
Abstract
Summary
Vitamin D deficiency is highly prevalent in Saudi Arabia, particularly among young women and is emerging as public health threat of epidemic proportions. Prevalence of severe hypovitaminosis D is expected to rise exponentially without primary intervention. This largest study encompasses extent of vitamin D deficiency and recommendations to reduce significant health care burden.
Introduction
The aim of the study was to determine the prevalence and significance of vitamin D deficiency in Saudi population and to help develop national consensus for its prevention, screening, and management.
Methods
This was a retrospective observational study which involved 10,709 patients, recruited from the Department of Family Medicine and Polyclinic, King Faisal Specialist Hospital and Research Center (KFSH&RC), Saudi Arabia, over a period of 5 years. The endpoints included overall status of vitamin D level and severity of vitamin D deficiency. Serum measurements included 25 hydroxyvitamin D (25(OH)D), parathormone, calcium, phosphate, alkaline phosphatase, albumin levels, eGFR levels, bone mineral density.
Results
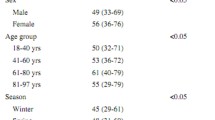
A total of 10,709 patients were analyzed; 31.4 % were males and 68.6 % were females, with a preponderance of Saudis (68.5 %) compared to non-Saudis (31.5 %). The prevalence of vitamin D deficiency was 83.6 % (31.9 % severe, 32.0 % moderate, and 19.7 % mild), when cut points of less than 25, 50, and 75 nmol/l, respectively, were used. Mean serum 25(OH)D was 44.58 ± 34.80 standard deviation (SD) nmol/l. There was significant difference in severity of vitamin D deficiency stratified by age, gender, and nationality. More females had severe 25(OH)D deficiency compared to males (35.6 vs. 23.7 %, p < 0.000). Severe 25(OH)D deficiency was markedly high among adolescents as compared to other age groups (49.2 vs. 30.9 %, p < 0.000). More Saudis were found to be vitamin D deficient compared to non-Saudis (37.2 vs. 20.3 %, p < 0.000).
Conclusion
The prevalence of hypovitaminosis D is significantly high among Saudi population, especially among women, despite abundant sunshine. It is a major public health concern and requires a robust health policy for vitamin D supplementation and implementation of dietary public health measures. Vitamin D screening is strongly recommended at an earlier age especially among women and children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vitamin D (1,25-dihydroxyvitamin D (1,25(OH)2D3)) is a pleotropic steroid with hormone-like activity. It is essential for calcium and bone homeostasis and has been recognized as a significant predictor of bone health. Vitamin D regulates more than 200 human genes in a wide variety of tissues [1]. Vitamin D deficiency continued to be an unrecognized epidemic among many populations with an estimated prevalence of over 1 billion people worldwide [2]. It has been reported in all age groups and genders. Vitamin D deficiency has been correlated with the increased risk of rickets and growth retardation in pediatric population, osteomalacia in adults, and hip fractures in the elderly [3]. Its deficiency has also been implicated in a number of systemic disorders including musculoskeletal system, colorectal cancer, breast cancer, autoimmune (e.g., IBD and IDDM), and cardiovascular diseases [4–8].
The clinical observation suggests that a significant number of Saudi populace has decreased levels of vitamin D in general. The objectives of this study was to determine the prevalence and significance of severe vitamin D deficiency ( 25(OH)D < 25 nmol/l) in Saudi population.
Patients and methods
This is a retrospective observational study to determine the trends and patterns of serum levels of vitamin D among Saudi population, using serum levels of 25-Hydroxy vitamin D [25(OH)D]. Data for 12,625 patients was collected in this study. However, data of 10,709 patients was analyzed. One thousand nine hundred sixteen patients were excluded from the final analysis for various reasons including lack of baseline vitamin D levels, already being on treatment for hypovitaminosis D, and incomplete data. The study population included all patients seen at the Department of Family Medicine and Polyclinic, King Faisal Specialist Hospital and Research Center (KFSH&RC) over 5 years from September 1, 2006 to March 6, 2011. The patients included the employees of the hospitals and their dependents of diverse nationalities and ethnic backgrounds. However, majority of the patients were Saudis from various parts of the kingdom (Table 1).
