedure, the majority were female with a male-to-female sex ratio of 1:3. The mean age was 42 years (range 13–79) and mean weight was 122 kg, with a mean BMI of 43.4 kg/m2 (range 35–75). The procedure was completed laparoscopically in all cases (100%). The baseline demographic characteristics were similar in both groups (the symptomatic and asymptomatic).
Presurgical Helicobacter assessment was positive in 15 (37.5%) patients; from them, 11 were symptomatic and four were asymptomatic (Table 1). These results were statistically significant (P < 0.05). These 11 patients were given H. pylori eradication therapy and all experienced subsequent resolution of their symptoms. The remaining four asymptomatic patients did not receive triple therapy prior to surgery.
Helicobacter pylori in Excluded Stomach
H. pylori was detected in 17 out of the 40 (42.5%) cases of the excluded stomach, as seen by positive Giemsa staining. Staining was positive in the antrum in all of them and in the body in four patients. Gastritis of the excluded stomach was associated to the presence of H. pylori. The pattern of inflammation was usually in the form of active chronic gastritis characterized by the presence of acute and chronic inflammatory cells in the lamina propria.
The symptomatic group had ten positive biopsies (four of them post triple therapy treatment). The asymptomatic (all untreated group) had seven positive biopsies (Table 2) and the results comparing the presurgical breath test to the biopsies in this group were statistically significant (P < 0.01).
These 17 biopsy positive patients performed a HP breath test 3 months post operation and only three (17.6%) tested positive (Table 3). A decision concerning treatment for HP in these three patients was postponed due to low stomach volume and probable low patient compliance with the antibiotic treatment. The other 14 patients had negative breath tests (82.4%).
In the first 3 months after LSG, 38 patients recovered completely from the operation with no minor or major complications. Only two patients required readmission (5%). The two patients had a history of previous gastric banding surgery. These two patients did not have HP in their pathology specimens. The admissions were related to dehydration from inadequate oral intake or vomiting, related to transient gastric dysmotility. Both these patients’ symptoms were transient after proper in- and out-hospital care. There were no cases of leaks or hemorrhages.
Discussion
This paper brings to discussion some interesting questions concerning the issue of HP in patients undergoing LSG for morbid obesity. What should be the approach regarding presurgical HP breath test for sleeve gastrectomy patients? Should all patients be tested or only the symptomatic? Must all positive HP breath test patients be treated prior to surgery? Is the urea breath test an applicable tool for sleeve gastrectomy patients? And can this type of gastrectomy lead to Helicobacter eradication and therefore possibly leading to a situation whereupon not all patients will require preoperative triple therapy treatment.
In this retrospective review of patients undergoing LSG, we found that the HP infection rate was 37.5% in the presurgical breath test and 42.5% in the gastric specimen, falling within the estimates of 20% to 50% prevalence in developed countries [4]. The prevalence in our series is as published results in patients undergoing weight loss surgery, which identified rates of 30% to 67% [10–12].
In recent years, there has been renewed interest in the surgical treatment of morbid obesity in concomitance with the epidemic of obesity and application of the laparoscopic techniques to the field of bariatric surgery as well. Bariatric surgery proved effective in providing weight loss of large magnitude, correction of comorbidities, and excellent short-term and long-term outcomes [13, 14], decreasing overall mortality and providing a marked survival advantage [15, 16]. The popularity of bariatric surgery has increased in recent years. There were 71,733 bariatric surgeries performed in the US in 2002, a significant increase from the 13,386 surgeries performed in 1998 [17]. In 2006, the ASMBS reported an estimated 177,600 people in the US had bariatric surgery [18].
LSG is the restrictive part of the more extensive mixed restrictive and malabsorptive operation, gastric bypass and duodenal switch (GB/DS). It generates weight loss solely by stomach reduction and thereby restricting the amount of food that can be eaten without any bypass of the intestines or malabsorption. With this procedure, the surgeon removes approximately 85% of the stomach laparoscopically so that the stomach takes the shape of a tube or “sleeve”. This part of the procedure is not reversible. Unlike many other forms of bariatric surgery, the outlet valve and the nerves to the stomach remain intact. The nerves to the stomach and the outlet valve (pylorus) remain intact with the idea of preserving the functions of the stomach while reducing the volume.
Should HP be Tested and Eradicated Before Surgery in all Patients?
