
Abstract
In this report, we present the derivation and characterization of 15 hESC lines established at the Vrije Universiteit Brussel, Belgium in collaboration with the Universitair Ziekenhuis Brussel, Belgium, using surplus in vitro fertilization embryos and embryos carrying monogenic disorders donated for research. Four lines were derived from blastocyst-stage embryos presumed to be genetically normal, and 11 hESC lines were obtained from embryos shown to carry genetic mutations by preimplantation genetic diagnosis. All the lines express markers of pluripotency as determined by immunocytochemistry and RT-PCR, and formed teratomas when injected into SCID mice. All VUB hESC lines, except for VUB17, are reported in the European hESC registry and are available upon request after signing a Material Transfer Agreement from the VUB (contact person: Prof. Dr. Karen Sermon; Karen.Sermon@uzbrussel.be).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Centre for Reproductive Medicine (CRG) in cooperation with the Centre for Medical Genetics (CMG) from the Universitair Ziekenhuis Brussel (UZ Brussel, Belgium) is offering assisted reproduction techniques for patients with infertility problems and/or for couples at risk of transmitting genetic diseases. Following in vitro fertilization (IVF), embryos at the blastocyst stage are transferred to the mother to achieve a pregnancy. The surplus embryos are cryopreserved, destroyed, or donated for research. For the couples at risk of transmitting genetic diseases, preimplantation genetic diagnosis (PGD) allows for the detection of a genetic defect in preimplantation embryos prior to their transfer in utero. PGD is performed by fluorescent in situ hybridization for the diagnosis of aneuploidies or X-linked pathologies, and by PCR for the diagnosis of single gene disorders (Sermon et al. 2004; Spits and Sermon 2009). PGD embryos diagnosed as free of the disease under consideration (or unaffected) are either transferred to the mother or cryopreserved if there are supernumerary good quality embryos. PGD embryos diagnosed as being affected are either discarded or donated for research. As a consequence, surplus normal embryos and embryos carrying genetic disorders are available in our center for the derivation of hES cell lines. In addition, blastomeres obtained from oocytes donated for research investigating the plasticity/totipotency state of the four-cell stage human embryo were also available for derivation of hESC lines (Geens et al. 2009).
We have previously reported the derivation of five hESC lines from which two lines were presumed to be genetically normal (VUB01 and VUB02) and three lines that carried mutations for myotonic dystrophy type 1 (VUB03_DM1), cystic fibrosis (VUB04_CF), and Huntington’s disease (VUB05_HD) (Mateizel et al. 2006). More recently, our group reported the derivation of two hESC lines (VUB26_QUATRO and VUB27_PATRU) from single blastomeres of four-cell stage embryos (Geens et al. 2009).
Here we present the isolation and characterization of 15 new hESC lines derived at the Vrije Universiteit Brussel (VUB) in collaboration with the CRG and CMG of UZ Brussel: Four lines were derived from presumed genetically normal blastocyst-stage embryos from regular IVF cycles, and 11 hESC lines were derived from affected embryos, therefore carrying known genetic defects like myotonic dystrophy type 1 (DM1), fragile X syndrome (FXS), spinocerebellar ataxia type 7 (SCA7), Marfan syndrome (MFS), fascioscapulohumeral muscular dystrophy (FSHD), Charcot-Marie Tooth type 1A (CMT1A), cystic fibrosis (CF), and osteogenesis imperfecta (OI). One hESC line was derived from an embryo affected with both Huntington’s disease and Marfan syndrome.
Materials and Methods
Embryo regulations.
All human embryos used in the present report were donated for research after the informed consent of the couple and the approval of the ethical committee at the UZ Brussel and of the Federal Commission for Medical and Scientific Research on Embryos in vitro that represents the competent authority in Belgium. All the donors are traceable and, as a part of IVF/PGD procedure, were screened for the presence of viral and/or microbiological contamination.
Source of embryos.
Spare fresh human embryos from IVF/intracytoplasmic sperm injection cycles (ICSI) cycles whose morphology did not fulfill the requirements for transfer or freezing were used at day 6 for the derivation of the hESC lines. The embryos diagnosed after PGD as carrying genetic mutations were used for the derivation of the affected lines. All the embryos were cultured in the sequential M1 (EmbryoAssist) and M2 (BlastAssist) medium (Medicult, www.medicult.com; Jyllinge, Denmark). The evaluation of embryo quality during in vitro development is presented in Table 1.
