
Abstract
Summary
We investigated bone mineral density (BMD) and analyzed the changes in peak bone mass and BMD in Chinese Han population. The main results are as follows: (1) The peak BMD in males (0.625 ± 0.109) and females (0.506 ± 0.058) was observed at the age of 30–34 years; (2) osteoporosis prevalence was 7.7% vs. 6.97% in males and females aged 50–59 years; 18.13% vs. 35.97% in males and females aged 60–69 years; 36.41% vs. 59.55% in males and females aged 70–79 years; and 57.53% vs. 75.56% in males and females aged >80 years; (3) BMD differed significantly between genders, and among age groups studied; and (4) peak BMD of Han Chinese was greater than that of Japanese and Danish, as well as ethnicities in China.
Purpose
The reference data on BMD and osteoporosis among Chinese people are lacking. We, therefore, investigated the BMD and analyzed the changes in peak bone mass and BMD in Han population.
Methods
BMD at the one third of distal radius and ulna of non-dominant forearm was measured by DTX-200 BMD detector in 16,019 Han individuals in Changchun divided into different groups based on age and gender. The mean BMD, T-score, and bone loss rate were analyzed using SPSS 13.0 statistical software.
Results
The peak BMD in males and females was 0.625 ± 0.109 and 0.506 ± 0.058, respectively, which was observed in the age group of 30–34 years. BMD decreased gradually after 40 years. The prevalence of osteoporosis was as follows: 7.7% in males and 6.97% in females in the age group of 50–59 years; 18.13% in males and 35.97% in females aged 60–69 years; 36.41% in males and 59.55% in females aged 70–79 years; and 57.53% in males and 75.56% in females aged over 80 years.
Conclusions
There was a significant difference (P < 0.01) in BMD in different age groups and between genders within the same age group. In different age groups, the prevalence of osteoporosis was significantly higher in females than in males (P < 0.01). The peak BMD in this region was higher than that reported in Japan and Denmark, and was comparable to that in Beijing. Furthermore, differences were significant (P < 0.01) as Han population of Changchun was compared with Dai population of Xishuangbanna, Tibet, and Dongxiang population of Gansu province.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis (OP) is a multifactorial disease associated with an increased risk of fracture and is caused by low bone mass, destruction of bone structure, and decline in bone strength. The differences exist in bone mineral density (BMD) among people with the same gender and similar age, as well as due to variable hereditary, nutrition, physical activity, age, gender, and environmental factors. Previously, a number of BMD studies were conducted in individuals from different nationalities and/or geographical regions, such as Han and Uygur nationalities (2,297 individuals) from Urumqi, China [1], normal individuals (546) living in coastal areas of Guangdong province of China [2] as well as in Japanese [3] and Danish [4] populations.
Studying the patterns of BMD variation among people of different regions, nationalities, ages, and genders is important not only for early detection of the disease but also for devising effective preventive and treatment strategies. At present, the data regarding comparison of the peak BMD values and OP prevalence among large ethnic groups from different regions of China are lacking. We, therefore, analyzed the peak bone mass and BMD profile of 16,019 people of Han nationality from Changchun province of China and compared the data with those of other groups with respect to age, gender, race, and geographical region.
Here, we present the evidence that BMD differed significantly (P < 0.01) between different age groups, as well as between genders within the same age group. Our data show that the prevalence of osteoporosis was significantly higher in females than in males (P < 0.01). The peak BMD in Changchun province was comparable to that in Beijing, but higher than that in Japan and Denmark. As well, there were significant differences (P < 0.01) observed as the Han population of Changchun was compared with Dai population of Xishuangbanna, Tibet, and Dongxiang population from Gansu province.
Methods
Study population
In this study, 16,019 individuals of Han nationality, aged 20–89 years, were recruited from Changchun city, China. This population represented different social settings such as government, industry, school, business, and retired people. The data collected included life history, ancestral history, family history, medical history, sports, special medication, etc., and in case of females, it also included menstrual history, childbearing history, and breastfeeding history. Acute or chronic hepatic, renal, and endocrine diseases were excluded.
BMD measurement
BMD at the one third of distal radius and ulna of non-dominant forearm was measured by using DTX-200 BMD detector (American Osteometer MediTech Inc.). The data were used to calculate mean BMD, T-score, and bone loss rates. BMD values of 16,019 individuals of Han nationality from Changchun were compared with those reported by other studies using similar measurements among individuals of both genders and similar age groups from Beijing (Han), Xishuangbanna (Dai), Tibet (Tibetan), Gansu (Dongxiang), Japan, and Denmark.
Statistical analysis
The data collected were analyzed using SPSS 13.0 software, and the results were expressed as mean±SD (\( \overline X \) ± S) values. Different groups were compared using t test, and all P values <0.05 were considered significant.
