
ABSTRACT
BACKGROUND
Little is known about the healthcare experiences of adults on the autism spectrum. Moreover, autistic adults have rarely been included as partners in autism research.
OBJECTIVE
To compare the healthcare experiences of autistic and non-autistic adults via an online survey.
METHODS
We used a community-based participatory research (CBPR) approach to adapt survey instruments to be accessible to autistic adults and to conduct an online cross-sectional survey. We assessed preliminary psychometric data on the adapted scales. We used multivariate analyses to compare healthcare experiences of autistic and non-autistic participants.
RESULTS
Four hundred and thirty-seven participants completed the survey (209 autistic, 228 non-autistic). All adapted scales had good to excellent internal consistency reliability (alpha 0.82–0.92) and strong construct validity. In multivariate analyses, after adjustment for demographic characteristics, health insurance, and overall health status, autistic adults reported lower satisfaction with patient-provider communication (beta coefficient −1.9, CI −2.9 to −0.9), general healthcare self-efficacy (beta coefficient −11.9, CI −14.0 to −8.6), and chronic condition self-efficacy (beta coefficient −4.5, CI −7.5 to −1.6); higher odds of unmet healthcare needs related to physical health (OR 1.9 CI 1.1–3.4), mental health (OR 2.2, CI 1.3–3.7), and prescription medications (OR 2.8, CI 2.2–7.5); lower self-reported rates of tetanus vaccination (OR 0.5, CI 0.3–0.9) and Papanicolaou smears (OR 0.5, CI 0.2–0.9); and greater odds of using the emergency department (OR 2.1, CI 1.8–3.8).
CONCLUSION
A CBPR approach may facilitate the inclusion of people with disabilities in research by increasing researchers’ ability to create accessible data collection instruments. Autistic adults who use the Internet report experiencing significant healthcare disparities. Efforts are needed to improve the healthcare of autistic individuals, including individuals who may be potentially perceived as having fewer disability-related needs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Over $400 million is spent annually in the United States on autism research, the vast majority addressing autism prevalence, potential etiologies, early identification strategies, and possible treatments in children.1 However, very few studies have focused on the priorities of adults with autism (hereafter referred to as “autistic adults”2), including access to high quality healthcare.3
Prior studies have documented that people with disabilities face disparities in health and healthcare as compared to people without disabilities.4–20 Though some studies assessing healthcare disparities for adults with developmental disabilities have included participants on the autism spectrum, with the exception of one small study using administrative data,21 they do not report results separately for autistic participants. Most studies also primarily include participants with intellectual disabilities, and may not be generalizable to the full range of individuals now recognized as on the autism spectrum, a majority of whom do not have an intellectual disability.22–25
Autistic adults who use the Internet represent an understudied population of healthcare users who may experience important barriers to care, despite often being presumed to have fewer disability-related needs. The Internet has played a very important role in the Autistic community, partly because online communication can be more accessible to individuals who find in-person and telephone communication challenging.26–29 Though the rate of Internet use amongst autistic adults has not been studied, it is likely high, with an adage in the autistic community that “the Internet is to autistics as American Sign Language was to the Deaf.”30 Autistic adults have a wealth of information to offer about their experiences, but to our knowledge, no studies elicit information directly from adults on the autism spectrum about their satisfaction with healthcare. Moreover, autistic adults have rarely been included as partners in autism research.
We used a community-based participatory research (CBPR) approach to adapt previously validated health services questionnaires to more accurately assess the healthcare experiences of autistic adults and hypothesized that potential disparities may exist.
METHODS
This study was approved by the Institutional Review Board at Oregon Health and Sciences University.