PGD procedure.
During this procedure, a blastomere is removed from the embryo at day 3 post-ICSI and used for the diagnosis of a known genetic disease, while the rest of the embryo is maintained in culture. The biopsied blastomeres were analyzed by simplex, multiplex, or triplet-primed PCR (TP-PCR), according to the mutations for which they were tested (Sermon et al. 2004; Spits and Sermon 2009). A description of the tests performed on embryos during PGD is presented in the “Results” section. A detailed protocol for each PGD procedure is available upon request, as not all protocols have been previously published.
Derivation of hESC lines.
The general procedure for the derivation of hESC lines applied in our center involved isolation of the inner cell mass (ICM) from the surrounding trophectoderm of day 6 blastocysts either by immunosurgery as previously reported (Reubinoff et al. 2000; Mateizel et al. 2006) or by a mechanical approach using a glass needle made from a finely drawn Pasteur pipette. The isolated ICMs were plated on inactivated CF1 mice embryonic fibroblasts (MEFs; 2–4 × 104 cells/cm2; Millipore, http://www.millipore.com, Billerica, MA) and cultured further at 37°C in 10% C02 in hESC medium consisting of knockout D-MEM (Invitrogen; http://www.invitrogen.com; Carlsbad, CA) supplemented with 20% (Invitrogen), 2 mM l-glutamin (Invitrogen), 1% non-essential amino acids (Invitrogen), 0.1 mM β mercapto-ethanol (Sigma Aldrich, St. Louis, MO), and 4 ng/ml human recombinant basic fibroblast growth factor (Invitrogen). Several days after the initial plating, when the outgrowths showed cells of stem cell-like morphology, a mechanical dissociation was performed. The clumps of cells were plated on new feeder layers, and the resulting colonies were passaged further by mechanical slicing.
Cryopreservation of the cells was successfully performed using a modified version (Mateizel et al. 2006) of the “vitrification in open pulled straws” protocol (Reubinoff et al. 2001).
Characterization of hESC lines.
Our previous publication (Mateizel et al. 2006) described the procedures used to characterize the first five hESC lines derived in our centers. The same characterization was performed for all the hESC lines derived further in our laboratory. The cell surface markers were analyzed by immunostaining. Cells were initially incubated over night at 4°C with the primary antibody: rat anti-SSEA-3 (IgM; MAB4303, Millipore, 1:100), mouse anti-TRA-1-60 (IgM; MAB4360, Millipore, 1:100), mouse anti-TRA-1-81 (IgM; MAB4381, Millipore, 1:100), and mouse anti-SSEA-4 (IgG, MAB4304, Millipore, 1:100); followed by the second incubation with the secondary antibodies for 2 h at room temperature: Alexa fluor 488-conjugated F(ab0)2 fragments of goat anti-mouse immunoglobulins IgM or IgG (Invitrogen, 1:250). Controls for antibody specificity included substitution with mouse IgM (Caltag, Carlsbad, CA; 1:10) or IgG (Zymed, San Francisco, CA; 1:250), respectively. Confocal scanning microscopy with an argon–krypton laser (488/568) (Fluoview IX70; Olympus, Aartselaar, Belgium) was used to record the fluorescent images.
For the gene expression studies of the markers POU5F1, NANOG, DNMT3B, GDF3, LIN 28, NPM 1, REX-1, and SOX-2, the RNA was isolated using the RNeasy Mini Kit (Qiagen, Hilden, Germany) and was reverse-transcribed to cDNA using the First-strand cDNA Synthesis Kit (GE Healthcare, Diegem, Belgium) with the NotI-d(T) primer. The primer sequences and conditions of the PCRs (35 cycles) are described in Table 2. PCR products were analyzed on a 2% agarose gel.
Alkaline phosphatase activity was detected using the Vector Blue substrate kit (Vector Laboratories, Burlingame, CA). For the in vivo test of pluripotency, small clumps of cells were injected into the rear leg muscle of a SCID mouse, and the obtained teratomas were analyzed by hematoxylin–eosin staining at the Anatomo-Pathology Department of the UZ Brussel for the presence of derivatives of the three cell lineages.
