
Abstract
Background
Obesity is not only associated with nonalcoholic fatty liver disease (NAFLD) but it also adversely affects the progression of other liver diseases. There are limited data regarding the dietary habits of patients with chronic liver disease.
Methods
Nutrition surveys containing 13 different food groups were mailed. Nutrition scores were calculated based on weekly servings. Foods were also divided into USDA food pyramid categories with conversion of each group into calories expended. Clinico-demographic data were available. NAFLD patients were compared to patients with chronic viral hepatitis.
Results
A total of 233 subjects were included: age 52.5 ± 10.0 years, Body mass index (BMI) 28.1 ± 6.5, MS 24.2%, 31.8% NAFLD, 48.1% hepatitis C virus (HCV), and 20.2% hepatitis B virus (HBV). Six nutrition indices were different among the groups. NAFLD and HCV consumed more low-nutrient food (p = 0.0037 and 0.0011) and more high-sodium food than HBV (p = 0.0052 and 0.0161). Multivariate analysis showed that NAFLD and HCV consumed more high-fat sources of meat/protein than HBV (p = 0.0887 and 0.0626). NAFLD patients consumed less calories from fruits compared to HCV and HBV patients (p = 0.0273 and 0.0023). Nine nutrition indices differed according to BMI. Univariate analysis showed that obese/overweight patients consumed more high-fat sources of meat/protein (p = 0.0078 and 0.0149) and more high-sodium foods (p = 0.0089 and 0.0062) compared to the normal-weight patients. In multivariate analysis, normal-weight patients consumed more fruits than obese (p = 0.0307). Overweight patients also consumed more calories of meat and oil than normal-weight patients (p = 0.0185 and 0.0287).
Conclusion
NAFLD and HCV patients have similar dietary habits. Patients with HBV have the healthiest dietary habits. Specific dietary interventions should focus on decreasing intake of low-nutrient and high-sodium food, as well as high-fat sources of meat/protein.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity increases the risk of developing a number of serious systemic disorders, such as cardiovascular disease, diabetes, cancer and nonalcoholic fatty liver disease (NAFLD). Obesity is a complex disease that has both genetic as well as dietary intake and activity components. The latter two make up important environmental factors contributing to obesity. Among chronic liver diseases, NAFLD is increasingly recognized as one of the most common, affecting 20–30% of the US population [1]. It has also been well established that obesity, metabolic syndrome (MS), and insulin resistance are all strongly associated with NAFLD. In fact, NAFLD is now recognized as the hepatic manifestation of MS [2]. In addition to its primary form of liver disease (NAFLD), obesity can exacerbate progression of other liver diseases such as chronic hepatitis C and to a lesser extent alcohol-related liver disease, iron overload and chronic hepatitis B. Furthermore, in patients with chronic hepatitis C, obesity has been associated with impaired treatment response to antiviral therapy [3–5].
Despite the important contribution of obesity to a number of liver diseases, dietary habits of patients with NAFLD and chronic viral hepatitis have not been fully studied. A few studies have suggested that NAFLD patients may consume more carbohydrates, saturated fat, and protein from meat [6–8]. Although weight loss through dietary changes is recommended for patients with NAFLD, only weight loss with bariatric surgery has consistently been shown to improve all important outcomes of patients with NAFLD. Furthermore, it is unknown whether dietary intake of patients with different types of liver disease differs from each other and whether these differences can be used as potential targets for future therapeutic interventions. In this study, our aim was to compare the nutritional status of patients with three common causes of chronic liver diseases—NAFLD, HCV, and HBV. This information may be important for dietary intervention through weight loss programs or postbariatric surgery.