Community-Based Participatory Research Approach
The Academic Autistic Spectrum Partnership In Research and Education (AASPIRE, www.aaspire.org) is a community-academic partnership that includes health services and disability researchers, autistic adults, family members, and disability services providers. We used a CBPR31,32 approach, whereby academic and community members served as equal partners throughout all phases of the research. A majority of study team members are on the autism spectrum. Community and academic partners worked collaboratively to choose the research questions, design study protocols, choose and adapt data collection instruments, recruit participants, interpret results, and coauthor this manuscript. Further details of our collaboration process are described elsewhere.33
Setting and Participants
We conducted this study using the Gateway Project (www.thegatewayproject.org), a secure registration system for online studies. We recruited a convenience sample of adults, age 18 or older, who have access to the Internet, by messages posted to listserves, blogs, and websites targeting autistic adults, adults with other disabilities, the broader autism and disability communities, and general Internet users. We also actively recruited participants through word of mouth and our informal network of autism and disability-related organizations and community agencies. The study was conducted in two parts. All participants first completed the Gateway Survey, which includes items about whether participants consider themselves to have a disability and/or to be on the autism spectrum (including autistic disorder, Asperger’s disorder, or pervasive developmental disorder–NOS). The survey also includes the six disability items used on the US Census,34 demographic characteristics, and the Autism Spectrum Quotient (AQ).35,36
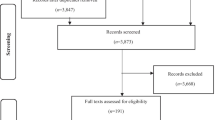
We invited Gateway Project participants who were U.S. residents and considered themselves to be on the autism spectrum to take the healthcare survey, followed by a random sample of non-autistic participants, selected amongst those who matched autistic responders by sex and age group. To address the relatively low proportion of non-autistic people with disabilities in the overall pool of Gateway Project participants, we oversampled people with disabilities by also inviting all Gateway project participants who considered themselves to have a disability and answered yes to at least one US census disability item. We stopped inviting non-autistic participants to take the healthcare survey when the number of non-autistic participants exceeded that of the autistic sample. Sixty-six participants were excluded because responses did not meet data validation standards (for example, responses to item on sex differed between Gateway and Healthcare surveys). We also excluded university students who had been incentivized with extra credit points to participate in the Gateway Survey.
Instrument Selection and Adaptation
Our academic and community partners collaboratively identified which constructs to measure, chose assessment instruments, and adapted instruments to be more accessible or relevant to autistic adults. Adaptations to increase accessibility included minor modifications to wording to make language more specific or clear, addition of hotlinks with definitions of technical or ambiguous terms, and addition of prefaces with more specific instructions. In one case, we created two additional items to increase relevance. For consistency, we adapted all items to be in the first person voice. To address the anxiety some partners reported experiencing when they did not know how to answer a question with complete accuracy or did not have a way to elaborate on their answers, we added a comment box on every page.
Data Collection
We collected data on patient-provider communication using six items adapted from 2007 Health Information National Trends Survey (HINTS).37–40 We added two new items on expressive and receptive comprehension, because community partners felt this was not adequately addressed in the initial scale. Participants were asked to think about their interactions with healthcare providers over the past year and rate how often their providers did each behavior. Responses used a 4-point Likert scale with anchors of “Never” to “Always”. We analyzed items both individually and by summing the responses into a composite score (range 8–32; higher scores indicate higher satisfaction). The original HINTS patient–provider communication scale had a Cronbach’s alpha of 0.9.41
We measured healthcare self-efficacy using the items adapted from the Chronic Disease Self-Management Studies by Lorig and colleagues.42,43 Participants were first presented with a list of chronic medical conditions and asked to indicate which ones they had been diagnosed with by a healthcare professional. Participants with at least one chronic medical condition then completed the Self-Efficacy for Managing Chronic Disease 6-Item Scale (which was found to have a Cronbach’s alpha 0.91 in prior studies).42 All participants were also asked to complete nine additional items about healthcare self-efficacy, selected from Lorig’s original longer instrument.43 Those items were adapted to be applicable to individuals whether or not they had any chronic illnesses. All items were rated on a scale of 1–10, with anchors of “not at all confident” and “totally confident” and summed into a composite score (range 9–90 for general healthcare self-efficacy, 6–60 for chronic condition self-efficacy; higher values indicate greater self-efficacy).
We collected data on unmet healthcare needs and healthcare utilization, using items adapted from the 2002/2003 Joint US Canada Survey44,45 and the 2007 National Health Interview Survey (NHIS) Questionnaire—Adult Access to Health Care & Utilization.46,47 Specifically, we measured unmet healthcare needs using the item “During the past 12 months, there was a time when I felt that I needed the following type of healthcare, but did not receive it. (Check all that apply).” Response options included six types of healthcare (e.g., “medical care for a physical health problem”, “mental healthcare or counseling”). Additional items assessed whether participants had a primary care provider (PCP), the number of emergency department visits, outpatient visits, and hospitalizations within the past 12 months, and receipt of a variety of preventive care services.