Initially, G-banding was used to karyotype the established hESC lines (Gosden et al. 1992). More recently, array-based comparative genomic hybridization (aCGH), which allows a higher resolution analysis, was performed on all hESC lines derived in our laboratory. This procedure has been described in detail by Spits et al. (2008). Briefly, aCGH was performed using in-house arrays from the Microarray facility, VIB, K.U. Leuven (www.microarrays.be, Leuven, Belgium). Genomic DNA was extracted from peripheral blood from male and female controls and used as references. Three-hundred-nanogram test and reference DNA samples were labeled for at least 2 h by random primer labeling (BioPrime Array CGH Genomic Labelling System; Invitrogen) using Cy5- and Cy3- labeled dCTPs (GE Healthcare). One thousand seven hundred and fifty nanogram of each labeled DNA was hybridized in a humid chamber (37°C for 24 to 72 h) on a slide blocked with Cot-1 and salmon testes DNA (Sigma Aldrich). The arrays were scanned using an Agilent dual laser DNA microarray scanner G2566AA (Agilent Technologies, Palo Alto, CA). The scan images were processed with Agilent Feature Extraction Software v9.5, and the final steps of data analysis were performed using Excel (Microsoft Corporation, Redmond, WA).
Genetic testing of the hESC lines carrying a monogenic disease.
All hESC lines assumed to carry a genetic disorder were tested to ensure their carrier status. For the lines VUB08_MFS, VUB09_FSHD, VUB10_SCA7, VUB20_CMT1A, VUB22_CF, and VUB23_OI, a similar PCR protocol was used to confirm the presence of the respective mutations as was applied during the PGD procedure. For the rest of the lines (VUB11_FXS, VUB13_FXS, VUB19_DM1, VUB24_DM1, and VUB28_HD_MFS), direct testing of the mutation was used. The loci tested for each line are described in the “Results” section, along with the exact mutation and its origin (paternal and/or maternal). The primer sequences for all loci, along with the PCR conditions, can be found in the “Electronic Supplementary Materials”.
Statistical analysis.
The statistical analysis was performed using MedCalc software (Belgium). The test was performed at the 5% level of significance. The χ 2 test was used to analyze the difference between the immunosurgery and mechanical approach in the derivation rate of hESC lines.
Results
Source of embryos and derivation of hESC lines.
Three hundred fifty-two embryos from IVF/ICSI and PGD cycles were used for the derivation of hESC lines, from which 46 embryos were spare normal embryos from IVF/ICSI cycles, and 306 embryos were affected embryos from PGD cycles. Four hESC lines (8.6%) were isolated from normal embryos (VUB06, VUB07, VUB014, and VUB17) and 11 hESC lines (3.6%) from the PGD embryos. From this last group, five hESC lines were derived from embryos affected by trinucleotide repeat disorders: myotonic dystrophy type 1 (VUB19_DM1 and VUB24_DM1), fragile X syndrome (VUB11_FXS and VUB13_FXS), and spinocerebellar ataxia type 7 (VUB10_SCA7); one hESC line was derived from an embryo affected with both Huntington’s disease and Marfan syndrome (VUB28_HD_MFS); five other hESC lines were derived from embryos diagnosed as carrying Marfan syndrome (VUB08_MFS), fascioscapulohumeral muscular dystrophy (VUB09_FSHD), Charcot-Marie Tooth type 1A (VUB20_CMT1A), cystic Fibrosis (VUB22_CF), and osteogenesis imperfecta (VUB23_OI).
Nine out of 15 hESC lines were derived using immunosurgery as a method for isolation of the ICM, and six hESC were derived by a mechanical approach, giving a success rate of 4.6% (nine lines out of 192 embryos) and 3.75% (six lines out of 160 embryos), respectively. All the lines are presented in Table 1 along with the evaluation from days 1 to 5 of the original embryo.
Characterization of the hESC lines.