In our study, we tested everyone and treated only the symptomatic ones. The results were statistically significant that the breath test is more positive in the symptomatic group. In prior studies of bariatric surgery, HP status is not always taken into consideration when planning the operation for morbid obesity. The prevalence of HP is not uncommon in this special subset of patients and ranges from 24% to 43.7% [19]. Many have suggested that it should be eradicated in morbidly obese patients before bariatric surgery [20, 21]. This concept is based on the assumption that HP infection may lead to chronic gastritis, peptic ulcer, and even gastric malignancies, whereas the examination of the stomach after bariatric surgery is a difficult task [22].
H. pylori infection is frequently seen in the gastric remnant after operations for peptic ulcer disease, but the infection does not seem to cause ulcer relapses in the gastric stump or in the anastamosis [23]. In our study, there were nine HP-positive patients (six from the symptomatic group and only three from the asymptomatic group) in the biopsy specimens from the 25 negative presurgical breath tests. This exhibits a higher false negative urea breath test results in the intact stomach in the symptomatic group (60%) compared with the asymptomatic group (20%).
The Urea Breath Test in Post LSG Patients
The diagnosis of HP infection is currently established by histological, rapid urease, and culture tests using endoscopic biopsy specimens or by a 13C-urea breath test (13C-UBT). The latter is a non-invasive approach based on the potent urease activity of HP and many reports evaluating its clinical utility have been published [24].
The 13C-UBT is an excellent and non-invasive method for diagnosis of HP infection in the intact stomach and it is especially useful for judging the results of eradication therapy [25, 26]. Its efficacy in the diagnosis of HP infection in the remnant stomach after surgery is controversial. With a residual stomach after partial gastrectomy, the gastric anatomy is considerably altered and the test urea might be expected to pass through the stomach faster, giving different reactant percentages in reaction time. Studies concerning the gastric emptying post pylorus-preserving procedures such as the sleeve gastrectomy are not conclusive. Some state that the emptying is preserved [27] and others state that it is accelerated [28]. Therefore the validity of this breath test under this type of surgery must be further studied.
Several reports have shown that the 13C-UBT is not as accurate as histological examination and culture in detecting HP after gastrectomy [29, 30], but others concluded that 13C-UBT is a sufficient, non-invasive diagnostic tool with nearly the same accuracy rate as routine tests with the present protocol, even in patients with only a remnant stomach after partial gastrectomy [31–34].
Another study proved that the 13C-UBT can be positive without HP in post gastrectomy patients. Having in mind that the basis for the urea breath test is the ability of HP in the stomach to break down urea, a chemical made up of nitrogen and carbon. They investigated the content of (13)CO2 in the CO2 gas expired after direct influx of 13C-urea into the small intestine. It suggested the possibility that 13C-urea is decomposed even in the jejunum or the lower part of the intestine resulting in absorption of H(13)CO3 and another possibility that 13C-urea is directly absorbed from the intestine and decomposed in the blood [35].
Does LSG Lead to HP “Eradication”?
Our study showed that, from 17 HP-positive biopsies, 14 patients (82.4%) had negative urea breath test after 3 months. It is interesting to note that, from the seven positive biopsies in the asymptomatic group whom did not receive any presurgical therapy, only one (14.28%) breath test remained positive after 3 months. This fact that 85.7% of the patients might have been eradicated just from the surgery may indicate a possibility that this extensive gastrectomy has an effect upon HP eradication.
Studies concerning the remission of HP infection after partial gastrectomy showed that the prevalence of HP within 3 years of gastrectomy was 59.5% and it decreased to 28.6% after 3 years of gastrectomy [36]. It may be due partly to the resection of distal gastric tissue, a usual site of infection, and only partly to the bactericidal effects of prolonged bile acid reflux in surgical patients [37]. Whatever the reason, this decrease represents one way surgery could contribute to the cure of peptic ulcer disease [38]. The severity of gastritis and prevalence of HP infection decreased gradually after vertical banding gastroplasty. The reduced food intake and uses of perioperative antibiotics were possible explanations for this phenomenon [39].
Bile reflux interferes with colonization by HP [40]. This is accentuated when comparing patients with Bilroth II (BII) to Bilroth I anastomosis, the BII exhibit positive to negative seroconversion for HP infection after the operation (mean 2.47 years), a phenomenon that was not observed in patients with Bilroth I anastomosis. But there is no reason for bile reflux after this pylorus-preserving procedure and therefore this explanation is not applicable.
