
Abstract
Summary
This study aimed to estimate the incidence rate of hip fracture during 2008–2010 in Shiraz, Iran. Overall, the standardized age-related incidence were 329.6/100,000 in men and 1,589.7/100,000 in women. The incidence rate in females was remarkably higher than the previous studies in Iran.
Purpose
This study aims to determine the incidence rate of hip fracture and its possible changes during 2008–2010 in Shiraz, Iran.
Materials and methods
This study reviewed and abstracted the hospital records, demographic, and clinical data of 1,923 patients aged 50 years or older with first time hip fracture admitted to private and public hospitals of Shiraz, Iran during 2008–2010 The age-adjusted incidence rate of hip fracture was determined along with association between gender, age, site of fracture, and socioeconomic status (SES) with the incidence rate.
Results
The mean age of subjects was 74.7 years (±10.6 years). Age-adjusted incidence rates for hip fracture, standardized to the 2000 US white male and female populations were 329.57 and 1,589.71 per 105, respectively, while totally it was 461.1 per 105. The incidence rate of hip fracture in females was higher than that of males in their 60s (1,229.2 versus 793.3), 70s (4,130.3 versus 2,835.3), and early 80s (4,506.8 versus 3,820.5) per 100,000. The hip fracture incidence in high SES area (157.1 per 100,000) followed by low SES regions (152.5 per 100,000) were higher compared to middle SES area (38.1 per 100,000) and towns around Shiraz (27.7 per 100,000) with fracture of the neck of femur being the most frequent affliction (391 per 100,000).
Conclusions
The rate of hip fracture is increasing in the area under study particularly in women and to a greater extent in those aged 60 years or older. Therefore, it is necessary to pay special attention to primary and secondary prevention of hip fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis, the most common metabolic disease of bone, weakens the bone and increases the risk of fracture. This disease is known as a silent illness which develops without any sign until the fracture happens by minor activity [1, 2]. The most serious clinical outcome of osteoporosis is hip fracture [3].
Hip fracture, as one of the most important causes of disability and death among the elderly, is rapidly increasing. The hip fracture is expected to rise with increasing age. This is evident by rapid increase in the number of elderly in some Asian countries [4].
Hip fracture accounts for majority of direct medical cost to the community [3]. The annual cost for treatment of asthma and congestive heart failure in the USA is $6.2 and $7.5 billion, respectively, while this amounts to $13.8 billion for treatment of osteoporosis and its sequel [5]. Thus, prevention of osteoporosis before massive bone mass loss is very important and even secondary prevention is necessary for those who have experienced osteoporotic fracture [5]. Incidence of hip fracture varies greatly among different countries. Approximately a tenfold difference in age-adjusted incidence of hip fracture is observed between different countries [6, 7]. Denmark, Sweden, Norway, England, and Canada have higher incidence of hip fracture than Germany, China, Taiwan, Hong Kong, Singapore, Japan, and other Asian countries [7].
Compared to men, a lower bone mineral density is seen in women. Women also have a longer life span and a higher rate of bone loss, especially in the period of estrogen deficiency which is in their 50s and 60s [7]. Bone mass is higher in men and harmonic changes needed for osteoporosis develops slowly and gradually in women [8, 9]. However, men with osteoporosis are more susceptible to fracture and death [9–11].
Since Iranian population is growing old, policymakers need some basic data to be used for further strategic planning. The most important measure is access to the latest information about osteoporosis in the population, either directly by bone densitometry or indirectly by estimating different items such as the incidence of osteoporosis-induced hip fracture. The aim of this study was to determine the incidence rate of hip fracture and its possible implications from 2008 to 2010 in southwest Iran.
Materials and methods
This study was conducted in Shiraz, the capital city of Fars province, the fifth populated city in Iran with 223.4 km2 and located at latitude of 29°38′ N and longitude of 52°34′ E. Shiraz has 16 hospitals where orthopedic surgeries are performed. Of these, four hospitals are university teaching hospitals, and the rest are private. A review of unpublished data reported by Shiraz University of Medical Sciences showed that more than 95 % of hip fractures are admitted to the teaching hospitals and five private hospitals. All these hospitals were included in our study.