A baseline vitamin D screening test results encompassing D2, D3, and 25(OH)D levels, were collected for all patients. The data was collected from the hospital electronic medical information system (ICIS). Serum level of 25-hydroxy vitamin D was performed by high-performance liquid chromatography (HPLC) assay at the KFSH&RC Department of Pathology and Laboratory Medicine (DLPM). The study endpoints included determination of the prevalence and severity of vitamin D deficiency and its correlation with age, gender, and country of origin (Table 2). Additional variables included serum parathormone, calcium, phosphate, alkaline phosphatase, albumin levels, eGFR, and bone mineral density. Data was summarized either as percentage or mean ± standard deviation (SD). Vitamin D deficiency was defined as 25(OH)D levels below 75 nmol/l, severe deficiency as levels below 25 nmol/l, and optimum levels as 75–199 nmol/l [5]. The 25(OH)D levels between 50 and 75 nmol/l were considered to be mild deficiency of vitamin D.
The statistical software SPSS (version 20 by IBM) was used for data analysis. Chi-square is carried out to compare relative distributions, frequency, and severity of hypovitaminosis D in each group stratified by age, gender, and nationality. Patients were substratified into different age groups for comparative analysis with 25(OH)D levels. Data was summarized either as percentage or mean ± standard deviation (SD). The level of significance for inclusion in this model was set at p < 0.05. Descriptive statistics were used to present the basic demographic data. Independent Student’s t test was used to compare the mean values of vitamin D of males and females. Univariate and multivariate logistic regression were used to confirm the association of vitamin D deficiency with age, gender and nationality.
Results
This is the largest community based study in Saudi Arabia. A total of 10,709 patients were enrolled in this comprehensive vitamin D registry over a period of 5 years. Comparison of key explanatory and outcomes variables was done using this large database of detailed clinical information. Population was distributed by gender, age, and nationality. The 25(OH)D levels were stratified into four age groups: children, adolescent, adults, and elderly. The level of vitamin D was determined using the HPLC assay technique and stratified by multiple variables for comparative analysis. A statistically significant difference was found in the mean levels of vitamin D when stratified by gender, using chi-square and independent Student’s t test. The mean levels of 25(OH)D in the overall study population was 44.58 nmol/l (range = 0–714 nmol/l and SD ±34.80 nmol/l). Additional subanalysis indicated that mean serum level of D2 was 17.72 nmol/l and D3 was 31.43 nmol/l. When further stratified by gender, the mean 25(OH)D levels among males was 50.49 nmol/l as compared to 41.88 nmol/l among females.
Substratification by gender, age, and nationality were significant in defining 25(OH)D deficiency, using chi-square and multivariate binary logistic regression analysis. Females had significantly higher prevalence of severe vitamin D deficiency (35.6 % [n = 2,618 of 7,346]) as compared to males (23.7 % [797 of 3,363]; p < 0.000) (Table 2; Fig. 1). When stratified by nationality, the prevalence of severe deficiency of 25(OH)D was significantly higher among Saudi females compared to Saudi males including all age groups (42.6 % [2,055 of 4,828] vs. 27 % [676 of 2,505]; p < 0.000). Only 10.9 % Saudi women had optimum levels of serum vitamin D compared to 18.9 % of men. (Fig. 2).

25(OH)D deficiency status by gender

Levels of 25(OH)D in Saudi population. Severe vitamin D deficiency is more prevalent in Saudi women as compared to men (42.6 vs. 27 %). Only 10.9 % Saudi women have optimum serum levels of vitamin D compared to 18.9 % among men
Comparative analysis by age group delineated vitamin D deficiency as markedly elevated among adolescents as compared to other age groups (49.2 % [294 of 597] vs. 30.9 % [3,121 of 10,113]; p < 0.000). When stratified by age groups adjusted by nationality, the Saudi adolescents had significantly higher prevalence of severe 25(OH)D deficiency as compared to all other age groups among Saudi population (52.1 % [248 of 476] vs. 36.2 % [2,483 of 6,857]; p < 0.000). Further substratification by gender and nationality indicated that Saudi female adolescents had markedly increased prevalence of vitamin D deficiency compared to their male counterparts (62.7 % [190 of 303] vs. 33.5 % [58 of 173]; p < 0.000) (Table 3; Fig. 3).