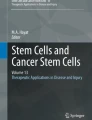
Morphological analysis of the human embryonic stem cells revealed the characteristic features of hESC (Thomson et al. 1998; Reubinoff et al. 2000): compact colony structure, high ratio of nucleus to cytoplasm, and prominent nucleoli (Fig. 1 A). The cell surface markers (SSEA-3, SSEA-4, TRA-1-60, and TRA-1-81) were expressed in all hESC lines, as determined by immunocytochemistry. Similarly, RT-PCR confirmed the expression at the mRNA level of several genes characteristic of undifferentiated hESC (POU5F1, SOX2, REX1, NANOG, GDF3, DNMT3B, LIN28, and NPM1) in all the lines. In addition, each line was found to present high levels of alkaline phosphatase activity. As all the lines gave comparable results, consistent with an undifferentiated ES cell phenotype, we have presented in Fig. 1, as an example, the results for line VUB11_FXS. When transplanted into SCID mice, all the hESC produced teratomas containing derivatives all of the three germ layers (endoderm, ectoderm, and mesoderm), confirming the pluripotent capacity of all the newly derived hESC lines. A teratoma derived from the line VUB11_FXS is shown in Fig. 1 J by way of example. The teratoma derived from VUB17 was not yet analyzed, the reason why it was not registered in the European hESC registry.

Characterization of VUB11-FXS line. (A) Phase contrast image of hESC colonies grown on mice embryonic fibroblasts. (B) Detection of ALP activity. (C) RT-PCR analysis of gene expression in predominantly undifferentiated hESC colonies. (D–I) Immunochemistry analysis of VUB11_FXS. (D, E) Confocal microscopy images showing IgG and IgM staining, respectively (negative control); the left panels represent the immunostaining for the isotype controls, and the right panels represent the corresponding differential interference contrast image of the colonies. (F–I) Confocal images showing expression of SSEA-3, SSEA-4, TRA-1–60, and TRA-1–81 on hESC colonies. (J) Hematoxylin–eosin staining on teratoma showing differentiation into cartilage, gastrointestinal tract, and squamous epithelium. (K) Result of the array CGH at passage 10 showing a 46,XX karyotype.
The aCGH and G-banding results showed a normal 46,XX karyotype at the first passage tested for all lines. However, chromosomal abnormalities were observed in some lines after as few as 21 passages in culture. VUB06 and VUB08_MFS presented a trisomy 17 and 22, respectively. A subline of VUB07 first acquired a duplication at 20q11.21 and later at 3q26.33q27.2 (containing the SOX2 gene). One subline of VUB09_FSHD acquired a duplication of the c-MYC gene, at 8q24.21; a second subline presented first a duplication 11q24.2q25 and later also the duplication 20q11.21. VUB13_FXS evolved from a normal karyotype to a monosomy X, combined with the appearance of a derivative chromosome 18 (dup(5)(q21.3qter)), del(18)(q12.1qter). These results have been previously published and discussed in depth by Spits et al. (2008). The normal 46,XX chromosomal constitution of the line VUB11_FXS obtained after aCGH is presented as an example in Fig. 1 K.
Genetic testing of the hESC lines carrying a monogenic disease.
Genetic testing of the hESC lines with the parents’ DNA as positive control was undertaken to ascertain whether the expected mutations were present in the hESC lines. The results are presented below and in Fig. 2 that illustrates the different methods that have been used: Fig. 2 A shows the results of the TP-PCR for VUB10_SCA7, Fig. 2 B shows a Southern blot result after small-pool PCR of VUB19_DM1, Fig. 2 C shows the genetic testing of VUB22_CF by fragment analysis after multiplex PCR, and Fig. 2 D shows the results of the minisequencing analysis and fragment analysis performed on VUB28_HD_MFS. The results proved that all lines carried the expected mutations.