Methods
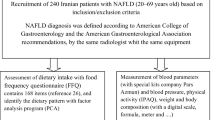
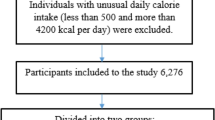
This study included patients with established diagnoses of NAFLD, chronic hepatitis B and C. The patients with liver mass (without chronic liver disease), acute hepatitis and post-liver transplant were excluded. All the patients received a nutrition survey which contained 7 items in 13 categories measuring dietary choices and frequencies of consumption for a wide variety of foods. The Nutrition Survey included the following categories: (1) vegetable sources of protein; (2) lean sources of protein; (3) high-fat sources of meat/protein; (4) total vegetable consumption; (5) low-fat milk products; (6) high-fat milk products; (7) low-nutrient dense foods, baking products, fats, oils, and sweets; (8) high caffeine; (9) alcohol; (10) high-sodium foods; (11) fruits; (12) bread and starchy foods; (13) cereals and grains.
All the patients enrolled lived in the USA (Mid-Atlantic States). Demographic and clinical data such as weight, height, and past medical history were available. Scores from nutrition questionnaire were calculated based on weekly servings and entered into a database. Specific foods were also divided into USDA food pyramid categories including (1) fats and oils; (2) milk, yogurt, cheese; (3) meat, poultry, fish, dry beans, eggs, and nuts; (4) fruits; (5) vegetables; (6) bread, cereal, rice, and pasta; and (7) other. Once the food was divided into the specific category, serving sizes were converted to calories based on the USDA file data. The protocol was fully approved by our institutional review board.
Statistical Analysis
Continuous variables and categorical variables are summarized as mean ± SD and percent (%), respectively. Chi-square or Fisher exact test was used to investigate the association between categorical variables. Comparisons between various groups were done using Student’s t test or analysis of variance for normal distributed data, and for nonnormal data using Wilcoxon–Mann–Whitney test or Kruskal–Wallis test. Additional analysis was performed using Pearson or Spearman correlation to investigate the association between normal or nonnormal data, respectively. Bonferroni method was used to adjust the p values for comparisons on more than two groups.
Multivariate analyses were conducted using general linear model with 13 different nutrition domains as outcome variables to investigate the nutrition patterns in concerned groups while controlling for confounders. Those covariates significant at 0.10 levels on univariate analysis were included in the multivariate model. The same type of multivariate analysis was used with the seven food pyramid groups.
For all our analyses, two failed p values were used, and a p value of < 0.05 was considered significant. All analyses were performed using SAS software (SAS, Cary, NC, USA).
Results
Demographics
A total of 233 patients with NAFLD, HCV, or HBV were included. Clinical and demographic data are provided in Table 1. The entire cohort’s mean age was 52.5 ± 10.0 years with 47.1% being male. Various ethnic groups were represented with 60.8% Caucasians, 23.1% Asians, 11.6% African-Americans, and 4.5% others.
A breakdown of patients with NAFLD, HCV, and HBV who had MS versus obesity is provided in Table 2. Metabolic syndrome was defined according to the adult treatment panel (ATP) III criteria [1, 2]. Of the entire cohort, 24.2% met the diagnosis of metabolic syndrome, while 50% of NAFLD patients had MS. In comparison, MS occurred in 12.7% in HCV and 10.6% in the HBV group [NAFLD vs. HCV (p < 0.001) and NAFLD vs. HBV (p < 0.001)]. Obesity defined as body mass index (BMI) ≥ 30 occurred in 46.5% of NAFLD patients as compared to 28.3% in HCV (p = 0.0492) and 13.0% in HBV (p = 0.0007).
Comparison of Nutritional Scores and Calories for USDA Food Pyramid Nutrition Categories Between NAFLD, HCV, and HBV
Six of 13 nutrition categories differed significantly between NAFLD, HCV, and HBV in the univariate analysis (Table 3). NAFLD group consumed more vegetable sources of protein than HCV (p = 0.0398). Both NAFLD and HCV consumed more low-nutrient food (p = 0.0037 and 0.0011, respectively) and more high-sodium food than HBV (p = 0.0052 and 0.0161, respectively). HBV patients had a more healthy diet with consuming more total vegetable consumption than NAFLD (p = 0.0434) and more cereal and grains than NAFLD and HCV (p = 0.0006 and 0.0001, respectively). Moreover, HCV and HBV patients consumed more fruits than NAFLD patients (p = 0.0066 and 0.0192, respectively).
