
Background
We investigated the success rate of a twostage operative concept for treatment of morbid obesity: primary laparoscopic adjustable gastric banding (LAGB, Lap-Band®) for all morbidly obese patients, followed by sleeve gastrectomy with biliopancreatic diversion (duodenal switch or DS) in case of failure.
Methods
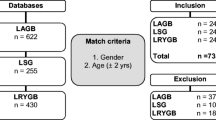
From Dec 1996 to May 2004, 366 consecutive patients (female 78%, mean age 41 (17–66) years, BMI 44.3 (35–75) kg/m2 were prospectively evaluated, using the two-stage operative concept. The follow-up rate after a mean of 4.1 (1–8.4) years was 98%. Primary outcome measure was BAROS score, defined according to weight loss, quality of life, reduction in co-morbidities, complications and re-operations.
Results
A very good-to-excellent result was found in 118 patients (32%), 141 (39%) had a goodresults, 76 (21%) a fair result, and 31 (8%) were failures. 39 patients needed re-banding due to slippage, 68 a DS, and 11 patients had band removal. Early morbidity of the Lap-Band® was 3.8%, that of DS 13%, and mortality was zero.The excess weight loss at last follow-up of all the patients was 44% (40% after Lap-Band®/rebanding, and 82% 2 years after DS).
Conclusion
The two-stage concept with primary LAGB, followed by DS in case of failure, leads to a good result in 71% of morbidly obese patients. LAGB alone does not appear to be an adequate procedure for every morbidly obese patient.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 2002; 16 287: 356–9.
Sjöström L, Lindroos A, Peltonen M et al. Lifestyle, diabetes, and cardiovascular risk factors 10 Years after bariatric ssurgery. N Engl J Med 2004; 351: 2683–93.
Maggard MA, Shugarman LR, Suttorp M et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med 2005; 142: 547–59.
Buchwald H, Avidor Y, Braunwald E et al. Bariatric surgery. A systemic review and meta-analysis. JAMA 2004; 292: 1724–37.
Buchwald H, Williams SE. Bariatric surgery worldwide surgery 2003. Obes Surg 2004; 14: 1157–64.
Solomon CG, Dluhy RG. Bariatric surgery – quick fix or longterm solution. N Engl J Med 2004; 351: 2751–3.
O’Brien PE, Dixon JB. Laparoscopic adjustable gastric banding in the treatment of morbid obesity. Arch Surg 2003; 138: 376–82.
Christou N, Sampalis J, Liberman M et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg 2004; 240: 416–424.
MacDonald KG, Long SD, Swanson MS et al. The gastric bypass operation reduces the progression and mortality of non-insulin-dependent diabetes mellitus. J Gastrointest Surg 1997; 1: 213–20.
Nguyen NT, Root J, Zainabadi K et al. Accelerated growth of bariatric surgery with the introduction of minimally invasive surgery. Arch Surg 2005; 140: 1198–1202.
Oria HE, Moorehead MK. Bariatric analysis and reporting outcome system (BAROS). Obes Surg 1998; 8: 487–99.
Woelnerhanssen B, Kern B, Peters T et al. Reduction in slippage with 11 cm Lap-Band® and change of gastric banding technique. Obes Surg 2005; 15: 1050–4.
Weiner RA. Gastric Banding: chirurgisch-technische Aspekte. Chirurg 2005; 76: 678–88.
Frigg A, Peterli R, Zynamon A et al. Radiologic and endoscopic evaluation for laparoscopic adjustable gastric banding: preoperative and follow-up. Obes Surg 2001; 11: 594–9.
Marceau P, Hould FS, Simard S et al. Bilio-pancreatic diversion with duodenal switch. World J Surg 1998; 22: 947–54.
Deitel M, Greenstein RJ. Recommendations for reporting weight loss (Editorial). Obes Surg 2003; 13: 159–60.
O’Brien PE, Dixon JB. Lap-band: outcomes and results. J Laparoendosc Adv Surg Tech A 2003; 13: 265–70.