Difference in vitamin D levels stratified by gender and age in the Saudi population
When stratified by nationality, the prevalence of severe hypovitaminosis D was significantly higher among Saudis compared to non-Saudis (37.2 % [2,731 of 7,333] vs. 20.3 % [684 of 3,376]; p < 0.000). Severe 25(OH)D deficiency was found to be more prevalent in Saudi adult population as compared to other nationalities (48.3 % [1,947 of 4,028] vs. 21.6 % [563 of 2,602]; p < 0.000). This significant difference was also noticed in other age groups. In non-Saudi population, patients from Middle East region had significantly higher level of severe 25(OH)D deficiency compared to other nationalities (31.9 % [864 of 1,268] vs. 13.3 % [280 of 2,108]; p < 0.000).
Comparative analysis by regional distribution indicated no difference in severe 25(OH)D deficiency levels among the study population, when compared by the cities of Riyadh and Jeddah (33.9 % [3,215 of 9,482] vs. 31 % [326 of 1,053]; p < 0.08).
Discussion
Although Saudi Arabia is one of the sunniest countries, vitamin D deficiency has been prevalent among Saudi population. The kingdom has one of the lowest levels of vitamin D, worldwide, among all age groups, especially adolescent women, children, and elderly. Vitamin D deficiency continues to be prevalent in the kingdom [9, 10] and has also led to increased hospitalizations due to rickets [11, 12].
The prevalence of hypovitaminosis D is significantly higher among Saudi population [13–15]. Saudi women have the highest prevalence of severe vitamin D deficiency compared to men [16, 17]. In our study, 44.6 % of Saudi women were found to have severe vitamin D deficiency as compared to 28.3 % in men. Ardawi et al. [18] reported around 80 % prevalence of hypovitaminosis D among 1,172 Saudi women from the western region of Saudi Arabia, while Sadat-Ali et al. [19] found 28 and 37 % prevalence of hypovitaminosis among male patients 25–35 years and ≥50 years old, respectively. Vitamin D deficiency among Saudi females is prevalent throughout the year, during summer and winter months [20, 21]. A high prevalence of vitamin D deficiency has also been reported among children in Saudi Arabia [22].
Among women, the young adolescent females have the significantly higher risk of severe vitamin D deficiency [9, 23–26]. Consequently, vitamin D deficient adolescents in this phase of growth and development are at increased risk of metabolic bone disorders especially rickets. Since clinical symptoms of Rickets are nonspecific, therefore, it is often underdiagnosed or missed [27]. Maintaining adequate levels of vitamin D during the adolescents age years can improve long-term health outcomes [28].
Several factors have been postulated for the low vitamin D level among Saudi women including dietary habits, lack of sun exposure, traditional clothing [29, 30], dark skin pigmentation, pregnancy, protracted lactation without vitamin D supplementation [31, 32], very hot climate, restricted outdoor activities, obesity, and lack of government regulation for vitamin D fortification of food. Our study found significantly lower levels of serum vitamin D2 as compared to vitamin D3. Vitamin D2 is derived from the food and vitamin D3 from exposure to sun light. Vitamin D contents of the food products in Saudi Arabia are mostly lower than recommended by the United States Code of Federal Regulations. There is none to suboptimal vitamin D fortification of the most commonly consumed foods in Saudi Arabia compared to the USA [33].
