
ABSTRACT
Background
Little research has examined the incidence, clinical relevance, and predictors of medication reconciliation errors at hospital admission and discharge.
Objective
To identify patient- and medication-related factors that contribute to pre-admission medication list (PAML) errors and admission order errors, and to test whether such errors persist in the discharge medication list.
Design, Participants
We conducted a cross-sectional analysis of 423 adults with acute coronary syndromes or acute decompensated heart failure admitted to two academic hospitals who received pharmacist-assisted medication reconciliation during the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL–CVD) Study.
Main Measures
Pharmacists assessed the number of total and clinically relevant errors in the PAML and admission and discharge medication orders. We used negative binomial regression and report incidence rate ratios (IRR) of predictors of reconciliation errors.
Key Results
On admission, 174 of 413 patients (42%) had ≥1 PAML error, and 73 (18%) had ≥1 clinically relevant PAML error. At discharge, 158 of 405 patients (39%) had ≥1 discharge medication error, and 126 (31%) had ≥1 clinically relevant discharge medication error. Clinically relevant PAML errors were associated with older age (IRR = 1.46; 95% CI, 1.00– 2.12) and number of pre-admission medications (IRR = 1.17; 95% CI, 1.10–1.25), and were less likely when a recent medication list was present in the electronic medical record (EMR) (IRR = 0.54; 95% CI, 0.30–0.96). Clinically relevant admission order errors were also associated with older age and number of pre-admission medications. Clinically relevant discharge medication errors were more likely for every PAML error (IRR = 1.31; 95% CI, 1.19–1.45) and number of medications changed prior to discharge (IRR = 1.06; 95% CI, 1.01–1.11).
Conclusions
Medication reconciliation errors are common at hospital admission and discharge. Errors in preadmission medication histories are associated with older age and number of medications and lead to more discharge reconciliation errors. A recent medication list in the EMR is protective against medication reconciliation errors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Medication errors, particularly unexplained discrepancies in medication regimens across different sites of care, are prevalent among hospitalized patients. One study reported that 67% of inpatients had at least one error on their admission medication lists.1 These errors can increase the risk of adverse drug events (ADEs) during hospitalization or following discharge.2–4 Hospitals attempt to avert medication errors and ADEs by implementing medication reconciliation, the process by which a clinician compiles an accurate list of all medications that an individual is currently taking5–7 and uses that list to provide correct medications anywhere within the health care system.8
Hospital-based medication reconciliation is to be completed upon admission, transfer, and at discharge.6 To compile an accurate list of medications, clinicians may use several sources of information during the medication reconciliation process, including pill bottles, the patient and/or family members, outpatient records, electronic medical records (EMR), and pharmacy records.5
At each point in the care continuum, patient characteristics and his/her medications may influence the medication reconciliation process. For example, health literacy and medication understanding may affect a patient’s ability to accurately report the medication regimen, possibly leading to errors in medication reconciliation during admission.9,10 Subsequently, errors in the pre-admission medication list (PAML) may persist through hospitalization and contribute to discharge medication errors.11 Little research has examined how patient characteristics and other factors affect the medication reconciliation process—those that have are generally small, single site studies (or two sites within one hospital system).11–15 Also few studies have examined how errors in the medication history-taking process (PAML errors) affect the likelihood of discharge errors.
We aimed to identify which patient- and medication-related factors contribute to PAML errors and admission order errors, and test whether such errors are carried through to the discharge medication list. We hypothesized that the absence of a medication list in the EMR, more medications on admission, low health literacy, and impaired cognitive function would be associated with PAML errors. We also predicted PAML errors would be associated with admission and discharge medication order errors.
METHODS
Study Design and Setting
We conducted a cross-sectional analysis of factors associated with medication errors among intervention patients from the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL–CVD) Study. The PILL–CVD Study was a randomized controlled trial at two academic hospitals—Vanderbilt University Hospital in Nashville, TN and Brigham and Women’s Hospital in Boston, MA.
Patient Population
We enrolled 862 patients between May 2008 and September 2009. Eligible patients were at least 18 years of age and admitted with acute coronary syndromes (ACS) or acute decompensated heart failure (ADHF). The rationale and design of this study, including a full description of inclusion and exclusion criteria, has been published.16
Patients were eligible for inclusion in these analyses if they were randomized to the intervention arm and received pharmacist-assisted medication reconciliation during hospitalization.
Patients were screened for eligibility shortly after admission and approached for written informed consent. Consenting participants completed a baseline assessment of patient-related measures (see below). The Institutional Review Boards at both study sites approved all materials and procedures.
Patient-Related Measures
Demographic characteristics included age, gender, race, ethnicity, living alone vs. not, and health insurance.
Cognitive function was assessed by the Mini-Cog.17–19 Patients were asked to recall three words after performing a clock draw test. Scores range from 0–5, where 0–2 points indicates dementia. We treated cognition as a dichotomous variable in our analyses (no cognitive impairment vs. dementia).