Mittermair RP, Weiss H, Nehoda H et al. Laparoscopic Swedish adjustable gastric banding: 6-year follow-up and comparison to other laparoscopic bariatric procedures. Obes Surg 2003; 13: 412–7.
Weiner R, Blanco-Engert R, Weiner S et al. Outcome after laparoscopic adjustable gastric banding – 8 years experience. Obes Surg 2003; 13: 427–34.
Ponce J, Haynes B, Paynter S et al. Effect of Lap-Band®-induced weight loss on type 2 diabetes mellitus and hypertension. Obes Surg 2004; 14: 1335–42.
Branson R, Potoczna N, Kral JG et al. Binge-eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003; 348: 1096–103.
Branson R, Potoczna N, Brunotte R et al. Impact of age, sex and body mass index on outcomes at four years after gastric banding. Obes Surg 2005;15: 834–42.
Potoczna N, Branson R, Kral JG et al. Gene variants and binge-eating as predictors of co-morbidity and outcome of treatment in severe obesity. J Gastrointest Surg 2004; 8: 971–81.
Weber M, Muller MK, Bucher T et al. Laparoscopic gastric bypass is superior to laparoscopic gastric banding for treatment of morbid obesity. Ann Surg 2004; 240: 975–82.
Rubino F, Gagner M, Gentileschi P et al. The early effect of the Roux-en-Y gastric bypass on hormones involved in body weight regulation and glucose metabolism. Ann Surg 2004; 240: 236–42.
Peterli R, Donadini A, Peters T et al. Reoperations following laparoscopic gastric banding. Obes Surg 2002; 12: 851–6.
Brolin RE. Gastric bypass. Surg Clin North Am 2001; 81: 1077–95.
Frigg A, Peterli R, Peters T et al. Reduction in co-morbidities 4 years after laparoscopic adjustable gastric banding. Obes Surg 2004; 14: 216–23.
Weber M, Muller MK, Michel JM et al. Laparoscopic Roux-en-Y gastric bypass, but not rebanding, should be proposed as rescue procedure for patients with failed laparoscopic gastric banding. Ann Surg 2003; 238: 827–33.
Calmes JM, Giusti V, Suter M. Reoperative laparoscopic Roux-en-Y gastric bypass: an experience with 49 cases. Obes Surg 2005; 15: 316–22.
Biertho L, Steffen R, Branson R, et al. Management of failed adjustable gastric banding. Surgery 2005; 137: 33–41.
Hess DS, Hess DW. Biliopancreatic diversion with a duodenal switch. Obes Surg 1998; 8: 267–82.
Scopinaro N, Adami GF, Marinari GM et al. Biliopancreatic diversion. World J Surg 1998; 22: 936–64.
Nguyen NT, Longoria M, Gelfand DV et al. Staged laparoscopic Roux-en-Y: a novel two-stage bariatric operation as an alternative in the super-obese with massively enlarged liver. Obes Surg 2005; 15: 1077–81.
Regan JP, Inabnet WB, Gagner M et al. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg 2003; 13: 861–4.
Langer FB, Reza Hoda MA, Bohdjalian A et al. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg 2005; 15: 1024–9.
Mognol P, Chosidow D, Marmuse JP. Laparoscopic sleeve gastrectomy as an initial bariatric operation for high-risk patients: initial results in 10 patients. Obes Surg 2005; 15: 1030–3.
Milone L, Strong V, Gagner M. Laparoscopic sleeve gastrectomy is superior to endoscopic intragastric balloon as a first stage procedure for super-obese patients (BMI ≥50). Obes Surg 2005; 15: 612–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Peterli, R., Wölnerhanssen, B.K., Peters, T. et al. Prospective Study of a Two-Stage Operative Concept in the Treatment of Morbid Obesity: Primary Lap-Band® Followed if Needed by Sleeve Gastrectomy with Duodenal Switch. OBES SURG 17, 334–340 (2007). https://doi.org/10.1007/s11695-007-9061-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9061-y