Vitamin D deficiency is highly prevalent in Saudi population, in general. However, further subanalysis indicated that adolescent women are the most vulnerable group susceptible to severe vitamin D deficiency in the kingdom. The etiology of this significant finding is multifactorial, in spite of the fact that there is abundance of year-round sunshine. Some of the plausible reasons are sociocultural, lifestyle, and dietary lack of vitamin D fortification and supplementation. A multi-prong approach is warranted to effectively manage this emerging public health threat of epidemic proportions. Education and awareness of the health importance of maintaining optimal circulating 25(OH)D and potential strategies to increase vitamin D intake, early on, is required for primary prevention. Clinicians and educators are encouraged to promote improved vitamin D intake and status, particularly among the high-risk groups like young and adolescent women. Early screening, detection, and intervention can effectively reduce the substantial health care burden in the kingdom by significantly reducing the risk of multiple chronic diseases, such as osteoporosis, cardiovascular disease, diabetes, and some cancers. Loco-regional consensus, comprehensive policies, and guidelines need to be established by the health authorities in conjunction with subject matter experts, health care providers, and scientists. Fortification and supplementation with vitamin D is significantly cost effective as compared to treatment of these chronic diseases. The Ministry of Health and regulatory authorities (SFDA, etc.) need to implement the vitamin D food fortification and develop individual supplementation protocols as per the established international guidelines and standards.
Conclusion
The prevalence of hypovitaminosis D is significantly higher among Saudi population, especially among women. Despite ample sunshine, women are at an inordinate risk of hypovitaminosis D, most likely due to low ultraviolet B radiation exposure, increased skin pigmentation, cultural and lifestyle variations, dietary factors, and lack of supplementation and fortification. Additional longitudinal vitamin D supplementation studies with multiple noncalcemic endpoints are indicated to define the benefits of an optimal vitamin D status in order to establish national consensus guidelines. In addition to culturally sensitive education and awareness, lifestyle modifications, loco-regional screening, and treatment guidelines are needed. Vitamin D screening should be considered early on in children and young women, especially among pregnant or lactating. People at most risk for vitamin D deficiency should be advised to increase their dietary calcium and vitamin D supplements and increased exposure to sunlight. Saudi FDA may have to look into increasing the quantity of vitamin D fortification to reduce highly prevalent vitamin deficiency and reduce significant health care burden as a sequel of hypovitaminosis in the kingdom.
References
Cannell JJ, Hollis BW (2008) Use of vitamin D in clinical practice. Altern Med Rev 13(1):6–20
Holick MF, Chen TC (2008) Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 87(4):1080S–1086S
Chapuy MC et al (1992) Vitamin D3 and calcium to prevent hip fractures in the elderly women. N Engl J Med 327(23):1637–1642
Garland CF et al (2007) Vitamin D and prevention of breast cancer: pooled analysis. J Steroid Biochem Mol Biol 103(3–5):708–711
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357(3):266–281
Looker AC et al (2008) Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am J Clin Nutr 88(6):1519–1527
Freedman DM et al (2007) Prospective study of serum vitamin D and cancer mortality in the United States. J Natl Cancer Inst 99(21):1594–1602
Yousef FM et al (2013) Vitamin D status and breast cancer in Saudi Arabian women: case–control study. Am J Clin Nutr 98(1):105–110
Siddiqui AM, Kamfar HZ (2007) Prevalence of vitamin D deficiency rickets in adolescent school girls in Western region, Saudi Arabia. Saudi Med J 28(3):441–444
Al-Jurayyan NA et al (2002) Nutritional rickets and osteomalacia in school children and adolescents. Saudi Med J 23(2):182–185