We used a single item to measure overall health status, with response options of Excellent, Very good, Good, Fair, and Poor.48 Results from additional instruments focusing on barriers or facilitators to care and perceptions of bias will be reported separately.
Data Analysis
Psychometric Assessment of Adapted Instruments
We used our CBPR process to ensure face and content validity. The team used an iterative process, reviewing and adapting instruments until all community and academic partners felt the survey was clear and adequately addressed the most important constructs. We assessed convergent validity by comparing responses between instruments we hypothesized would be associated with each other. We assessed the internal consistency reliability of our three adapted composite scales for each population (autistic vs. non-autistic) using Cronbach’s alpha.
Demographic Characteristics and Healthcare Experiences
We conducted bivariate analyses comparing the responses of autistic and non-autistic adults for all available demographic characteristics and health services outcomes using two sample t-tests and chi-square tests. We used logistic and linear regression to assess for independent associations with dichotomous and continuous outcomes, respectively. Our main predictor was population (autistic adults vs. non-autistic adults). All models were also adjusted for age, sex, race/ethnicity (non-Hispanic White, yes/no), personal and parental educational attainment (high school or less, some college, bachelor’s degree, any graduate work), income (< $25,000, $25,000–49,999, ≥ $50,000), health insurance (none, Medicare/Medicaid only, private insurance, other), and overall health status (excellent/good vs. fair/poor). Parental education is often used as an additional proxy measure for socioeconomic status (SES) in people with developmental disabilities.49 We conducted separate analyses for each outcome measure, analyzing responses to the patient–provider communication scale and the general and chronic illness healthcare self-efficacy scales as continuous outcomes. We dichotomized the number of outpatient visits in the past year into 0–3 vs. ≥ 4, and the number of emergency department visits into zero vs. ≥ 1. All other outcomes were collected and analyzed as dichotomous variables.
Sensitivity Analyses
Primary analyses included all participants who indicated that they were on the autism spectrum. Due to changes in diagnostic criteria over time and difficulty obtaining diagnoses in adulthood, many adults who meet diagnostic criteria for autism spectrum disorder (ASD) do not carry formal medical diagnoses.50 Moreover, screening instruments such as the Autism Quotient have limited accuracy.35 We felt that using formal diagnoses or a screening instrument to determine eligibility would unnecessarily exclude a large number of autistic adults who may still experience healthcare disparities related to being on the autism spectrum. Sensitivity analyses limited the autistic group to those who score a 26 or greater on the Autism Quotient.35 We also conducted a sensitivity analysis limiting the non-autistic sample to only those without other disabilities. Finally, we compared all healthcare outcomes for participants with diagnoses of autistic disorder vs. Asperger’s disorder.
We analyzed data using STATA software (version 11.0, Statacorp, LP, College Station, Texas).
RESULTS
Study Sample
Two hundred and nine autistic adults and 228 non-autistic adults completed the survey. Table 1 shows participant characteristics. A majority of autistic participants were diagnosed with Asperger’s disorder. Amongst the autistic sample, there was no difference in Autism Quotient scores between those with or without formal diagnoses. Fifty-five (24 %) of the non-autistic participants had a disability. Participants resided in 47 different US states (including the District of Columbia).
Psychometric Properties of Adapted Measures
All adapted measures with composite scores had good to excellent internal consistency reliability (alphas .83–.92; Tables 2 and 3). When comparing results from the autistic and non-autistic samples, the scales demonstrated slightly lower internal consistency in the autistic sample, but the differences in alphas between the two samples were extremely small (no greater than 0.03). All alphas were comparable to what has been reported in the literature for the original measures.
There was strong convergent validity, with significant correlations amongst all scales in the expected direction. For example, there was a strong correlation (correlation coefficient 0.7, p < 0. 001) between general healthcare and chronic condition self-efficacy, and between both measures of self-efficacy and unmet healthcare needs.
Healthcare Experiences
When compared to non-autistic adults, autistic adults had significantly lower scores on each of the items on the patient–provider communication scale and the self-efficacy scales. In multivariate analyses, after adjustment for age, sex, race/ethnicity, personal and parental educational level, income, type of health insurance, and overall health status, autistic adults had lower composite scores for patient–provider communication (beta coefficient −1.9, CI −2.9 to −0.9), general healthcare self-efficacy (beta coefficient −11.9, CI −14.0 to −8.6), and chronic condition self-efficacy (beta coefficient −4.5, CI −7.5 to −1.6) than non-autistic adults (Tables 2 and 3).