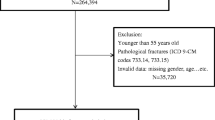
This retrospective study comprised patients older than 50 years who lived in Shiraz and experienced a hip fracture from 1 January 2008 to 1 January 2011. Having the local ethics committee approved our study, hospital records of all patients with hip fracture, filed according to International Classification of Diseases, tenth edition (ICD-10), in the foregoing hospitals, were carefully reviewed to determine the incidence of hip fracture. The data obtained were abstracted from the operation room logs and discharge sheet and included age, sex, residence, type of hip fracture according to ICD-10, cause of fracture, socioeconomic status based on residence, co-existing diseases such as diabetes mellitus, hypertension, cerebrovascular accidents, myocardial infarction, asthma, rheumatoid diseases, thyroid diseases, and Parkinson along with history of smoking and/or opium addiction. All patients from Shiraz with hip fracture were identified using relevant codes and computerized hospital records saved under hip fracture. The following patients were excluded from our study:
-
Patients with fractures except intertrochanteric, neck of femur, subtrochanteric, and a combination of these fractures and/or subcapital and transcervical fractures referred to as “other” in our analysis.
-
Fractures due to major trauma such as traffic accidents or falling from more than 2 m.
-
Fractures induced by cancer, diseases (except for osteoporosis), and medication.
The number of subjects aged 50 years and older was estimated from reports of Fars population 2008–2010, issued by Fars Management and Organization. This was then applied to the 2006 national census for estimation of each 5-year age group. Age-adjusted incidence rates were standardized and calculated directly based on the 2000 US white population [12].
Shiraz is divided into nine municipality districts. Regions 1, 3, and 6 are located in the northern part; regions 2 and 9 in the southern part; region 7 in the eastern part; region 4 in the western part; and regions 5 and 8 in the central part of the city. Region 4 has the largest population, and region 8 has the smallest population. Regions 2 and 3 have the largest and smallest area, respectively. Overall, the populations living in the northern part of the city have the highest socioeconomic status (SES) and those coming from the south have the lowest SES. Therefore, each patient was placed into high, middle, or low SES based on his or her address saved in the hospital file.
Data were analyzed by SPSS software version 16. Chi-square test or Fisher’s exact tests were used to find the differences in incidence rates in males and females, and p < 0.05 was considered as significant.
Results
This study included 1,923 patients, aged 50 years or older, with hip fracture, standardized to the 2000 US white population, admitted to the public and private hospitals in Shiraz over a period of 3 years.
The mean age of the subjects was 74.7 ± 10.6 SD years and no significant difference (p = 0.33) in age was found between males (74.5 ± 11.1) and females (74.9 ± 10.3 SD).
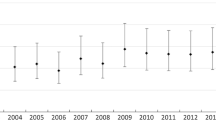
Total incidence rate in females was 890.1 per 100,000 which was significantly higher than males (711.3 per 100,000; p < 0.001). As shown in Fig. 1, a statistically significant descending trend was found in the incidence rate of hip fracture between2008 and 2010 (p < 0.001).

The incidence of hip fracture per 100,000 in Shiraz, Iran during 2008–2010
Age-adjusted incidence rates of hip fracture, standardized to the 2000 US white population, were 329.57 and 1,589.71 per 105 populations in male and female, respectively, and 461.1 per 105 in total.
This study showed that in subjects aged 50 years or over, the incidence rate of hip fracture rose by increasing age, which was prominently higher in 60 years or older females (Table 1).
The incidence rate of intertrochanteric fracture was higher in females than males (384.9 versus 334.9, p = 0.06) but this difference was not statistically significant. The rate of fractures of neck of the femur was significantly higher in females compared to males (391 versus.243.4, p < 0.001). The rates of subtrochanteric and other fractures were higher in males which compared to females it was not statistically significant. Table 2 demonstrates age-specific rates of various sites of fracture in both genders.
Of the cases, 44 are of unknown residence and of 1,879 patients with known abode; 1,776 (94.5 %) patients came from Shiraz and 103 patients lived in small towns around Shiraz, where there were no suitable hospitals. The highest rate of hip fracture (157.06 per 105) was detected in high socioeconomic areas, which was not significantly different from low socioeconomic regions (152.47 per 105). The lowest incidence rates were observed in middle areas (38.15 per 105) which were not significantly different (p = 0.26) from small towns around Shiraz (27.75 per 105). However, a significant difference in the incidence rates of hip fracture was found between high and low SES compared to middle SES and small towns (p < 0.001; Fig. 2).

The incidence of hip fracture per 100,000 according to patients’ residence in Shiraz, Iran from 2008 to 2010
Of 1,923 patients with hip fractures, orthopedic specialists prescribed calcium D for 37 (1.9 %), vitamin D for 17 (0.9 %), and calcium for 3 cases (0.15 %). Vitamin D and calcium was prescribed for one (0.05 %) patient.
At least one coexisting disease was recorded in 1,195 out of 1,923 (62.1 %) hospital files. Females had a significantly higher proportion of a coexisting disorder than males (60.8 % versus. 39.2 %; p < 0.001).In this context, hypertension was the most common (39.4 %) next to diabetes mellitus (16.8 %). Frequencies of other noncommunicable diseases are shown in Table 3.