Results
Regarding the BMD data of 16,019 Han nationality individuals from Changchun, the peak bone mass in male and female population was detected in the age group of 30–39 years. BMD started to decrease with the advancing age. BMD of females aged over 50 years and males aged over 60 years was significantly lower (P < 0.01) compared with peak BMD. Of note, there was a significant difference (P < 0.01) of BMD between male and female individuals within the same age group. Regarding the BMD and OP morbidity data of 16,019 individuals tested in this study (Table 1), OP prevalence in the age group 20–44 years was 0, while the prevalence gradually increased in the age groups over 50 years. Moreover, OP prevalence of the females aged over 55 years was significantly higher (P < 0.01) than that of age-matched males. The BMD comparisons of Han nationality males from Changchun with Han males from Beijing, Dai males from Xishuangbanna, Tibetan males from Tibet, and Dongxiang males from Gansu are summarized in Table 2. Likewise, the BMD comparisons of Han nationality females from Changchun with the Han females from Beijing, Dai females from Xishuangbanna, Tibetan females from Tibet, and Dongxiang females from Gansu are summarized in Table 3. Furthermore, the BMD comparison of Han nationality males and females from Changchun with the age-matched male and female population from Japan is given in Table 4. Similarly, the BMD comparison of Han nationality males and females from Changchun with the age-matched male and female population from Denmark is shown in Tables 5. In addition, the comparisons of OP prevalence (percentage) between Changchun (Han) and Urumqi (gender-/age-matched, Han, and Uygur) populations are summarized in Tables 6. These data indicate that the OP prevalence in Changchun Han population was comparable to Urumqi (gender-/age-matched) Han population; however, OP prevalence of Changchun males in the age group 60–90 years was significantly lower than that of age-matched Urumqi males. The OP prevalence in Changchun Han females of the age group over 70 years was significantly higher than that of age-matched Uygur females from Urumqi.
Discussion
This study analyzed BMD profile of 16,019 males and females of Han nationality in Changchun region of China. The results show significant differences (P < 0.01) of BMD between different age groups, as well as between both genders within the same age group. In different age groups, the prevalence of osteoporosis was significantly higher in females than in males (P < 0.01). The peak BMD in this region was relatively higher than that reported in Japan and Denmark, and was comparable to that in Beijing. Moreover, the differences were significant (P < 0.01) as Han population of Changchun was compared with Dai population of Xishuangbanna, Tibetan population of Tibet, and Dongxiang population of Gansu.
Peak BMD value
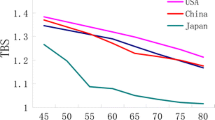
The peak BMD value (peak bone mass) affects the lifetime bone mineral contents, and hence, this study provides important reference data that may be used to evaluate the time of appearance and extent of bone loss. Our data show that in our study population, the peak bone mass of both males and females was observed at the age of 30–39 years; however, the peak bone mass of males was higher than that of females. These findings were in accordance with the previous studies from Urumqi, Beijing, Ningxia, and Nanning regions [1, 5–8]. The peak BMD value was higher than that of Dai individuals in Xishuangbanna and Tibetan individuals in Tibet but was lower than that of Dongxiang individuals in Gansu [2, 9]. Comparing with other studies that used the same type of measuring instruments as we did, the age of males in Changchun at which they attained the peak bone mass was the same as that of males in Japan and Denmark. However, the females in Changchun attained the peak bone mass at an earlier age as compared with females in Japan and Denmark [3, 4]. Statistical analysis revealed that peak bone mass of males and females in Changchun was higher than those of counterpart populations from Japan and Denmark.
Peak BMD value is the largest BMD value in the lifetime and the gross value of bone tissue that the human could reach at the mature age in life. It was reported [10] that 60–90% of bone mass changes correlated with genetic factors, whereas life environment, physical activity, nutrition, age, and gender were also the important factors that affected bone mass. After comparison with other studies using the same type of instruments, in China and abroad, our data showed that BMD had racial and regional differences. Therefore, our results point to the significance of establishing a Chinese population-based database of BMD based on different nationalities, regions, and age groups, including the measurements obtained by using different instruments in order for early-stage prevention, diagnosis, and treatment of OP.
Gender-based difference of bone mass changes
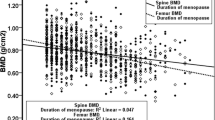
In Changchun, BMD of females aged over 40 years started to decline slowly, and the rate of bone loss increased each year after menopause. All the menopausal females in this study had natural menopause, and the mean menopausal age was 53.173 ± 2.591 years. The longest menopausal duration was 41 years and the shortest was 1 year. The bone loss rate of 0–5 year after menopause was 7.58%, BMD declined significantly with the extension of menopausal duration, and there were significant differences of BMD among the age groups of 65–89 years (P < 0.01). The rate of bone loss reached 11.5% in 10 years after menopause and 33.42% in 20 years after menopause, while the bone mass was 1/3 of the peak bone mass. Menopause is also an important risk factor for bone loss of females in Changchun. The females suffer from ovarian hypofunction after menopause during which estrogen level declines and the activity of osteoclasts increases. Thus, the bone loss is accelerated and, as a result, bone mass declines. BMD of males declined slowly after the age of 60 years, and then, the bone loss rate increased gradually with the advancing age; the bone loss rate was 15.66% at the age of 70 years, 19.96% at 75 years, 22.78% at 80 years, and 32.93% at 85 years. The rate of bone loss in females was significantly higher than in males, and there was a significant difference of the rate of bone loss between males and females (P < 0.01).