Genetic testing of hESC lines. A, C, and D show the analysis results on an ABI Prism 3130 Avant 400 Genetic Analyzer. In all cases, the X axis represents fragment size and the Y axis peak signal intensity. A- Genetic testing of VUB10_SCA7. Fragment analysis on after TP-PCR for the direct screening of CAG triplet repeat expansion. All alleles are marked with arrows and with their size in repeats. The genomic DNA of the donors of the embryo shows two wild-type alleles (10 and 12 repeats) and a wild-type allele of 10 repeats and an expanded allele of 37 repeats. The results from VUB10_SCA7 show a wild-type allele of 10 repeats and an expanded allele of 37 repeats. B- Southern blot of the PCR products for the genetic testing of VUB19_DM1. (a) Genomic DNA from VUB19_DM1 at passage 1 showing the wild-type allele and an expansion of 250 repeats (arrow); (b) genomic DNA from the unaffected partner of the couple donating the embryo (only wild-type signal); (c) genomic DNA from the affected partner (wild-type allele and expansions of 135, 409 180, 240, 260, 300, and 550 repeats). C- Genetic testing of VUB22_CF. Fragment analysis after multiplex PCR for the mutation c.1522_1524del (p.F508del) and the microsatellite markers IVS17BTA, IVS8CA, D7S633, D7S677, and CFTRSTR30AC. Both donors are carriers, while the VUB22_CF is homozygous for the p.F508del mutation. The alleles for the p.F508del mutation are marked with arrows. D- Genetic testing of VUB28_HD_MFS. Results of the minisequencing analysis of the c.7828G>A mutation in FBN1 (a–c) and of the fragment analysis of the Huntington triplet repeat mutation (d). (a) Genomic DNA of the unaffected female donor, showing a G/G genotype; (b) genomic DNA of the affected male donor, showing a G/A genotype; and (c) genomic DNA of the affected VUB28_HD_MFS line, also showing a G/A genotype; (d) the unaffected allele (23 repeats) and the expanded allele (40 repeats) of the Huntington’s gene in the VUB28_HD_MFS line. Both alleles are marked with arrows.
MFS (OMIM 154700) is an autosomal dominant disorder of the fibrous connective tissue caused by mutations in the fibrillin-1 (FBN1) gene. VUB08_MFS carried the c.266G>T mutation in exon 3, inherited from the husband from the couple that donated the embryo. During PGD, a multiplex PCR for the five polymorfic markers D15S1028, D15S992, D15S196, D15S576, and D15S143 was used, which was shown to be informative after linkage analysis of family members. This same protocol was later applied for the testing of the line, which revealed that it carried the haplotype linked to the mutation, and therefore can be considered as carrier of the disease.
FSHD (OMIM 158900) is an autosomal dominant disorder caused by a chromosomal rearrangement within the D4Z4 subtelomeric region of 4q35. The female partner of the couple donating the embryo used for the derivation of VUB09_FSHD carried a pathogenic deletion in the D4Z4 locus. This deletion was detected during PGD, and later in the VUB09_FSHD line by triplex PCR for three markers linked to D4Z4 locus (D4S1523, D4S2930, and D4S2299).
FXS (OMIM 300624) is an X-linked disease caused by mutation in the FMR1 gene, the vast majority of cases being caused by a trinucleotide (CGG)n expansion in the 5′ region of the FMR1 gene greater than 200 repeats. The embryos used for the derivation of VUB11_FXS and VUB13_FXS came from the same PGD cycle, making the two lines genetically related. The embryos used to derive VUB11_FXS and VUB13_FXS were diagnosed as female carriers using a PCR amplifying the wild-type allele, and conventional Southern blotting on DNA from the hESC lines revealed that VUB11_FXS was a mosaic for two fully methylated expansions of approximately 2,000 and 2,100 CGGs, and VUB13_FXS carried a fully methylated expansion of 2,000 CGGs.
SCA7 (OMIM 164500) is a progressive autosomal dominant neurodegenerative disorder caused by an expansion of over 36 repeats for the trinucleotides CAG in the ATXN-7 gene. Both the embryo used for the derivation of VUB10_SCA7, as the line itself, were diagnosed using TP-PCR for the direct screening of CAG triplet repeat expansion. The result showed that the hESC carries the mutation (37 CAG repeats), inherited from the husband from the couple donating the embryo (Fig. 2 A).
DM1 (OMIM 160900) is an autosomal dominant neurodegenerative disorder caused by the expansion of a CTG repeat to more than 50 repeats in the 3′ untranslated region of the dystrophia myotonica protein kinase gene (DMPK). During two different PGD cycles, the embryos used for the derivation of VUB19_DM1 and VUB24_DM1 were diagnosed by TP-PCR. In the case of VUB19_DM1, the line was derived from an embryo carrying a paternally inherited expansion (160 CTG repeats in the donor). For VUB24_DM1, the expansion was maternally inherited, and of unknown size in the donor. Both hESC lines were tested by small-pool PCR followed by Southern blot (De Temmerman et al. 2008). VUB19_DM1 presented an expansion of 250 repeats at passage 1 (Fig. 2 B) and VUB24_DM1 an expansion of 1,800 repeats at passage 5. This expansion proved unstable and steadily increased in size over time in culture (Seriola et al. 2008 and manuscript in preparation).