Table 4 shows responses to items about unmet healthcare needs and healthcare utilization. In multivariate analyses, autistic adults had significantly higher odds of unmet healthcare needs related to physical health (OR 1.9 CI 1.1–3.4), mental health (OR 2.2, CI 1.3–3.7), and prescription medications (OR 2.8, CI 2.2–7.5). Though autistic adults were as likely as non-autistic adults to have a PCP or have their blood pressure checked, and had similar numbers of outpatient appointments or hospitalizations, they were less likely to have received a tetanus vaccine (OR 0.5, CI 0.3–0.9), and, if female, less likely to have received a Papanicolaou smear in the past 3 years (OR 0.5, CI 0.2–0.9). They also had more than twice the odds of using the emergency department (ED) in the past year (OR 2.1, CI 1.8–3.8).
Sensitivity analyses limiting autistic participants to only those with Autism Quotient scores ≥ 26 reached similar conclusions as those from primary analyses. Analyses limiting the non-autistic sample to people without disabilities strengthened the magnitude of findings, but did not qualitatively change conclusions. In multivariate analyses, participants with diagnoses of Asperger’s disorder were less likely than those with diagnoses of autistic disorder to use the ED. There were no differences related to diagnosis in any of the other healthcare items or composite scores assessed in the study.
DISCUSSION
Researchers have argued that obtaining input from individuals with developmental disabilities is critical to producing scientific information that is valid, ethical, and inclusive of their perspectives.51–55 The CBPR process allowed us to successfully adapt instruments to directly collect data from autistic individuals. To our knowledge, this is the first study to directly obtain data from autistic adults about their perceptions of unmet healthcare needs, patient-provider communication, and healthcare self-efficacy.
The literature includes multiple conceptualizations and definitions of “disparities”.56,57 We have chosen to frame our findings as healthcare disparities based on the Healthy People 2020 conceptualization, which defines disparities as differences that “adversely affect groups of people who have systematically experienced greater obstacles to health based on [a number of characteristics, including] disability”.58 Several studies have noted that people with developmental disabilities experience important healthcare disparities,4 but most have primarily included people with intellectual disabilities and none have focused on autistic adults. Our study suggests that autistic adults who use the Internet may also experience important healthcare disparities. Future research is needed to better understand the factors that contribute to the disparity and ways to eliminate it.
Our survey found an interesting pattern of similarities and differences in healthcare utilization between autistic and non-autistic adults. The vast majority of participants in both groups reported that they had a PCP, and the two groups had similar outpatient clinic utilization. However, the receipt of outpatient care does not necessarily mean that care is effective. Additionally, providers have reported feeling uncomfortable with their level of training regarding autistic patients.59 While it may be expected that autistic participants report worse patient–provider communication and lower patient self-efficacy, our study showed that they further report greater unmet healthcare needs, higher use of the ED, and lower utilization of some preventive services. Preventive services requiring providers to more effectively communicate or coordinate care (e.g., Pap smears) were more greatly affected than those done routinely (e.g., blood pressure measurement). Together, these findings point to the existence of a significant problem in how healthcare is delivered to autistic adults.
Our study has several limitations. The cross-sectional design precludes the ability to draw causal inferences. Our Internet-based recruitment strategy resulted in a convenience sample that may not be representative of the autistic population, the general population, or even the population of people who have access to the Internet. However, it is encouraging that non-autistic participants in our sample had rates of unmet healthcare needs similar to those found in large population-based studies.45 Autistic individuals also had rates of preventive health utilization within the range of what has been noted in other studies of people with disabilities.9,10,60 We had an over-representation of female participants, as is often, unfortunately, the case in online surveys.60,61 Given the constraints of an online survey, we did not independently confirm ASD diagnoses or any other self-report variables. However, secondary analyses restricting the sample to only those with high Autism Quotient scores did not qualitatively change the results. Our study notes increased ED use in the autistic sample, but we did not collect data on the reason for the ED visits.
