
Abstract
For a balanced scapulohumeral rhythm in arm elevation, it is necessary to have an optimal position, motion, stability and muscle performance of the scapula and scapular muscles. In the case of abnormal movements, so-called scapular dyskinesis, the tendons (e.g. biceps tendon, rotator cuff) can be irritated and may cause pain in overhead activity. There are various causes for scapular dyskinesis and, therefore, the treatment is a challenge for therapists. The aim of conservative treatment is to restore normal position and movement of the scapula and furthermore dynamic scapular stability during overhead activities. Rehabilitation based on effective exercises should be tailored individually and the complexity of the exercises should be increased slowly.
Zusammenfassung
Für einen ausgeglichenen skapulohumeralen Rhythmus bei Armelevation ist eine optimale Position, Beweglichkeit, Stabilität und Muskelkraft der Skapula und der die Skapula umspannenden Muskulatur notwendig. Im Fall einer abnormen Bewegung der Skapula, Skapuladyskinesie genannt, können Sehnen (z. B. die Bizepssehne und Rotatorenmanschette) geschädigt werden, was zu Schmerzen bei Überkopfaktivität führen kann. Es gibt verschiedenste Ursachen für eine Skapuladyskinesie. Die Therapie ist daher eine Herausforderung für den Behandler. Das Ziel einer konservativen Therapie ist es, die normale Position und Bewegung der Skapula sowie darüber hinaus die dynamische Stabilität während Überkopfaktivität wiederherzustellen. Die Rehabilitation basiert auf einem effektiven Übungsprogramm und wird individuell angepasst, wobei die Komplexität der Übungen langsam gesteigert werden sollte.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
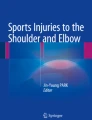
The scapula with the glenoid is the anchor for the humeral head and forms the origin of the rotator cuff as a basis for motions of the upper limb. Insufficient scapulohumeral motion implies a deficit of this anchorage. Physiologically, the scapula performs a complex three–dimensional movement during arm elevation including upward rotation, posterior tilting and varying internal/external rotation depending on the plane and angle of elevation [11, 27]. This is possible because of predominant muscular stabilization, besides the bony fixation of the clavicula, on the thorax with the upper and lower fibres of the trapezius, serratus anterior (“force couple”) and the posterior rhomboid muscle (Fig. 1). However, scapular dyskinesis (SD) is a divergence of the regular position and movement of the scapula [16, 18, 19].