Cigarette smoking and/or opium addiction were reported in 295 (15.3 %) patients, involving a higher proportion of men compared to women (66.8 % versus. 33.2 %; p < 0.001).
Discussion
According to our findings, the age-dependent incidence rates for hip fracture (per 100,000), standardized to the 2000 US white population, were 329.57 in males and 1,589.71 females. A study carried out in Shiraz by Soveid et al., on cases occurring from March 2001 to March 2003 showed the age-dependent incidence rates (per 100,000) of hip fracture, standardized to the 1989 US white population, to be 384.61 for men and 548.17 for women [13]. In Kuwait, which is located in the southwestern border of Iran, the age-standardized incidence rate (per 100,000) of hip fracture was 295 in females and 200 in males, which was comparable to some of the western European and North American populations [4]. However, contrary to Soveid et al. [13], our study was conducted in different area of Shiraz from 2008 to 2010 with the incidence rates standardized to the 2000 US white population, and using the same exclusion and inclusion criteria. This might help compare the results of two studies in relation to the changing pattern of hip fracture incidence in this region from 2003 to 2009. Surprisingly, the incidence rate in women has risen compared to previous study. A multicenter study on cases occurring in summer 2003 in nine provinces of Iran reported the age-related incidence rates (per 100,000), standardized to the 2000 US population to be 127.3 in men and 164.6 in women. It was concluded that hip fracture in Iranian women is lower than other Asian countries and is close to the rates from China [14]. Also, Beyranvand et al. showed that the annual age-standardized incidence rates were 181.1/100,000 in men and 214.6/100,000 in women in Kermanshah, a city located in western Iran, which were lower than the incidence rates reported in our study [15]. Considering the results of similar studies reported from other parts of Iran, it appears that the incidence rate of hip fracture is lower than the previous study in Shiraz [13]. Based on worldwide annual number of 1.66 millions of hip fracture in 1990 [16], it is estimated that this number will rise to 6.26 by 2050 [17]. The changes in demographic characteristics, osteoporosis and other systemic diseases, medications, life style, and nutrition associated with the risk of hip fracture [18] could account for increasing incidence of hip fracture in women. As the results of our study indicate, only 3 % of the subjects had received medications for osteoporosis even after a hip fracture. This is indicative of the very low attention paid to the osteoporosis in our community. Decline in physical activity and increase in minor traumas may be another reason for this rise [19]. A fourfold increase in incidence of hip fracture, from 1991 to 2001, was also reported by a Korean study [20]. A remarkable and significant rise in the incidence rate of hip fracture in women, but not in men was also reported in Belgrade from 1990 to 2000 [21]. Most studies from Iran and other countries indicated a higher rate of hip fracture among women than men [4, 13, 14, 20, 22–27]. However, In India and China, more hip fractures were more prevalent in men than in women (F:M = 0.8 and 0.9) [3].
In our study, the rate of fracture in femoral neck was significantly higher in women than men. Although women had a higher rate of intertrochanteric fracture than men, this difference was not significant. Soveid et al. reported a comparable pattern of fracture of the femoral neck; however, intertrochanteric fracture was significantly higher among women while subtrochanteric and other fractures had approximately the same rates in men and women [13]. Intertrochanteric fracture was the most common site in our study which was consistent with the results of other investigations [13, 14, 21].
We found the highest rate of hip fracture in affluent regions. Areas with low SES had a high rate of hip fracture but lower, but not significantly, than prosperous areas. Middle areas and small towns had significantly lower rates. This was in agreement with the previous study from Shiraz which reported the highest rate in affluent areas. It seems that the impact of SES on osteoporosis varies in different geographical areas or it may still be controversial. Studies from Norway [28, 29] reported that osteoporosis was more prevalent in lower SES areas in contrast to other studies from New Zealand [18, 30] where osteoporosis was reported to be more prevalent in sectors with high SES.
Our study had several limitations, the most important of which was dependence on previously recorded data, which could not prove the presence of osteoporosis in included cases. In addition, there could be few cases that did not refer to hospitals or admitted to the hospitals in other cities.
In summary, the rate of hip fracture, particularly among women, is increasing in the area under our study. Increasing awareness regarding osteoporosis and its primary prevention will have an important impact on decreasing the rate of hip fracture as well as its costs and implications.