Patients with major gastric resections, having a small residual stomach, had a lower HP persistence rate than patients with a large residual stomach for all three postoperative time periods, the difference being significant in the subgroup with the longest elapsed time since surgery. Taken together, persistence of HP colonization in the residual stomach is clearly related to both the degree of surgical resection and the time elapsed after surgery [41].
In summary we have shown that H. pylori infection is frequent in biopsy specimens from patients with previous sleeve gastrectomy for non-neoplastic, non-peptic disease and the majority of follow-up 13C-UBT were negative. In our small initial sample, we treated only symptomatic patients preoperatively. Routine screening for HP for all sleeve gastrectomy patients and/or treatment for all the positive ones would subject patients to expensive and unnecessary investigations. Furthermore, indiscriminate use of antibiotics not only wastes resources but also increases the risk of adverse drug reactions and resistance to antibiotic. We propose that this stomach-reducing, pylorus-preserving surgery might even lead to HP eradication. Further clinical studies on larger populations should be performed in order to address this issue and compose appropriate guidelines for this relative new procedure.
References
Kopelman PG. Obesity as a medical problem. Nature 2000;404:635–43.
Maggard MA, Shugarman LR, Suttorp M. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142(7):547–59.
Bariatric Surgical Society Takes On New Name, New Mission and New Surgery at http://www.asbs.org/Newsite07/resources/press_release_8202007.pdf published by the American Society for Bariatric Surgery 2007.
Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med. 2002;347:1175–86.
Goodwin CS, Mendall M, Northfield TC. Helicobacter pylori infection. Lancet 1997;349:265–9.
Regan JP, Inabnet WB, Gagner M. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg. 2003;13:861–4.
Eshun JK, Black DD, Casteel HB. Comparison of immunohistochemistry and silver stain for the diagnosis of pediatric Helicobacter pylori infection in urease-negative gastric biopsies. Pediatr Dev Pathol. 2001;4:82–8.
Toulaymat M, Marconi S, Garb J, et al. Endoscopic biopsy pathology of Helicobacter pylori gastritis. Comparison of bacterial detection by immunohistochemistry and Genta stain. Arch Pathol Lab Med. 1999;123:778–81.
Dixson MF, Genta RM, Yardley JH. Classification and grading of gastritis. The update Sydney system. Am J Surg Pathol. 1996;20:1161–81.
Renshaw AA, Rabaza JR, Gonzalez AM. Helicobacter pylori infection in patients undergoing gastric bypass surgery for morbid obesity. Obes Surg. 2001;11:281–3.
Papavramidis ST, Theocharidis AJ, Zaraboukas TG, et al. Upper gastrointestinal endoscopic and histologic findings before and after vertical banded gastroplasty. Surg Endosc. 1996;10:825–30.
Schirmer B, Erenoglu C, Miller A. Flexible endoscopy in the management of patients undergoing Roux-en-Y gastric bypass. Obes Surg. 2002;12:634–8.
Buchwald H, Avidor Y, Braunwald E. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37.
Sugerman HJ, Kral JG. Evidence-based medicine reports on obesity surgery: a critique. Int J Obes (Lond). 2005;29:735–45a.
Christou NV, Sampalis JS, Liberman M. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240:416–23, discussion 423–424.
Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199:543–51.
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Working Group on Bariatric Surgery, Executive Summary. May 2002.
Bariatric Surgical Society Takes On New Name, New Mission and New Surgery at http://www.asbs.org/Newsite07/resources/press_release_8202007.pdf published by the American Society for Bariatric Surgery 2007.
Wu MS, Lee WJ, Wang HH, et al. A case–control study of association of Helicobacter pylori infection with morbid obesity in Taiwan. Arch Intern Med. 2005;165:1552–4.
Ramaswamy A, Lin E, Ramshaw BJ, et al. Early effects of Helicobacter pylori infection in patients undergoing bariatric surgery for morbid obesity. Arch Surg. 2004;139:1094–6.
Cordeiro F, Ferraz E. H. pylori and gastroplasty in the treatment of morbid obesity. Am J Gastroenterol. 2001;96:605–6.