CMT1A (OMIM 118220) is an autosomal dominant disease resulting from a duplication of the PMP-22 (peripheral myelin protein-22) gene, a critical component of the myelin sheath. We used the same protocol to test VUB20_CMT1A as was applied for the PGD, a multiplex PCR for three markers in the duplication of the PMP-22 gene: D17S2220, D17S2227, and D17S2230. The mutation was transmitted by the male partner of the donor couple. The results showed that the hESC carries the PMP-22 duplication.
CF (OMIM 219700) is an autosomal recessive disease caused by mutations in the coding region of the cystic fibrosis transmembrane conductance regulator gene (CFTR). Both partners of the couple who donated the embryo for the derivation of VUB22_CF were carriers of the c.1522_1524del (p.F508del) mutation. During PGD, a multiplex PCR for the mutation c.1522_1524del and the microsatellite markers IVS17BTA, IVS8CA, D7S633, D7S677, and CFTRSTR30AC was used. This same test was performed on the established hESC line, proving that it is homozygous for the mutation (Fig. 2 C).
OI type 1 (OMIM 166200) is an autosomal dominant disease caused by mutation in the COL1A1 gene, leading to reduced amounts of normal collagen type I. The embryo for the derivation of VUB23_OI and later the hESC line itself were tested by linkage analysis and indirect diagnosis using a multiplex PCR for five markers (D17S1319, D17S588, D17S19GT, D17S16AC, and D17S1869) in the region of the COL1A1 gene. The results revealed that VUB23_OI carries the c.769G>A mutation, transmitted by the female partner of the couple donating the embryo.
HD (OMIM 143100) is an autosomal dominant neurodegenerative disease associated with increases of over 35 repeats in a CAG triplet repeat in the huntingtin gene. The embryo for the derivation of VUB28_HD_MFS was diagnosed using a complex PGD protocol involving whole genome amplification and PCRs specific for the HD and FBN1 (MFS) region (the details of this procedure are available upon request). Both disorders were transmitted by the male partner of the couple donating the embryo. For the genetic testing of VUB28_HD_MFS, we performed a direct testing by minisequencing for the FBN1 c.7828G>A mutation and size determination of the CAG repeat for HD. The results confirmed the PGD results, and the line carries both disorders (Fig. 2 D).
Discussion
After more than 10 years since the derivation of the first hESC line (Thomson et al. 1998), around 600 lines are now registered at the European hESC registry, a significant part of which carry a monogenic disorder. This is a consequence of the existence of centers such as our own that are linked to an IVF center with a very active PGD program.
We report here the derivation of presumably genetically normal hESC lines and of hESC lines carrying mutations for monogenic diseases using either immunosurgery or a mechanical approach as means for the isolation of the ICMs. We showed that hESC lines could also be isolated from low quality embryos with an abnormal developmental pattern. No significant statistical difference (p = 0.86) in the derivation rate between the immunosurgical and mechanical approach for ICM isolation was observed.
While derivation of hESC lines from unaffected embryos has a potential use in clinical application for regenerative medicine, hESC lines carrying mutations for monogenic diseases mainly have potential applications in disease modeling and drug screening. As these cells can differentiate to all the different cell types present in an adult individual, they could be used as a constant source of those cell types affected by the studied disease. This is of particular interest in disorders such as for instance DM1, for which the existing mouse models do not fully represent the human pathogenesis (for instance the Dmpk knockout mouse; Reddy et al. 1996), and for which the culture of the relevant cell types is difficult. An example of this is our current work on the generation of epithelial–lung cells from CF affected hESC lines. CF is considered the most common severe autosomal recessive disease in Caucasian populations, and one of the organs primarily affected by the disease is the lung. The main objective of this project is to create a valid in vitro model for the pathogenesis of CF. In this regard, besides the already reported hESC line (VUB04_CF) carrying the p.F508del mutation in the CFTR gene (Mateizel et al. 2006), we present here the derivation of a new hESC line (VUB22_CF), homozygous for the same mutation. This provides the possibility to investigate the different impacts on a given tissue (f.i. the lung epithelium) and the fact of its being homo- or heterozygous for a CF mutation.