Our sample only included participants with access to the Internet. A majority of participants in both the autistic and non-autistic sample received at least some college education and were non-Hispanic White. Our findings cannot be generalized to adults who do not use the Internet, be it due to lack of access, socioeconomic factors, preference, or ability. Nor can they be generalized to populations with lower educational attainment or to individuals from racial or ethnic minority communities. However, we feel that the existence of healthcare disparities in this sample is still an important finding, as these individuals may otherwise be perceived as having fewer disability-related barriers to care. A recent study found that young adults on the autism spectrum whose parents reported they could perform four activities of daily living independently very well were less likely to receive medical services for diagnosis or evaluation related to disability than those who could not.62 Our study furthers that finding, highlighting that high educational attainment does not necessarily eliminate the existence of important barriers to quality healthcare. We did not collect data on how often or in what ways participants access the Internet, nor did we collect data from participants without access to the Internet. Though one might speculate that autistic individuals who do not use the Internet may have greater barriers (e.g., due to greater communication difficulties), they also may benefit from greater support from family members, caregivers, or support staff to effectively access healthcare.
Our study has several important implications. A CBPR approach may facilitate the inclusion of people with disabilities in research, both as members of the research team and as study participants. Our CBPR process allowed us to adapt instruments to be accessible to this sample of autistic adults, primarily by increasing the clarity and precision of the language used in the instruments. Future studies are needed to further validate our adapted measures in other samples of autistic adults.
American Psychiatric Association (APA) has proposed new diagnostic criteria for the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which includes combining autistic disorder, Asperger’s disorder, and pervasive developmental disorder–NOS into one diagnosis.63 Part of the rationale for this change is the lack of clear and consistent distinctions between diagnoses.64 The lack of significant differences by diagnosis type in almost all reported healthcare experiences may be reflective of this issue.
Being that our study was designed prior to the announcement of the proposed changes, we did not collect data to predict whether participants will meet the revised DSM-5 diagnostic criteria. There has been considerable controversy over the proposed criteria, with some studies predicting a significant reduction in the number of people who will meet criteria, especially amongst those diagnosed with Asperger’s disorder or without intellectual disabilities.65,66 There is concern that those individuals will be deprived of services, self-understanding, and the right to accommodations, which would otherwise be mandated by the Americans with Disabilities Act. The existence of healthcare disparities in our sample, many of whom may be at risk for no longer meeting criteria, highlights these potential negative consequences, as not having a diagnosis may deprive patients and their providers of possible insights, strategies, and accommodations to try to improve healthcare experiences.
Clinicians should be both aware of the potential healthcare disparities experienced by autistic adults—including adults such as those in our sample with overall high educational attainment and access to the Internet—and open to accommodations and strategies that may improve healthcare. Some examples of accommodations and strategies that have been useful to our team of patients and providers include: offering patients an alternative to an over-stimulating waiting room; allowing patients to communicate in their preferred mode (e.g., writing or typing); using precise, specific language; allowing extra time for patients to process information; providing very concrete, step-by-step written instructions for how to obtain necessary prescriptions, tests, or referrals; and clarifying the role of supporters. Our academic-community partnership is currently conducting a National Institute of Mental Health-funded study to better understand strategies and accommodations that improve healthcare for autistic adults, and to develop and evaluate an interactive toolkit for autistic adults and their PCPs. The toolkit will include a way for patients to generate customized accommodations reports, as well as information about health and healthcare targeted toward autistic patients, their supporters, and PCPs. Future research is needed to assess the effectiveness of such tools in improving health outcomes.
REFERENCES
Office of Autism Research Coordination, National Institute of Mental Health, on behalf of the Interagency Autism Coordinating Committee. 2010 IACC Autism Spectrum Disorder research portfolio analysis report. Washington, DC July 2012.
Sinclair J. Why I dislike “person first” language. http://web.archive.org/web/20080616063934/http://web.syr.edu/∼jisincla/person_first.htm. Accessed October 10, 2012.
Nicolaidis C, Raymaker D, McDonald K, et al. Collaboration strategies in nontraditional community-based participatory research partnerships: lessons from an academic-community partnership with autistic self-advocates. Prog Community Health Partnersh. 2011;5(2):143–50.
Krahn GL, Hammond L, Turner A. A cascade of disparities: health and health care access for people with intellectual disabilities. Ment Retard Dev Disabil Res Rev. 2006;12(1):70–82.
Durvasula SBH. Health inequalities in people with intellectual disability: strategies for improvement. Health Promot J Aust. 2001;11:27–31.