Calories for three food pyramid nutrition categories differed between NAFLD, HCV, and HBV in the univariate analysis (Table 4). Consistent with the nutrition score analysis, NAFLD patients consumed less calories of fruits than HCV and HBV (p = 0.0112 and 0.0319, respectively). NAFLD and HCV patients also consumed more calories of milk products than HBV (p = 0.0356 and 0.0137, respectively). Lastly, NAFLD patients consumed more calories of meat and bean than HCV (p = 0.0316).
The multivariate analysis showed that NAFLD and HCV patients tended to consume more high-fat sources of meat/protein than HBV patients (p = 0.0887 and 0.0626, respectively). The multivariate analysis also showed that NAFLD patients consumed less calories of fruits than HCV and HBV (p = 0.0273 and 0.0023, respectively).
Comparison of Nutritional Scores and Calories for USDA Food Pyramid Nutrition Categories Between Patients with and without Cirrhosis
A total of 25.3% of the cohort had either a clinical or histological diagnosis of cirrhosis. Only two nutrition indices were different between those with cirrhosis and those without cirrhosis (Table 5). Although univariate analysis showed a difference in the consumption of bread and starchy foods (p = 0.0039) and alcohol (p = 0.0019), the multivariate analysis revealed that cirrhotic patients tended to consume more low-fat milk products (p = 0.0561). On the other hand, the multivariate analysis conducted with calories for the USDA food pyramid nutrition categories (Table 6) showed that cirrhotic patients consumed more calories of grains than noncirrhotic patients (p = 0.0153).
Comparison of Nutritional Scores and Calories for USDA Food Pyramid Nutrition Categories According to the Body Mass Index
This cohort of patients with chronic liver disease was categorized as underweight (BMI < 18.5), normal weight (18.5 ≤ BMI < 25.0), overweight (25.0 ≤ BMI < 30), and obese (BMI ≥ 30.0). The underweight category was 1.8%, the normal-weight category was 31.4%, the overweight category was 35.9%, and the obese category was 30.9% of the entire cohort. After excluding underweight patients and those with incomplete data, 219 patients were used for this analysis (Tables 7, 8). Nine nutrition categories differed significantly between these BMI groups in the univariate analysis (Table 7). Univariate analysis showed that obese and overweight patients consumed more high-fat sources of meat/protein (p = 0.0078 and 0.0149, respectively) and more high-sodium foods (p = 0.0089 and 0.0062, respectively) as compared to the normal-weight patients. Overweight group also consumed more high-fat milk products (p = 0.0064) and more low-nutrient foods (p = 0.0101) as compared to the normal-weight group. Normal-weight and overweight groups consumed more fruit than the obese group (p = 0.0484 and 0.0392, respectively). Overweight patients consumed more cereals and grains than obese patients (p = 0.0281). Total calories differed only between normal and overweight patients with less calories consumed by the normal-weight group (p = 0.0090).
Calories for four food pyramid nutrition categories differed between the BMI groups in the univariate analysis (Table 8). Overweight patients consumed more calories of grains and calories of fat than normal-weight patients (p = 0.0489 and 0.0118, respectively). Obese and over-weight patients consumed more calories of meat and bean than normal-weight patients (p = 0.0367 and 0.0490, respectively). Over-weight patients also consumed more calories of fruits than obese patients (p = 0.0237).
In the multivariate analysis, normal-weight patients with chronic liver disease consumed more fruits than obese patients (p = 0.0307). Overweight patients consumed more cereals and grains than normal-weight patients (p = 0.0288). Obese patients with chronic liver disease tended to consume more total vegetable consumption (p = 0.0512) and high-fat milk products (p = 0.0587) compared to the normal-weight patients. Overweight patients consumed more calories of meat and oils than normal-weight patients (p = 0.0185 and 0.0287, respectively).