References
Watts NB, Lewiecki EM, Miller PD, Baim S (2008) National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis and the World Health Organization Fracture Risk Assessment Tool (FRAX): what they mean to the bone densitometrist and bone technologist. J Clin Densitom 11:473–477
Kanis JA (1997) Diagnosis of osteoporosis. Osteoporos Int 7(Supp. 3):SI08–SI116
Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 15(11):897–902
Memon A, Pospula WM, Tantawy AY, Abdul-Ghafar S, Suresha A, Al-Rowaih A (1998) Incidence of hip fracture in Kuwait. Int J Epidemiol 27:860–865
Petrella RJ, Jones TJ (2006) Do patients receive recommended treatment of osteoporosis following hip fracture in primary care? BMC Fam Pract 7:31
Johnell O, Gullberg B, Allander A, Kanis JA (1992) The apparent incidence of hip fracture in Europe. Osteoporos Int 2:298–302
Kanis JA, Oden A, McCloskey EV, Johansson H, Wahl DA, Cooper C (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23(9):2239–2256
Prelevic GM (2001) Osteoporosis in men. J R Soc Med 94(12):620–623
Khosla S (2010) Update in male osteoporosis. J Clin Endocrinol Metab 95(1):3–10
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17(12):1726–1733
Ebeling PR (2008) Osteoporosis in men. N Engl J Med 358(14):1474–1482
Gordis L (2008) Epidemiology, 4th edn. Saunders, New York, pp 90–91
Soveid M, Serati AR, Masoompoor M (2005) Incidence of hip fracture in Shiraz, Iran. Osteoporos Int 16(11):1412–1416
Moayyeri A, Soltani A, Larijani B, Naghavi M, Alaeddini F, Abolhassani F (2006) Epidemiology of hip fracture in Iran: results from the Iranian Multicenter Study on Accidental Injuries. Osteoporosis 17(8):1252–1257
Beyranvand M, Mohammadi G (2009) Incidence of hip fracture in Kermanshah, Iran. Arch Osteoporos 4:67–70
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a worldwide projection. Osteoporos Int 2:285–289
Melton LJ (1993) Hip fractures: a worldwide problem today and tomorrow. Bone 14(Suppl 1):S1–S8
Benetos IS, Babis GC, Zoubos AB, Benetou V, Soucacos PN (2007) Factors affecting the risk of hip fractures. Injury 38(7):735–744
Harvey N, Dennison E, Cooper C (2009) Epidemiology of osteoporotic fractures. In: Rosen CJ (ed) Primer on the metabolic bone disease and disorders of mineral metabolism, 7th edn. American Society for Bone and Mineral Research, Washington D.C., pp 198–203
Rowe SM, Song EK, Kim JS, Lee JY, Park YB, Bae BH et al (2005) Rising incidence of hip fracture in Gwangju City and Chonnam Province, Korea. J Korean Med Sci 20(4):655–658
Lesic A, Jarebinski M, Pekmezovic T, Bumbasirevic M, Spasovski D, Atkinson HD (2007) Epidemiology of hip fractures in Belgrade, Serbia Montenegro, 1990–2000. Arch Orthop Trauma Surg 127(3):179–183
Xu L, Lu A, Zhao X, Chen X, Cummings SR (1996) Very low rates of hip fracture in Beijing, People’s Republic of China the Beijing Osteoporosis Project. Am J Epidemiol 144(9):901–907
Melton LJ, Crowson CS, O’Fallon WM (1999) Fracture incidence in Olmsted County, Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int 9:29–37
Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dawson A et al (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11(8):669–674
Lau EM, Lee JK, Suriwongpaisal P, Saw SM, De Das S, Khir A et al (2001) The incidence of hip fracture in four Asian countries: the Asian Osteoporosis Study (AOS). Osteoporos Int 12(3):239–243
Lofthus CM, Osnes EK, Falch JA, Kaastad TS, Kristiansen IS, Nordsletten L et al (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29(5):413–418
Castro da Rocha FA, Ribeiro AR (2003) Low incidence of hip fractures in an equatorial area. Osteoporos Int 14(6):496–499
Meyer HE, Tverdal A, Falch JA (1993) Risk factors for hip fracture in middle-aged Norwegian women and men. Am J Epidemiol 137(11):1203–1211
Kaastad TS, Meyer HE, Falch JA (1998) Incidence of hip fracture in Oslo, Norway: differences within the city. Bone 22(2):175–178
Elliot JR, Gilchrist NL, Wells JE (1996) The effect of socioeconomic status on bone density in a male Caucasian population. Bone 18(4):371–373
Acknowledgments
We would like to express our particular appreciation to the Health Policy Research Center for financial support.
Conflicts of interest
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maharlouei, N., Khodayari, M., Forouzan, F. et al. The incidence rate of hip fracture in Shiraz, Iran during 2008–2010. Arch Osteoporos 9, 165 (2014). https://doi.org/10.1007/s11657-013-0165-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-013-0165-9