Furthermore, hESC has been suggested as a unique model for early human development, and lines carrying trinucleotide repeat mutations may prove very useful for the understanding of the genetic mechanisms of repeat instability during the embryonic stage, and possibly gametogenesis. Indeed, taking into account that 42% of the PGD cycles in our center are triplet nucleotide repeat disorders, one interest of our laboratory was the derivation of hESC lines affected with these mutations as a main source of cells for characterizing the mechanisms of repeats instability. We have previously reported the derivation and characterization of VUB03_DM1 and VUB05_HD (Mateizel et al. 2006), and here, we present the derivation of six additional hESC carrying mutations for triplet nucleotide repeats disorders: VUB19_DM1, VUB24_DM1, VUB11_FXS, VUB13_FXS, VUB10_SCA7, and VUB28_HD_MFS. These lines present mutations inherited through both the maternal and paternal lineages, which for these diseases make a crucial difference in the triplet repeat behavior (Pearson et al. 2005). Several projects on the mechanisms of repeat instability, based on analysis of these lines, are ongoing in our laboratory and in collaboration with other research groups (De Temmerman et al. 2008; Seriola et al. 2008).
The derivation of the VUB09_FSHD, to our knowledge, the first hESC line affected with FSHD mutation, will help to elucidate the complexities of the subtelomeric 4q35 locus characterized by high recombination and therefore the study of the underlying mechanisms of the disease. In addition, derivation of the lines VUB08_MFS, VUB20_CMT1A, and VUB23_OI can provide models for those groups working on these diseases.
Another interesting aspect of hESC is their similitude to cancer cells, particularly concerning their genomic instability. We have found several recurrent chromosomal abnormalities that had not been previously reported (Spits et al. 2008). Although this fact may, at first sight, hamper the clinical use of these cells, intensive research on the mechanisms of origin and the biological significance of these abnormalities may, on one hand, allow us to avoid their appearance in culture and, on the other hand, gain very interesting insights in the in vivo carcinogenic processes.
Currently, an upcoming alternative source of pluripotent immortal cells carrying various mutations is represented by the induced Pluripotent Stem (iPS) cells. The possibility of deriving iPS from virtually any cell type allows for the derivation of disease specific lines, using cells from patients affected by genetic diseases with either Mendelian or complex inheritance (Park et al. 2008). Although relatively simple to achieve, questions remain whether the insertion of genes necessary for inducing pluripotency affects the functionality of iPS cell-derived differentiated cells (Liu 2008; Abeliovich and Doege 2009). Therefore, considering the inherent genetic variability between hESC and iPS cell lines, derivation of more pluripotent cell lines (hESC and iPS) with or without genetic diseases will allow a better comparison among them and consequently a better chance for choosing the appropriate source for therapy or for disease modeling.
References
Abeliovich; Doege. Reprogramming therapeutics: iPS cell prospects for neurodegenerative disease. Neuron 61(3): 337–339; 2009.
De Temmerman N.; Seneca S.; Van Steirteghem A.; Haentjens P.; Van der Elst J.; Liebaers I.; Sermon K. D. CTG repeat instability in a human embryonic stem cell line carrying the myotonic dystrophy type 1 mutation. Mol. Hum. Reprod. 14(7): 405–412; 2008.
Gardner D. K.; Schoolcraft W. B. In-vitro culture of human blastocysts. In: Jansen R.; Mortimer D. (eds) Towards Reproductive certainty: fertility and genetics beyond 1999. Parthenon, Carnforth, pp 378–388; 1999.
Geens M.; Mateizel I.; Sermon K.; De Rycke M.; Spits C.; Cauffman G.; Devroey P.; Tournaye H.; Liebaers I.; Van de Velde H. Human embryonic stem cell lines derived from single blastomeres of two 4-cell stage embryos. Hum Reprod. 24: 2709–2717; 2009.