Health literacy, assessed using the short Test of Functional Health Literacy in Adults (s-TOFHLA), is a measure of a patient’s ability to understand written information encountered in the health care setting.20 Scores range from 0–36 and were categorized as adequate (23–36), marginal (17–22), or inadequate health literacy (0–16). We treated health literacy as a dichotomous variable in our analyses (inadequate/marginal vs. adequate).
The Medication Understanding Questionnaire (MUQ) was adapted from prior instruments.9 A random number table was used to select up to five medications from a patient’s PAML. The patient was given the name of each randomly selected medication and asked to provide the indication (1 point); strength of each unit (½ point), number of units per dose (½ point); and the frequency (1 point). The MUQ score ranges from 0 to 3 per medication, with the composite score being the average of the MUQ score across all medications tested. Higher scores indicate better medication understanding.
Pre-admission medication adherence was measured using the Morisky medication adherence scale.21 The four yes/no questions ask patients about forgetfulness, carelessness, and cessation of medications if s/he feels better or worse. Each yes answer counts for 1 point, and the possible score ranges from 0 to 4. Lower scores indicate better adherence.
Medication-Related Measures
From the EMR, we abstracted several variables. Patients seen in an affiliated clinic, emergency department, or hospital within 90 days prior to admission with a documented medication list were categorized as having a pre-admission medication list in the EMR (dichotomous). We assessed the number of pre-admission and discharge prescription medications (continuous) and the number of prescription medication changes made between admission and discharge (continuous). Each adjustment in dose, frequency, or route; discontinuation; or initiation of a medication counted as a change. If a medication was listed at both admission and discharge but dose or frequency was not documented, we assumed there was no change.
Outcome Measures: Errors in Medication Reconciliation
During hospital admission and prior to study enrollment, the treating physician took a medication history and documented the patient’s PAML in the EMR. The treating physicians ordered any medications to be administered in the hospital (admission orders) and, later, the post-discharge home medication regimen (discharge medications).
As part of the PILL–CVD intervention, pharmacists followed a structured protocol for medication reconciliation: first by obtaining a “reference standard” PAML, and then comparing that standard to the treating physician’s PAML, then to the admission orders, and finally to the discharge medications. The pharmacists tallied the number of errors in the treating physicians’ PAML and unintentional discrepancies in admission orders and discharge medications compared to the pharmacist’s reference standard list immediately after each step in the medication reconciliation process. All unintentional discrepancies were considered to be errors. The pharmacists also tallied how many of these errors were clinically relevant, i.e. important enough to contact the treating physicians. Treating physicians were informed of all clinically relevant errors so that they could be promptly addressed.
Primary Statistical Analyses
Frequency distributions and correlations were evaluated first. Using negative binomial logistic regression, we tested the association between patient- and medication-related factors and both the total number of medication errors and the number of clinically relevant errors. We constructed separate models for PAML errors (outcome 1), admission medication order errors (outcome 2), and discharge medication order errors (outcome 3). Because of the potential downstream effect of PAML errors, we analyzed models for outcomes 2 and 3 both with and without PAML errors. Regression diagnostics were performed to assess the fulfillment of model assumptions. Results are reported as incidence rate ratios (IRR) and 95% confidence intervals.
Secondary Analyses
For outcome 1, we performed a sensitivity analysis by excluding participants who had no pre-admission prescription medications.
For outcome 2, we tested whether the number of PAML errors mediated the relationship between covariates (age and number of pre-admission medications) and admission order errors.
For each outcome, effect modification was assessed through 2 sets of stratified analyses. First, we analyzed the medication errors for individuals with less than the median or greater than or equal to the median number of pre-admission medications (median = 8). Second, we assessed medication errors based on the presence or absence of a medication list in the EMR within the 90 days prior to admission. These factors had been demonstrated in prior research to predict medication reconciliation errors.12,14
RESULTS
Among 430 patients randomized to the PILL–CVD intervention, 423 (98.4%) had sufficient data available for these analyses (Table 1). The mean age was 61 years (SD = 14), 173 (41%) were female, and 319 (75%) were white. Ninety-two participants (22%) had inadequate or marginal health literacy. Forty-five percent of participants had a medication list documented in the EMR within 90 days prior to admission. Participants took a mean of 8 pre-admission prescription medications (SD = 5), had a mean of 7 medication changes during hospitalization (SD = 4), and were discharged with a mean of 10 prescription medications (SD = 4).
In a subset of participants who had PAML errors, the types of errors identified were: omission of a medication (40%), inclusion of a medication the patient was not supposed to be taking—an error of commission (27%), difference in dose (15%), difference in frequency (10%), and substitutions (7%). Likewise, at discharge errors were: omission (25%), commission (35%), difference in dose (18%), difference in frequency (15%), and substitutions (5%).