Overview of periscapular muscles
Divergence during scapular dyskinesis
During arm elevation the lower trapezius (LT) with its attachment to the medial border allows the centring of the scapula rotation centre and supports the external rotation of the scapula [1]. Additionally, owing to its attachment on the margo inferior the muscle allows for a stabilization to the thorax during arm lowering. The other partner of the force couple is the serratus anterior muscle: It is a major stabilizer of the scapula and facilitates an upward rotation, posterior tilting and external rotation [26]. The position in external rotation and posterior tilting is necessary to allow for an optimal activation of the shoulder muscles during overhead activities such as throwing, especially during the cocking phase [33]. In concert with the muscles of the knee and hip in extension, plus a stable trunk (“kinetic chain”), the retracted scapula is a stabile anchor for the rotator cuff and therewith the humeral head for arm elevation. Maximal rotator cuff strength is achieved with a stable and retracted scapula [40].
Thus, SD itself is not a specific pathology, rather a symptom of one or more different pathologies and functional impairment. To date it is unclear whether SD is the cause or rather a consequence of shoulder pathologies. A study by Clarsen et al. examining Norwegian elite handball players showed that SD predicts shoulder pain [4]. Another prospective study by Struyf et al. evaluating recreational overhead athletes showed that the presence of SD did not influence the occurrence of shoulder pain [39]. However, the presence of SD may negatively influence specific shoulder pathologies. If an SD is not treated sufficiently, it can impair the healing of the underlying disease. A selection of pathologies are listed in Table 1.
Clinical examination
Patients with SD are typically young with nonspecific shoulder pain and irregular scapula motion. Nevertheless, SD is found not only in symptomatic patients, but also in healthy overhead athletes as an individual adaptation [14, 38]. Overhead sport such as volleyball, tennis, handball and swimming with repetitive abduction and external rotation may cause muscle imbalances and dyskinesis of the scapula. Dysfunction of the “force couple” and the kinetic chain is assumed to cause secondary impingement, which is not to be confused with classic outlet impingement of the shoulder. Thus, the recognition of deficits at different levels of the kinetic chain during physical examination is important in guiding proper treatment. In addition, the focus of the examination should be on pathology such as superior labral anterior–posterior (SLAP) or pulley lesions, rotator cuff tears and glenohumeral internal rotation deficit (GIRD).
The clinical examination of SD includes visual evaluation of the scapula, which is done from the dorsal side with bilateral repetitive arm elevation. Adding handheld weights may help to identify subtle SD, especially in athletes [22]. Results from visual assessment of SD can be classified according to Kibler into four types (Table 2; [19]), although other classifications exist:
However, during visual examination itself it is not possible to determine whether the position and/or movement of the scapula contribute to shoulder symptoms. Therefore, symptom alteration tests such as the scapular assistance test (SAT) or the modified SAT (mSAT) and the scapular retraction test (SRT) should be used [15, 21, 24, 40]. The SAT is performed while the examiner manually assists the upward rotation of the scapula during active elevation of the upper limb by pushing the inferior medial border of the scapula on the thorax [23]. The SAT was modified (mSAT) by Rabin et al. with inclusion of manual assistance of both upward rotation and posterior tilt [35]. Kopkow et al. demonstrated in a recently published study that the mSAT is reliable for clinical use, also if performed with additional handheld weights [24]. Positive symptom alteration test results will help identify patients in need of specific scapula-focused treatment. It is assumed that in the case of a positive test result, a scapula-specific treatment is promising [5, 8, 16].
Treatment
In the case of manifest structural pathologies such as glenohumeral instability with labral lesions, full thickness rotator cuff tear or SLAP lesions, an operative treatment should be considered as the basis of the treatment of SD. However, evidence regarding the influence of SD on outcomes after surgery is lacking and further studies evaluating this issue are needed. In patients with positive symptom alteration test results (SAT, mSAT or SRT) a preoperative scapula-specific treatment might help to improve postoperative outcomes. Nevertheless, in the case of primary or secondary muscular deficits throughout the complete kinetic chain, e.g. weakness of the serratus anterior and the trapezius muscle (force couple), the core trunk or lower extremity muscles, a structured and step-by-step physiotherapeutic treatment is recommended.
In throwing athletes with acute shoulder pain, a break from any overhead sporting activities is often necessary for pain management. Furthermore, a generally accepted conservative treatment with, e.g. NSAIDs and physical applications such as iontophoresis, electrical stimulation and cryotherapy should be always followed to diminish pain and inflammation for symptom reduction in patients with SD [36].
However, the aim of conservative treatment in patients with SD is to restore optimal scapula position and movement characterized by posterior tilt, external rotation and upward rotation during elevation of the upper limb. Therefore, the two basic pillars of pathology should be addressed in the case of pathological findings: the deficit of soft-tissue flexibility and the lack of muscle performance [5]. In general, it is recommended that isometric before dynamic exercises and training of proprioception before strength should be performed. In cases of deficit of soft-tissue flexibility, manual therapy and stretching exercises are indicated and in cases of lack of muscle performance, neuromuscular coordination and strength training. The exercises are gradual, beginning with training of the lower extremities and trunk stability (“core exercises”) as a prerequisite for correct posture and sufficient strength transfer from the lower to the upper extremity [37].
Rehabilitation of flexibility deficits
In cases of SD an internal rotation deficit of the glenohumeral joint caused by tenderness and stiffness of the posterior–inferior capsule and the external rotator muscle is often seen [17]. This leads to an anterior tilting and downward rotation of the scapula [2], causing impingement during active elevation of the upper limb. The “sleeper stretch” (Fig. 2) and the “cross-body stretch” (Fig. 3) have shown positive effects in improving the range of motion (ROM) and increasing the acromiohumeral distance [28, 31, 32]. Nevertheless, increasing internal rotation should be done carefully in the elite athlete, since this will probably decrease external rotation, which is essential for overhead athletes. In addition, the total ROM should be measured and considered before focusing solely on internal rotation [30].

Sleeper stretch (a frontal, b axial). Starting position: lying on the side using a head pad, pathological shoulder lying on the mattress, elbows bent at 90°, healthy hand holds the wrist of the pathological arm, own weight pushes the pathological arm down with minimal force (approximately 0.5 kg). [a Courtesy of Kopkow C, Dexel J, Kasten P (2015) Skapuladyskinesie. Klinische Untersuchung und Therapiestrategie. Zeitschrift für Physiotherapeuten 67:10–16]