Janicki MP, Dalton AJ, Henderson CM, Davidson PW. Mortality and morbidity among older adults with intellectual disability: health services considerations. Disabil Rehabil. 1999;5(6):284–94.
Lishner DM, PhD MR, Levine P, Patrick D. Access to primary health care among persons with disabilities in rural areas: a summary of the literature. J Rural Heal. 1996;12(1):45–53.
Sullivan WF, Heng J, Cameron D, et al. Consensus guidelines for primary health care of adults with developmental disabilities. Canadian Family Physician. 2006;52(11):1410.
Lewis MA, Lewis CE, Leake B, King BH. The quality of health care for adults with developmental disabilities. Public Health Rep (1974-). 2002;174–84.
Wei W, Findley PA, Sambamoorthi U. Disability and receipt of clinical preventive services among women. Women’s Health Issues. 2006;16(6):286–96.
Coughlin TA, Long SK, Kendall S. Health care access, use, and satisfaction among disabled Medicaid beneficiaries. Health Care Financing Rev. 2002;24(2):115–36.
Wan TTH, Arling G. Differential use of health services among disabled elderly. Res Aging. 1983;5(3):411.
Diab ME, Johnston MV. Relationships between level of disability and receipt of preventive health services. Arch Phys Med Rehabil. 2004;85(5):749–57.
Havercamp SM, Scandlin D, Roth M. Health disparities among adults with developmental disabilities, adults with other disabilities, and adults not reporting disability in North Carolina. Public Health Rep. 2004;119(4):418–26.
Ramirez A, Farmer GC, Grant D, Papachristou T. Disability and preventive cancer screening: results from the 2001 California Health Interview Survey. Am J Public Health. 2005;95(11):2057–64.
Reynolds F, Stanistreet D, Elton P. Women with learning disabilities and access to cervical screening: retrospective cohort study using case control methods. BMC Publ Health. 2008;8(1):30.
Burns TJ, Batavia AI, Smith QW, DeJong G. Primary health care needs of persons with physical disabilities: what are the research and service priorities? Arch Phys Med Rehabil. 1990;71(2):138–43.
Chau N. More than ramps. a guide to improving healthcare quality and access for people with disabilities. Br Med J. 2007;61(4):367–367.
Rimmer JH, Braddock D. Health promotion for people with physical, cognitive, and sensory disabilities: an emerging national priority. Am J Heal Promot. 2002;16(4):220–4.
Becker H, Stuifbergen A, Tinkle M. Reproductive health care experiences of women with physical disabilities: a qualitative study. Arch Phys Med Rehabil. 1997;78(12S5):26–33.
Tyler CV, Schramm SC, Karafa M, Tang AS, Jain AK. Chronic disease risks in young adults with autism spectrum disorder: forewarned is forearmed. Am J Intellect Dev Disabil. 2011;116(5):371–80.
Chakrabarti S, Fombonne E. Pervasive developmental disorders in preschool children: confirmation of high prevalence. Am J Psychiatry. 2005;162(6):1133–41.
Chakrabarti S, Fombonne E. Pervasive developmental disorders in preschool children. JAMA. 2001;285(24):3093–9.
Williams E, Thomas K, Sidebotham H, Emond A. Prevalence and characteristics of autistic spectrum disorders in the ALSPAC cohort. Dev Med Child Neurol. 2008;50(9):672–7.
Keen D, Ward S. Autistic spectrum disorder: a child population profile. Autism. 2004;8(1):39–48.
Jordan CJ. Evolution of autism support and understanding via the World Wide Web. Intellect Dev Disabil. 2010;48(3):220–7.
Robertson S. Information technology & the autistic culture: Influences, empowerment, & progression of IT usage in advocacy initiatives. Paper presented at: Autreat; June, 2007, 2007; Pennsylvania, PA.
Biever C. Web removes social barriers for those with autism. New Scientist. 2007;2610:26–7.
Murray D, Aspinall A, Getting IT. Using information technology to empower people with communication difficulties. London: Jessica Kingsely Publishers; 2006.
Blume, H. Autistics are communicating in cyberspace. http://www.nytimes.com/library/cyber/techcol/063097techcol.html. Accessed October 10, 2012.
Jones L, Wells K. Strategies for academic and clinician engagement in community-participatory partnered research.[see comment]. JAMA. 2007;297(4):407–10.