Gosden C.; Davdson C.; Robertson M. Lymphocyte culture. In: Rooney D. E.; Czepulkowsky B. H. (eds) Human cytogenetics. Oxford University Press, Oxford, pp 37–47; 1992.
Liu S. V. iPS cells: a more critical review. Stem Cells Dev 17(3): 391–397; 2008.
Mateizel I.; De Temmerman N.; Ullmann U.; Cauffman G.; Sermon K.; Van de Velde H.; De Rycke M.; Degreef E.; Devroey P.; Liebaers I.; Van Steirteghem A. Derivation of human embryonic stem cell lines from embryos obtained after IVF and after PGD for monogenic disorders. Hum. Reprod. 21(2): 503–511; 2006.
Park I. H.; Arora N.; Huo H.; Maherali N.; Ahfeldt T.; Shimamura A.; Lensch M. W.; Cowan C.; Hochedlinger K.; Daley G. Q. Disease-specific induced pluripotent stem cells. Cell 134(5): 877–886; 2008.
Pearson C. E.; Nichol Edamura K.; Cleary J. D. Repeat instability: mechanisms of dynamic mutations. Nat. Rev. Genet. 6: 729–742; 2005.
Reddy S.; Smith D. B.; Rich M. M.; Leferovich J. M.; Reilly P.; Davis B. M.; Tran K.; Rayburn H.; Bronson R.; Cros D.; Balice-Gordon R. J.; Housman D. Mice lacking the myotonic dystrophy protein kinase develop a late onset progressive myopathy. Nat. Genet. 13: 325–335; 1996.
Reubinoff B. E.; Pera M. F.; Fong C. Y.; Trounson A.; Bongso A. Embryonic stem cell lines from human blastocysts: somatic differentiation in vitro. Nat. Biotechnol. 18: 399–404; 2000.
Reubinoff B. E.; Pera M.; Vajta G.; Trounson A. O. Effective cryopreservation of human embryonic stem cells by the open pulled straw vitrification method. Hum. Reprod. 16(10): 2187–2194; 2001.
Seriola A.; Spits C.; Mateizel I.; De Temmerman N.; Hilven P.; Van der Elst J.; Liebaers I.; Sermon K. Trinucleotide repeat instability in human embryonic stem cells: the role of the mismatch repair machinery. Hum. Reprod. 23(S1): i110; 2008.
Sermon K.; Van Steirteghem A.; Liebaers I. Preimplantation genetic diagnosis. Lancet 363: 1633–1641; 2004.
Spits C.; Mateizel I.; Geens M.; Mertzanidou A.; Staessen C.; Vandeskelde Y.; Van der Elst J.; Liebaers I.; Sermon K. Recurrent chromosomal abnormalities in human embryonic stem cells. Nat. Biotechnol. 26(12): 1361–1363; 2008.
Spits C.; Sermon K. PGD for monogenic disorders: aspects of molecular biology. Prenat. Diagn. 29(1): 50–56; 2009.
Thomson J.; Itskovitz-Eldor J.; Shapiro S.; Waknitz M.; Swiergiel J.; Marshall V.; Jones J. Embryonic stem cell lines derived from human blastocysts. Science. 282(5391): 1145–1147; 1998.
Acknowledgments
We gratefully acknowledge the assistance of Mieke Geens, Lindsey Van Haute, Bing Chen, and Anna Seriola Petit for maintaining the hESC lines in culture. The authors are also grateful to Debby Van Boxstael for performing part of the genetic analysis of the hESC lines. Ileana Mateizel is supported by the Research Council (OZR) of the Vrije Universiteit Brussel and the FWO (Fonds voor Wetenschappelijk Onderzoek, Vlaanderen, Fund for Scientific Research Flanders). Claudia Spits is a postdoctoral fellow of the FWO.
Author information
Authors and Affiliations
Corresponding author
Additional information
Editor: P. Andrews
Ileana Mateizel and Claudia Spits contributed equally to this work.
Electronic Supplementary Materials
ESM 1
(DOC 60 kb)
Rights and permissions
About this article
Cite this article
Mateizel, I., Spits, C., De Rycke, M. et al. Derivation, culture, and characterization of VUB hESC lines. In Vitro Cell.Dev.Biol.-Animal 46, 300–308 (2010). https://doi.org/10.1007/s11626-010-9284-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11626-010-9284-4