Cross-body stretch (a frontal, b axial). Starting position: lying on the side using a head pad, pathological shoulder lying on the mattress, elbow flexed, arm is pulled across the body (up to pain level). [a Courtesy of Kopkow C, Dexel J, Kasten P (2015) Skapuladyskinesie. Klinische Untersuchung und Therapiestrategie. Zeitschrift für Physiotherapeuten 67:10–16]
Besides the posterior–inferior capsule, in particular the pectoralis minor and the levator scapulae muscle may cause flexibility problems and stretching exercises to treat such deficiencies have been published [10, 34]. The “corner stretch” (90° abduction and external rotation) seems to be an exercise with a large increase in the length of the pectoralis major [3], but this position will cause pain in most patients. Therefore, it is recommended to perform the exercise supine with passive stabilization of the scapula in a neutral position and with the assistance of a therapist [10]. However, whether a real elongation of the muscle or a sensory adaptation to the pain is the main effect is still debated [41].
Rehabilitation of muscular deficits
Before strengthening exercises, it should be ensured that no sensomotoric deficits of the kinetic chain exist. In cases of relevant deficits, simple exercises such as “knee bends” or “star excursion balance” (Fig. 4) may be used for conscious muscle control and to improve sensomotoric deficits and flexibility of the lower limb [20]. Core stability is achieved through “lateral forearm push-ups” because of a high activation of the gluteus medius and obliquus abdominis externus [9].

Star excursion balance exercise. Upright standing position, knees slightly bent, hands supported on hips, imagine a four-sided star on the floor, standing on one leg while trying to reach the end of the star sides as far as possible with the contralateral leg. Reach each of the eight points, five to eight repetitions
Especially during the acute phase with persistent shoulder pain and before beginning with the strengthening of the periscapular muscles, sensomotoric and isometric exercises to stabilize the scapula can be done parallel to core stabilization, because the shoulder is not to be moved dynamically [19, 23]. During the acute phase, exercises such as “scapula clock” (Fig. 5) and “inferior glides” (Fig. 6) are recommended and can be used to address conscious muscle control of scapular muscles [17, 23]. Holtermann et al. evaluated electromyography feedback systems for the learning of selective activation of scapular muscles and found promising clinical applications for restoring scapular muscle balance [13]. Exercises such as “low rows” can be applied, primarily isometric, and can be increased with decreasing pain in “mid” or “high rows” (Fig. 7).

Scapula clock exercise. Standing or in upright sitting position, a clock is used for visualization of scapula movement; the scapula is slowly moved into the different directions (3, 6, 9 and 12 o’clock). Each position should be reached once, 15 repetitions on each side. [Courtesy of Kopkow C, Dexel J, Kasten P (2015) Skapuladyskinesie. Klinische Untersuchung und Therapiestrategie. Zeitschrift für Physiotherapeuten 67:10–16]

Inferior glides. Standing or in upright sitting position, arm abducted up to 90°, fist clenched, the patient applies pressure with his/her fist in the direction of adduction and retracts/inferiorly and depresses the scapula. Hold end position for about 5 s, ten repetitions, three cycles

Low-row exercise. a Starting position: standing position, knees and trunk slightly flexed. b End position: extension of trunk and lower extremity, scapular retraction combined with low rows (elbows straight by the side). Hold end position for about 5 s, ten repetitions, three cycles. [b Courtesy of Kopkow C, Dexel J, Kasten P (2015) Skapuladyskinesie. Klinische Untersuchung und Therapiestrategie. Zeitschrift für Physiotherapeuten 67:10–16]
If no further sensomotoric deficits are present, the secondary focus should be in restoring muscle disbalances [6, 7, 25]. The upper trapezius (UT) muscle often shows hyperactivity in patients with SD, and thus exercises should be selected that activate the lower trapezius (LT) and the anterior serratus muscle (SA) [7]. Therefore, exercises with a low UT/LT and UT/SA ratio are of particular importance [23]. Through the high activation of the serratus anterior muscle “push-up plus” exercises appear to be very suitable in the closed chain. The therapy intensity could increase by combining the exercise with an ipsilateral extension of the leg through increasing activity of the SA muscle [29].
Training of muscular endurance and strengthening exercises
To change from the closed to the open kinetic chain exercises, “wall slides” exercises (Fig. 8) may be used, which activates the SA and also enables the patient to move the upper limb into overhead positions [12]. In the case of sufficient muscle stability of the scapula, “lateral pull”, “scapula punches” (Fig. 9) and “three-point plank with shoulder extension” exercises (Fig. 10) can be used in combination with “core exercises” for increasing intensity. At the end of rehabilitation, patients should be able to stabilize the scapula during their individual activities such as overhead sport but also work. Therefore, this needs to be addressed individually in the final rehabilitation phase [5].