Al-Atawi MS et al (2009) Epidemiology of nutritional rickets in children. Saudi J Kidney Dis Transpl 20(2):260–265
Abanamy A et al (1991) Vitamin D deficiency rickets in Riyadh. Ann Saudi Med 11(1):35–39
Naeem Z et al (2011) Vitamin D status among population of Qassim Region, Saudi Arabia. Int J Health Sci (Qassim) 5(2):116–124
Elsammak MY et al (2010) Vitamin d deficiency in Saudi Arabs. Horm Metab Res 42(5):364–368
Mohammed S et al (1993) Serum calcium, parathyroid hormone, and vitamin D status in children and young adults with sickle cell disease. Ann Clin Biochem 30(Pt 1):45–51
Elshafie DE, Al-Khashan HI, Mishriky AM (2012) Comparison of vitamin D deficiency in Saudi married couples. Eur J Clin Nutr 66(6):742–745
Al-Mogbel ES (2012) Vitamin D status among Adult Saudi females visiting primary health care clinics. Int J Health Sci (Qassim) 6(2):116–126
Ardawi MS et al (2011) Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and vitamin D receptor genotypes in healthy Saudi pre- and postmenopausal women. Osteoporos Int 22(2):463–475
Sadat-Ali M et al (2009) Vitamin D levels in healthy men in eastern Saudi Arabia. Ann Saudi Med 29(5):378–382
Kanan RM et al (2013) Year-round vitamin D deficiency among Saudi female out-patients. Public Health Nutr 16(3):544–548
Alsuwadia AO et al (2013) Prevalence of vitamin D deficiency in Saudi adults. Saudi Med J 34(8):814–818
Mansour MM, Alhadidi KM (2012) Vitamin D deficiency in children living in Jeddah, Saudi Arabia. Indian J Endocrinol Metab 16(2):263–269
Al-Ghamdi MA, Lanham-New SA, Kahn JA (2012) Differences in vitamin D status and calcium metabolism in Saudi Arabian boys and girls aged 6 to 18 years: effects of age, gender, extent of veiling and physical activity with concomitant implications for bone health. Public Health Nutr 15(10):1845–1853
Al-Daghri NM et al (2010) Severe hypovitaminosis D is widespread and more common in non-diabetics than diabetics in Saudi adults. Saudi Med J 31(7):775–780
Al-Turki HA et al (2008) 25-Hydroxyvitamin D levels among healthy Saudi Arabian women. Saudi Med J 29(12):1765–1768
Palacios C, Gonzalez L (2013) Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol
Abdullah MA et al (2002) Adolescent rickets in Saudi Arabia: a rich and sunny country. J Pediatr Endocrinol Metab 15(7):1017–1025
Stoffman N, Gordon CM (2009) Vitamin D and adolescents: what do we know? Curr Opin Pediatr 21(4):465–471
Gannage-Yared MH et al (2000) Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J Bone Miner Res 15(9):1856–1862
Jamali Z et al (2013) Vitamin D status in female students and its relation to calcium metabolism markers, lifestyles, and polymorphism in vitamin D receptor. Clin Lab 59(3–4):407–413
Fields J et al (2011) Vitamin D in the Persian Gulf: integrative physiology and socioeconomic factors. Curr Osteoporos Rep 9(4):243–250
Christie FT, Mason L (2011) Knowledge, attitude and practice regarding vitamin D deficiency among female students in Saudi Arabia: a qualitative exploration. Int J Rheum Dis 14(3):e22–e29
Sadat-Ali M et al (2013) Fortification with vitamin D: comparative study in the Saudi Arabian and US markets. J Fam Community Med 20(1):49–52
Acknowledgments
Skillful assistance provided by Ms. Sahar Iqbal in the preparation of this manuscript is gratefully acknowledged by the authors.
Conflicts of interest
Ethical considerations: The research project was conducted in accordance with the guiding principles for experimental procedures written in the Declaration of Helsinki of the World Medical Association, and the NIH Guide for the Care and Use of Laboratory Animals, 1985, contained in the Declaration of Helsinki (2000) and is approved by the institutional review board of KFSH&RC. It complies with the policies of the Research Advisory Committee (RAC) at KFSH&RC and the laws of the Kingdom of Saudi Arabia.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hussain, A.N., Alkhenizan, A.H., El Shaker, M. et al. Increasing trends and significance of hypovitaminosis D: a population-based study in the Kingdom of Saudi Arabia. Arch Osteoporos 9, 190 (2014). https://doi.org/10.1007/s11657-014-0190-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-014-0190-3