Viswanathan M, Ammerman A, Eng E, et al. Community-based participatory research: Assessing the evidence. Rockville, MD: Agency for Healthcare Research and Quality July 2004. Evidence Report/Technology Assessment Number 99.
Nicolaidis C, Raymaker D, McDonald K, et al. Collaboration strategies in non-traditional CBPR partnerships: lessons from an academic-community partnership with autistic self-advocates. Progress in Community Health Partnerships: Research, Education, and Action. In press.
Bureau USC. Disability Status: 2000 Census Brief 2003.
Woodbury-Smith MR, Robinson J, Wheelwright S, Baron-Cohen S. Screening adults for Asperger Syndrome using the AQ: a preliminary study of its diagnostic validity in clinical practice. J Autism Dev Disord. 2005;35(3):331–5.
Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians.[erratum appears in J Autism Dev Disord 2001 Dec;31(6):603]. J Autism Dev Disord. 2001;31(1):5–17.
Cantor D, Covell, J., Davis, T., Park, I., & Rizzo, L. Health Information National Trends Survey (HINTS). http://hints.cancer.gov/docs/HINTS2007FinalReport.pdf. Accessed October 10, 2012.
Hong T. Internet health information in the patient-provider dialogue. CyberPsychology Behav. 2008;5:587–9.
Marks R, Ok H, Joung H, Allegrante JP. Perceptions about collaborative decisions: perceived provider effectiveness among 2003 and 2007 Health Information National Trends Survey (HINTS) respondents. J Heal Commun. 2010;15(Suppl 3):135–46.
Ok H, Marks R, Allegrante JP. Perceptions of health care provider communication activity among American cancer survivors and Adults Without Cancer Histories: an analysis of the 2003 Health Information Trends Survey (HINTS) Data. J Health Commun. 2008;13(7):637–53.
Smith SG, Wolf MS, von Wagner C. Socioeconomic status, statistical confidence, and patient-provider communication: an analysis of the Health Information National Trends Survey (HINTS 2007). J Heal Commun.15 Suppl 3:169–85.
Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4(6):256–62.
Lorig K, Stewart A, Ritter P, Gonzalez V, Laurent D, Lynch J. Outcome measures for health education and other health care interventions. Thousand Oaks: Sage Publications; 1996.
Blackwell, D., Gentleman, J., Martin, M., Ng, E.,Sanmartin, C., Simile, C. Joint Canada/United States Survey of Health: Findings and Public-use Microdata File. http://www.statcan.gc.ca/pub/82m0022x/2003001/pdf/4228656-eng.pdf. Accessed 02/25/2009.
Sanmartin C, Berthelot J-M, Ng E, et al. Comparing health and health care use in Canada and the United States. Health Aff. 2006;25(4):1133–42.
Pleis JR, Lucas JW. Summary health statistics for U.S. adults: National Health Interview Survey, 2007. Vital Health Stat—Series 10: Data From the National Health Survey. 2009;240:1–159.
CDC. National Health Interview Survey (NHIS)—Adult access to health care & utilization. http://www.ihis.us/ihis/resources/surveys_pdf/survey_form_ih2007_fam.pdf. Accessed October 10, 2012.
Ware JE, GlaxoSmithKline. How to score and interpret single-item health status measures: a manual for users of the of the SF-8 health survey:(with a supplement on the SF-6 health survey): QualityMetric, Inc.; 2001.
Emerson E, Graham H, Hatton C. The measurement of poverty and socioeconomic position in research involving people with intellectual disability. Int Rev Res Ment Retard. 2006;32:77–108.
Wing L, Potter D. The epidemiology of autistic spectrum disorders: is the prevalence rising? Ment Retard Dev Disabil Res Rev. 2002;8(3):151–61.
Koch T, Marks J, Tooke E. Evaluating a community nursing service: listening to the voices of clients with an intellectual disability and/or their proxies. J Clin Nurs. 2001;10(3):352–63.
Aman MGHB. Reactions to “ethical challenges and complexities of including people with intellectual disability as participants in research” by dr teresa lacono. J Intellect Dev Disabil. 2006;31(3):180–2.
Kottorp A, Bernspang B, Fisher AG. Validity of a performance assessment of activities of daily living for people with developmental disabilities. J Intellect Disabil Res. 2003;47(Pt 8):597–605.