Wall slides exercises. a Upright standing position, homolateral leg extended, sliding on the wall with actively retracted scapula. b Start under 90° abduction, then progress if there is no pain and the scapula can be stabilized

Scapula punches. a Starting position: upright standing position, resistance using elastic tubes and trunk rotation. b End position: extension of shoulders and elbows up to 120° of elevation and full protraction. Hold end position for about 5 s, ten repetitions, three cycles

Three-point plank with shoulder extension. a Three-point plank, elbow flexed 90° with light weight in the hand and followed by arm extension. b Hold end position for about 5 s, ten repetitions, three cycles
Return to play
Before athletes are able to return to play, sport-specific exercises should be performed to increase endurance and strength according to the individual sporting demands. Sufficient scapular stability and absence of pain during sport-specific exercises are needed before the athlete can return to sport. Cools et al. recommend (a) symmetrical scapular muscle strength in athletes not performing throwing sports and (b) 10 % increased strength on the dominant side in athletes performing unilateral overhead sporting activities [5]. Persistent pain and/or insufficient stability of the scapula will hamper return to sport. After returning to sport, athletes should be closely monitored for early detection of renewing problems and for adapting the sporting activities again to avoid long-term absence from sporting activities.
References
Bagg SD, Forrest WJ (1988) A biomechanical analysis of scapular rotation during arm abduction in the scapular plane. Am J Phys Med Rehabil 67(6):238–245
Borich MR, Bright JM, Lorello DJ, Cieminski CJ, Buisman T, Ludewig PM (2006) Scapular angular positioning at end range internal rotation in cases of glenohumeral internal rotation deficit. J Orthop Sports Phys Ther 36(12):926–934
Borstad JD, Ludewig PM (2006) Comparison of three stretches for the pectoralis minor muscle. J Shoulder Elbow Surg 15(3):324–330
Clarsen B, Bahr R, Andersson SH, Munk R, Myklebust G (2014) Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: a prospective cohort study. Br J Sports Med 48(17):1327–1333
Cools AM, Struyf F, De Mey K, Maenhout A, Castelein B, Cagnie B (2014) Rehabilitation of scapular dyskinesis: from the office worker to the elite overhead athlete. Br J Sports Med 48(8):692–697
Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC (2003) Scapular muscle recruitment patterns: trapezius muscle latency with and without impingement symptoms. Am J Sports Med 31(4):542–549
Cools AM, Witvrouw EE, Declercq GA, Vanderstraeten GG, Cambier DC (2004) Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement symptoms. Br J Sports Med 38(1):64–68
De Mey K, Danneels LA, Cagnie B, Huyghe L, Seyns E, Cools AM (2013) Conscious correction of scapular orientation in overhead athletes performing selected shoulder rehabilitation exercises: the effect on trapezius muscle activation measured by surface electromyography. J Orthop Sports Phys Ther 43(1):3–10
Ekstrom RA, Donatelli RA, Carp KC (2007) Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther 37(12):754–762
Ellenbecker TS, Cools A (2010) Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: an evidence-based review. Br J Sports Med 44(5):319–327
Giphart JE, van der Meijden OA, Millett PJ (2012) The effects of arm elevation on the 3-dimensional acromiohumeral distance: a biplane fluoroscopy study with normative data. J Shoulder Elbow Surg 21(11):1593–1600
Hardwick DH, Beebe JA, McDonnell MK, Lang CE (2006) A comparison of serratus anterior muscle activation during a wall slide exercise and other traditional exercises. J Orthop Sports Phys Ther 36(12):903–910
Holtermann A, Mork PJ, Andersen LL, Olsen HB, Sogaard K (2010) The use of EMG biofeedback for learning of selective activation of intra-muscular parts within the serratus anterior muscle: a novel approach for rehabilitation of scapular muscle imbalance. J Electromyogr Kinesiol 20(2):359–365
Kawasaki T, Yamakawa J, Kaketa T, Kobayashi H, Kaneko K (2012) Does scapular dyskinesis affect top rugby players during a game season? J Shoulder Elbow Surg 21(6):709–714
Kibler WB (1998) The role of the scapula in athletic shoulder function. Am J Sports Med 26(2):325–337
Kibler WB, Sciascia A (2010) Current concepts: scapular dyskinesis. Br J Sports Med 44(5):300–305
Kibler WB, Kuhn JE, Wilk K, Sciascia A, Moore S, Laudner K et al (2013) The disabled throwing shoulder: spectrum of pathology-10-year update. Arthroscopy 29(1):141–161