Stellato TA, Crouse C, Hallowell PT. Bariatric surgery creating new challenges for the endoscopist. Gastrointest Endosc. 2003;57:86–94.
Leivonen M, Nordling S, Haglund C. The course of Helicobacter pylori infection after partial gastrectomy for peptic ulcer disease. Hepatogastroenterology 1998;45(20):587–91, Mar–Apr.
Koletzko S, Haisch M, Seeboth I. Isotopeselective non-dispersive infrared spectrometer for detection of Helicobacter pylori infection with 13C-urea breath test. Lancet 1995;345:961–2.
Graham DY, Klein PD, Evans DJ Jr. Campylobacter pylori detected noninvasively by the 13C-urea breath test. Lancet 1987;1:1174–7.
Cutler AF, Havstad S, Ma CK. Accuracy of invasive and non-invasive tests to diagnose Helicobacter pylori infection. Gastroenterology 1995;109:136–41.
Nishikawa K, Kawahara H, Yumiba T, et al. Functional characteristics of the pylorus in patients undergoing pylorus-preserving gastrectomy for early gastric cancer. Surgery 2002;131(6):613–24, Jun.
Melissas J, Koukouraki S, Askoxylakis J, et al. Sleeve gastrectomy: a restrictive procedure. Obes Surg. 2007;17(1):57–62, Jan.
Sheu B-S, Lee S-C, Lin P-W, et al. 13Carbon urea breath test is not as accurate as endoscopy to detect Helicobacter pylori after gastrectomy. Gastrointest Endosc. 2000;51:670–5.
Schilling D, Jakobs R, Peitz U. Diagnostic accuracy of 13C-urea breath test in the diagnosis of Helicobacter pylori infection in patients with partial gastric resection due to peptic ulcer diseases: a prospective multicenter study. Digestion 2001;63:8–13.
Kubota K, Shimoyama S, Shimizu N, et al. Studies of 13C-urea breath test for diagnosis of Helicobacter pylori infection in patients after partial gastrectomy. Digestion 2002;65(2):82–6.
Kubota K, Hiki N, Shimizu N, et al. Utility of [13C] urea breath test for Helicobacter pylori detection in partial gastrectomy patients. Dig Dis Sci. 2003;48(11):2135–8, Nov.
Togashi A, Matsukura N, Kato S, et al. Simple and accurate (13)C-urea breath test for detection of Helicobacter pylori in the remnant stomach after surgery. J Gastroenterol. 2006;41(2):127–32, Feb.
Lotterer E, Ludtke FE, Tegeler R, et al. The 13Curea breath test-detection of Helicobacter pylori infection in patients with partial gastrectomy. Z Gastroenterol. 1993;31:115–9.
Rino Y, Takanashi Y, Hasuo K, et al. 13C-urea breath test in patients having undergone total gastrectomy. Hepatogastroenterology 2007;54(77):1601–3, Jul–Aug.
Kim ES, Park DK, Hong SH. Helicobacter pylori infection in the remnant stomach after radical subtotal gastrectomy. Korean J Gastroenterol. 2003;42(2):108–14, Aug; Korean.
O’Connor HJ, Wyatt JI, Ward DC, et al. Effect of duodenal ulcer surgery and enterogastric reflux on Campylobacter pyloridis. Lancet 1986;(i):1178–81.
Danesh J, Appleby P, Peto R. How often does surgery for peptic ulceration eradicate Helicobacter pylori? Systematic review of 36 studies. BMJ 1998;316(7133):746–7, Mar 7.
Papavramidis ST, Theocharidis AJ, Zaraboukas TG. Upper gastrointestinal endoscopic and histologic findings before and after vertical banded gastroplasty. Surg Endosc. 1996;10:825–30.
Lee YT, Sung JJ, Choi CL, et al. Ulcer recurrence after gastric surgery: is Helicobacter pylori the culprit. Am J Gastroenterol. 1998;93(6):928–31, Jun.
Sheu BS, Lee SC, Lin PW, et al. Carbon urea breath test is not as accurate as endoscopy to detect Helicobacter pylori after gastrectomy. Gastrointest Endosc. 2000;51:670–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Keren, D., Matter, I., Rainis, T. et al. Sleeve Gastrectomy Leads to Helicobacter pylori Eradication. OBES SURG 19, 751–756 (2009). https://doi.org/10.1007/s11695-008-9694-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9694-5