Discussion
This is the first in-depth nutritional assessment of patients with NAFLD and two other common types of chronic liver disease. Our study shows that dietary habits of NAFLD and HCV patients were similar to each other and different from patients with chronic hepatitis B. NAFLD and HCV patients tended to have higher consumption of low nutrient, high-fat sources of meat/protein, and high sodium foods. Although dietary habits of NAFLD and HCV were similar in the three indices of low nutrient, high-fat sources of meat/protein, and high-sodium foods, these specific measures may not necessarily translate into the development of obesity or MS in a different cohort of patients. Additional factors such as physical activity and basal metabolic rate may also play an important role in the development of conditions associated with metabolic syndrome.
Furthermore, current medical practice dictates lifestyle modification including dietary changes as the primary intervention for NAFLD. However, there are little data on the long-term efficacy of this approach for patients with NAFLD. Additionally, there seems to be a discrepancy between the current patient practice and general recommended provider guidelines. This may be due to either patient non-adherence or lack of emphasis or appropriate education from the healthcare providers.
The fact that NAFLD, HCV, and those who are overweight had high consumption of low-nutrient foods is clinically significant. Low-nutrient foods such as sweets that contain high fructose contents have been found to increase de novo lipogenesis, especially in the insulin resistant overweight subjects [9]. Solga also showed that high-carbohydrate intake (60% of calories) was associated with a higher degree of hepatic inflammation [10]. Thus, it is reasonable to deduce that low nutrient foods should be restricted or at least limited in patients with chronic liver diseases, especially if there is a concomitant insulin resistance or diabetes mellitus.
In our study, there was a tendency for NAFLD, HCV, and obese patients with chronic liver disease to consume more high-fat sources of meat/protein. This trend is corroborated by previous studies of Cortez-Pinto and Musso [7, 8]. Literature suggests that saturated fatty acids promote endoplasmic reticulum stress and hepatocyte injury which have been implicated in the pathogenesis of obesity related liver disease (NAFLD) [11]. It seems reasonable to suggest that high-fat sources of meat/protein, which contribute to obesity, should be limited in patients with chronic liver disease. However, study by Solga showed that hepatic inflammation was less prominent in those with higher fat intake (48% of the total calories) which is in direct contradiction to the current dietary recommendations for NAFLD patients [10].
Our study also showed that hepatitis B patients had the healthiest diet. They consumed the greatest amount of fruits and vegetables and tended to consume more lean sources of protein and overall fewer calories. This may explain the lower incidence of MS and obesity and in patients with HBV. It is important to note that the majority of HBV patients were of Asian descent which may explain some of these differences. However, our multivariate analysis did control for race as a potential confounder. Nevertheless, future studies must further address this important issue.
In this study, we also assessed the dietary habit of patients with or without cirrhosis. Our results showed a similar prevalence of MS and obesity in patients with or without cirrhosis. Cirrhotic patients also consumed less alcohol, thereby being in compliance with clinical instructions to avoid alcohol. In addition, cirrhotic patients consumed more calories of grain than noncirrhotic patients. Otherwise, nutrient intakes between cirrhotic and noncirrhotic patients were similar. Although malnutrition can be seen in 27–87% of patients with chronic liver disease, our study did not specifically investigate malnutrition in these patients [12]. Nevertheless, if there were significant differences between cirrhotics and noncirrhotics, we would have expected different dietary intakes between these two groups.
Analysis based on BMI groups also provided us with insight into the possible dietary contributors to obesity in patients with chronic liver disease. Overweight patients with chronic liver disease consumed more cereal along with more calories from meat and oils as compared to normal-weight patients. Although we cannot conclude a causal relationship, it is reasonable to deduce that reducing intakes in the meat and oil may be targeted for weight loss plan of these overweight/obese patients with chronic liver disease. With accomplishing sustained weight loss, one can expect some reduction of the negative influence of obesity on chronic liver diseases.