OP incidence
According to WHO diagnostic criteria for primary OP, it is diagnosed as OP if the BMD is lower than two standard deviations of BMD peak value OP [11]. Among the 16,019 individuals tested in this study, OP prevalence was 0 in the age group of 20–39 years. In females, the OP prevalence increased progressively after the age of 50 years, and significant differences (P < 0.01) were found among the age groups of 50–89 years. The female OP prevalence for each age group was significantly higher (P < 0.01) than that for males. The male OP prevalence increased after the age of 70 years, and there were significant differences (P < 0.01) between each age group. Compared with OP prevalence reported by other studies, OP prevalence for each age group in Changchun males was comparable to that of Han nationality males in Urumqi; however, OP incidence of the age groups of 60–90 years in Changchun was significantly lower than that of Uygur nationality males in Urumqi. The female OP prevalence after 70 years of age in Changchun was significantly lower than that of Uygur nationality females in Urumqi. The female OP incidence of the age groups of 50–79 years in Changchun was significantly lower than that in Japan [12]. Of note, there were differences regarding BMD and OP prevalence among individuals with same age and gender but having different race and geographical region.
Conclusions
In conclusion, BMD evaluation of 16,019 Han nationality individuals from Changchun region provides the reference data for the local peak BMD value and OP diagnosis which can be helpful as the basis for an early diagnosis and prevention of OP among individuals of both genders and different age groups. Our future studies will include the BMD evaluation across more diverse ethnic groups, such as Manchu, Korean, and Mongolian individuals, as well as establishment of multiethnic BMD database, and also investigate the factors that affect BMD at different levels.
References
Hao Z, Wangping Y, Qing G (2006) Study of normal range of BMD for peoples of Han and Uygur nationalities in Urumqi. Chinese J Osteoporosis 12:579–581
Wenli Z, Tuxing L, Yiping Y, Xianzhi C (2005) Normal values of bone mineral density measured with pDEXA in people of Guangdong in China. Chinese J Osteoporosis 11:64–67
Nakamura K, Tanaka Y, Saitou K, Nashimoto M, Yamamoto M (2000) Age and sex differences in the bone mineral density of the distal forearm based on health check up data of 6343 Japanese. Osteoporosis Int 11:772–777
Warming L, Hassager C, Christiansen C (2002) Changes in bone mineral density with age in men and women: a longitudinal study. Osteoporosis Int 13:105–112
Zhenfu Q, Hongbing Y, Xinghong W, Sanbao L, Aiguo S, Zhonghou L (2007) Study on the bone mineral pattern changes in phalangeal bones among the normal population in Miyun, Beijing. Chinese J Osteoporosis 13:648–650
Xiaomin W, Zhili Z, Jun L, Jiuyue Z, Qing X, Liu Z (2008) The study on bone mineral density of people in Beijing, Shenzhen and Tibet. Chinese J Osteoporosis 11:295–297
Zongjun M, Yinong W, Ning M, Lijun C, Xiaofang M, Lei D (2008) Investigation of bone mass density and prevalence rate of osteoporosis in healthy Hui people in Ningxia Province. Chinese J Osteoporosis 14:254–257
Xiaodong Y, Feng W, Zhong H, Minjia Z, Youhua C (2003) Investigation of bone mass density and prevalence rate of osteoporosis in healthy Han and Zhuang people in Nanning region. Chinese J Osteoporosis 9:268–270
Guoyi G, Fanbo J, Pinghua L, Zhiqiang M, Dongying W, Ling Y (2008) Investigation on bone mineral density in healthy Dai and Han nationalities in XiShuangBanNa. Chinese J Osteoporosis 14:266–269
Landin WK, Wihelmsen L, Bengtsson BA (1995) Postmenopausal osteoporosis is more related to hormonal aberrations than to lifestyle factors. Clin Endocrinol Oxf 51:387–394
Yan X (1999) Diagnosis and therapy of osteoporosis, 1st edn. Science Press, Beijing, pp 41–47
Iki M, Kagamimori S, Kagawa Y, Matsuzaki T, Yoneshima H, Marumo F (2001) Bone mineral density of the spine, hip and distal forearm in representative samples of the Japanese female population: Japanese Population-Based Osteoporosis (JPOS) Study. Osteoporosis Int 12:529–537
Acknowledgments
This study was supported by the Ministry of Civil Affairs (grant ref. Minrenkejiao–2007–18–1). We thank Gao Yuan, Ma Qianqian, and Mao Weixian for kind help with epidemiological investigation.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mengmeng, Z., Yagang, L., Ying, L. et al. A study of bone mineral density and prevalence of osteoporosis in Chinese people of Han nationality from Changchun. Arch Osteoporos 7, 31–36 (2012). https://doi.org/10.1007/s11657-011-0066-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11657-011-0066-8