Ham M, Jones N, Mansell I, Northway R, Price L, Walker G. ‘I’m a researcher!’ working together to gain ethical approval for a participatory research study. J Learn Disabil. 2004;8(4):397–407.
McVilly K, Dalton AJ. Commentary on lacono (2006): “ethical challenges and complexities of including people with intellectual disability as participants in research”. J Intellect Dev Disabil. 2006;31(3):186–8.
Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health. 2006;27:167–94.
Carter-Pokras O, Baquet C. What is a“ health disparity”? Public Health Rep. 2002;117(5):426.
U.S. Department of Health and Human Services. The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020. About Health People: Disparities. http://www.healthypeople.gov/2020/about/disparitiesAbout.aspx. Accessed July 10, 2012.
Bruder MB, Kerins G, Mazzarella C, Sims J, Stein N. Brief report: the medical care of adults with autism spectrum disorders: identifying the needs. J Autism Dev Disord. 2012;42(11):2498–504.
Sax LJ, Gilmartin SK, Bryant AN. Assessing response rates and nonresponse bias in web and paper surveys. Res High Educ. 2003;44(4):409–32.
Rhodes SD, Bowie DA, Hergenrather KC. Collecting behavioural data using the world wide web: considerations for researchers. J Epidemiol Community. 2003;57(1):68–73.
Shattuck PT, Wagner M, Narendorf S, Sterzing P, Hensley M. Post-high school service use among young adults with an autism spectrum disorder. Arch Pediatr Adolesc Med. 2011;165(2):141–6.
American Psychiatric Association. DSM-5 proposed criteria for autism spectrum disorder designed to provide more accurate diagnosis and treatment. January 20, 2012. http://www.dsm5.org/Documents/12-03%20Autism%20Spectrum%20Disorders%20-%20DSM5.pdf. Accessed July 10, 2012.
American Psychiatric Association. DSM-5 Development: A 05 Autism Spectrum Disorder—Rationale. http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=94#. Accessed July 10, 2012.
Mattila M-L, Kielinen M, Linna S-L, et al. Autism spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: an epidemiological study. J Am Acad Child Adolesc Psychiatr. 2011;50(6):583–92.e511.
McPartland JC, Reichow B, Volkmar FR. Sensitivity and specificity of proposed DSM-5 diagnostic criteria for autism spectrum disorder. J Am Acad Child Adolesc Psychiatr. 2012;51(4):368–83.
Acknowledgements
Contributors
We would like to thank Gateway Project investigators Morton Ann Gernsbacher, PhD and Jennifer Stevenson, PhD, for their collaboration on the Gateway Project and their review of the healthcare study materials and publications. We would like to thank Roberta Delaney, Dean Westwood, MS, and the Oregon Institute on Disability and Development (OIDD) Community Partners Council (including Rhonda Way, Emily Holmes, Jerry Pattee, and Judy Cunio) for their help with study development and recruitment efforts. We would also like to thank the Autistic Self-Advocacy Network for their help with recruitment and dissemination, and Martha Gerrity, MD, MPH, for her review of this manuscript.
Funders
This project was funded by the Oregon Clinical and Translational Research Institute (OCTRI), grant number UL1 RR024140 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. The Gateway Project is funded by the Vilas Trust Fund.
Conflict of Interest
None of the authors have any potential conflicts of interest to disclose.
Prior Presentations
Preliminary results from this study have been presented at the Family Medicine Education Consortium NE Region Meeting & Residency Fair (Hershey, PA, October, 2010), the Society of General Internal Medicine Annual Meeting (Phoenix, Arizona, May, 2011), Developmental Disabilities: Update for Health Professionals (San Francisco, CA, March, 2011), the Scientific Meeting for Autism Spectrum Conditions (WTAS, Berlin, Germany, February, 2011), and Oregon Health & Sciences University Psychiatry Grand Rounds (Portland, OR, March, 2011).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Nicolaidis, C., Raymaker, D., McDonald, K. et al. Comparison of Healthcare Experiences in Autistic and Non-Autistic Adults: A Cross-Sectional Online Survey Facilitated by an Academic-Community Partnership. J GEN INTERN MED 28, 761–769 (2013). https://doi.org/10.1007/s11606-012-2262-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-012-2262-7