This study does have some limitations. With any questionnaire study, there is the possibility of recall bias or reporting bias. Future investigation should ideally be done prospectively looking to see if education specific to the three nutritional categories of low nutrient, high-fat sources of meat/protein, and high-sodium foods that differed between the three major liver disease groups affects the overall prevalence of metabolic syndrome, obesity, or progression of liver disease. Our findings suggest, however, that additional nutrition education and counseling are needed regarding increasing nutrient dense foods, fruit, and vegetable consumption.
Nevertheless, this study provides important data regarding the nutritional status of patients with NAFLD and other important causes of chronic liver disease. Our study provides data on the relatively poor dietary habits of NAFLD and HCV patients in comparison to patients with HBV. Food categories that need to be targeted for potential intervention include the low-nutrient diets, high-fat sources of meat/protein, and high-sodium foods. Referral to a nutritionist to further educate these patients about the important role of nutrition in liver disease should also be integrated into the plan of care. In addition to the generic recommendation for “low fat, low calorie” diet, we may be able to specifically focus on these three nutritional categories in hopes of reducing the impact of obesity and MS on chronic liver disease.
References
Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steatohepatitis: summary of an AASLD single topic conference. Hepatology. 2003;37:1202–9.
Marchesini G, Brizi M, Morselli-Labate AM, Bianchi G, Bugianesi E, McCullough AJ, et al. Association of nonalcoholic fatty liver disease with insulin resistance. Am J Med. 1999;107:450–5.
Poustchi H, Negro F, Hui J, Cua IHY, Brandt LR, Kench JG, et al. Insulin resistance and response to therapy in patients infected with chronic hepatitis C virus genotypes 2 and 3. J Hepatology. 2008;48:28–34.
Bondini S, Kallman J, Wheeler A, Prakash S, Gramlich T, Jondle DM, Younossi ZM. Impact of non-alcoholic fatty liver disease on chronic hepatitis B. Liver International. 2007;27:607–11.
Bondini S, Younossi ZM. Non-alcoholic fatty liver disease and hepatitis C infection. Minerva Gastroenterol Dietol. 2006;52:135–43.
Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, Webb M, Blendis L, Halpern Z, et al. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): a population based study. J Hepatol. 2007;47(5):711–7.
Cortez-Pinto H, Jesus L, Barros H, Lopes C, Moura MC, Camilo ME. How different is dietary pattern in non-alcoholic steatohepatitis patients? Clin Nutr. 2006;25:816–23.
Musso G, Gambino R, De Michieli F, Cassader M, Rizzetto M, Durazzo M, et al. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology. 2003;37:909–16.
McDevitt RM, Scott SJ, Harding M, Coward WA, Bluck LJ, Prentice AM. De novo lipogenesis during controlled overfeeding with sucrose or glucose in lean and obese women. Am J Clin Nutr. 2001;74:737–46.
Solga S, Alkhuraishe AR, Clark JM, Torbenson M, Greenwald A, Diehl AM, et al. Dietary composition and nonalcoholic fatty liver disease. Dig Dis Sci. 2004;49:1578–83.
Wang D, Wei Y, Pagliassotti MJ. Saturated fatty acids promote endoplasmic reticulum stress and liver injury in rats with hepatic steatosis. Endocrinology. 2006;147(2);943–51.
Wendland BE. Nutritional guidelines for persons infected with the hepatitis C virus: a review of the literature. Can J Diet Pract Res. 2001;62(1):7–15.
Acknowledgments
This study has been supported by the Liver Disease Outcomes fund of the Center for Liver Diseases at Inova Fairfax Hospital, Inova Health System.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, C.H., Kallman, J.B., Bai, C. et al. Nutritional Assessments of Patients with Non-alcoholic Fatty Liver Disease. OBES SURG 20, 154–160 (2010). https://doi.org/10.1007/s11695-008-9549-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9549-0