Kibler WB, Ludewig PM, McClure P, Uhl TL, Sciascia A (2009) Scapular Summit 2009: introduction. July 16, 2009, Lexington, Kentucky. J Orthop Sports Phys Ther 39(11):A1–A13
Kibler WB, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD (2013) Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the ‘Scapular Summit’. Br J Sports Med 47(14):877–885
Kibler WB, McMullen J, Uhl T (2001) Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am 32(3):527–538
Kibler WB, Sciascia A, Dome D (2006) Evaluation of apparent and absolute supraspinatus strength in patients with shoulder injury using the scapular retraction test. Am J Sports Med 34(10):1643–1647
Kibler WB, Sciascia A, Wilkes T (2012) Scapular dyskinesis and its relation to shoulder injury. J Am Acad Orthop Surg 20(6):364–372
Kibler WB, Sciascia AD, Uhl TL, Tambay N, Cunningham T (2008) Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med 36(9):1789–1798
Kopkow C, Lange T, Schmitt J, Kasten P (2015) Interrater reliability of the modified scapular assistance test with and without handheld weights. Man Ther. doi:10.1016/j.math.2015.04.012
Ludewig PM, Cook TM (2000) Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther 80(3):276–291
Ludewig PM, Cook TM, Nawoczenski DA (1996) Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther 24(2):57–65
Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, Laprade RF (2009) Motion of the shoulder complex during multiplanar humeral elevation. J Bone Joint Surg Am 91(2):378–389
Maenhout A, Van Eessel V, Van Dyck L, Vanraes A, Cools A (2012) Quantifying acromiohumeral distance in overhead athletes with glenohumeral internal rotation loss and the influence of a stretching program. Am J Sports Med 40(9):2105–2112
Maenhout A, Van Praet K, Pizzi L, Van Herzeele M, Cools A (2010) Electromyographic analysis of knee push up plus variations: what is the influence of the kinetic chain on scapular muscle activity? Br J Sports Med 44(14):1010–1015
Manske R, Wilk KE, Davies G, Ellenbecker T, Reinold M (2013) Glenohumeral motion deficits: friend or foe? Int J Sports Phys Ther 8(5):537–553
Manske RC, Meschke M, Porter A, Smith B, Reiman M (2010) A randomized controlled single-blinded comparison of stretching versus stretching and joint mobilization for posterior shoulder tightness measured by internal rotation motion loss. Sports Health 2(2):94–100
McClure P, Balaicuis J, Heiland D, Broersma ME, Thorndike CK, Wood A (2007) A randomized controlled comparison of stretching procedures for posterior shoulder tightness. J Orthop Sports Phys Ther 37(3):108–114
Meister K (2000) Injuries to the shoulder in the throwing athlete. Part one: biomechanics/pathophysiology/classification of injury. Am J Sports Med 28(2):265–275
Muraki T, Aoki M, Izumi T, Fujii M, Hidaka E, Miyamoto S (2009) Lengthening of the pectoralis minor muscle during passive shoulder motions and stretching techniques: a cadaveric biomechanical study. Phys Ther 89(4):333–341
Rabin A, Irrgang JJ, Fitzgerald GK, Eubanks A (2006) The intertester reliability of the Scapular Assistance Test. J Orthop Sports Phys Ther 36(9):653–660
Reinold MM, Gill TJ, Wilk KE, Andrews JR (2010) Current concepts in the evaluation and treatment of the shoulder in overhead throwing athletes, part 2: injury prevention and treatment. Sports Health 2(2):101–115
Sciascia A, Cromwell R (2012) Kinetic chain rehabilitation: a theoretical framework. Rehabil Res Pract 2012:853037
Silva RT, Hartmann LG, Laurino CF, Bilo JP (2010) Clinical and ultrasonographic correlation between scapular dyskinesia and subacromial space measurement among junior elite tennis players. Br J Sports Med 44(6):407–410
Struyf F, Nijs J, Meeus M, Roussel NA, Mottram S, Truijen S et al (2014) Does scapular positioning predict shoulder pain in recreational overhead athletes? Int J Sports Med 35(1):75–82
Tate AR, McClure PW, Kareha S, Irwin D (2008) Effect of the Scapula Reposition Test on shoulder impingement symptoms and elevation strength in overhead athletes. J Orthop Sports Phys Ther 38(1):4–11
Weppler CH, Magnusson SP (2010) Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther 90(3):438–449
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Nowotny, C. Kopkow, F. Mauch and P. Kasten state that there are no conflicts of interest.
The accompanying manuscript does not include studies on humans or animals.
Rights and permissions
About this article

Cite this article
Nowotny, J., Kopkow, C., Mauch, F. et al. Effective rehabilitation in patients with scapular dyskinesis. Obere Extremität 11, 40–46 (2016). https://doi.org/10.1007/s11678-015-0344-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-015-0344-y