PRIMARY OUTCOMES: PAML ERRORS, ADMISSION AND DISCHARGE MEDICATION ORDER ERRORS
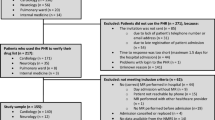
Figure 1 shows the sample size for analysis of each outcome. For outcome 1 (PAML errors), 174 patients (42%) had an error in the medication history performed by their treating physicians, and an additional 73 patients (18%) had a clinically relevant error. For outcome 2, 78 patients (19%) had an admission order error, and another 38 patients (10%) had a clinically relevant error. For outcome 3 (discharge order errors), 158 patients (40%) had an error, and an additional 126 patients (32%) had a clinically relevant error. There was no significant difference in the rate of PAML errors and discharge medication errors between the two study sites, but there was a difference in total and clinically relevant admission order errors between sites.

Flow diagram of participants included in analyses.
Figure 2 displays the frequency distribution of total and clinically relevant medication errors for each outcome, excluding participants without errors. The majority of participants with an error had only one. For PAML and admission orders, 42% and 49% (respectively) of total errors were clinically relevant. However, at hospital discharge, 80% of errors were clinically relevant.

Frequency of total and clinically relevant PAML, admission medication order, and discharge medication order errors.
Factors associated with PAML errors are presented in Table 2. Older age was significantly associated with an increased rate of PAML errors in unadjusted analyses and remained associated with clinically relevant PAML errors after adjustment. Inadequate or marginal health literacy was significantly associated with more clinically relevant PAML errors in bivariate but not in multivariable analysis. For every one additional pre-admission prescription medication there was an increase in total and clinically relevant PAML errors (12 and 17%, respectively). Finally, in adjusted analyses, having a medication list available in the EMR within 90 days prior to admission was associated with a 40–46% lower rate of PAML errors.
Admission order errors were more common among patients with older age (Table 3). For each additional pre-admission prescription medication, the rate of total and clinically relevant admission order errors increased by 7% and 12%, respectively, in adjusted models. However, when the number of PAML errors was included in the models as a covariate, the association between pre-admission prescription medications and admission order errors was no longer statistically significant. The number of PAML errors was strongly associated with both total and clinically relevant admission order errors in unadjusted and adjusted analyses.
Both total and clinically relevant discharge medication errors were less common among patients who lived alone and those with cognitive impairment (Table 4). The number of PAML errors was strongly associated with discharge medication errors (IRR = 1.31 per PAML error in adjusted analyses). The number of medication changes made during hospitalization also was significantly associated with discharge medication errors (IRR = 1.06 for each additional medication change in adjusted analyses).
SECONDARY ANALYSES
A sensitivity analysis of factors associated with PAML errors, excluding participants without pre-admission prescription medications, demonstrated consistent findings. When stratified on the presence or absence of a medication list available in the EMR within 90 days prior to admission, the number of pre-admission medications was associated with PAML errors, consistent with the main results. In mediation analyses, the number of PAML errors was found to mediate the effect seen between number of pre-admission prescription medications and admission order errors.
DISCUSSION
We found that medication reconciliation errors at the time of admission and discharge are common and often clinically relevant at two unaffiliated academic medical centers. Factors associated with PAML errors included more pre-admission prescription medications and older age. Having a recent medication list in the EMR was protective against PAML errors. Admission order errors were linked to a greater number of pre-admission prescription medications, an effect that was mediated by the number of PAML errors. Finally, medication errors at the time of discharge increased with the number of PAML errors and medication changes made prior to discharge.
The observed incidence of participants with PAML errors (42%), admission order errors (19%), and discharge errors (40%) concurs with previous studies. A systematic review of PAML error studies revealed that 10–67% of patients had at least 1 PAML error upon admission.1 Admission order errors occurred slightly more often in several,3,22–24 but not all,11 prior studies. Our incidence of discharge medication errors is within the 25–71% incidence found in other studies.4,11,23 Additionally, when we probed a subset of patients who had errors on admission and discharge, we found that the distribution of types of errors (i.e. mostly errors of omission or commission) were similar to prior studies.1,3,12,14,15,23,25
Several factors we found to be associated with medication reconciliation errors, such as older age and number of pre-admission medications, were confirmed by others.11,12,14,15 However, in one study fewer unintentional medication discrepancies were associated with age over 85 compared to age less than 50.12 Herrero–Herrero et al. found that the number of preadmission medications predicted unjustified discrepancies (i.e. medication errors) at discharge.26 Furthermore, Pippins et al. showed that 72% of all potentially harmful discrepancies in admission or discharge orders were due to PAML errors.12 Similarly, we discovered that PAML errors and medication changes made during hospitalization predicted discharge medication errors.
Our results that discharge medication errors were less likely in cognitively impaired patients and those who lived alone deserve comment. Regarding the former, the healthcare providers in our study may have been more cautious when prescribing medications for cognitively impaired patients, particularly prior to hospital discharge.27,28 These patients may have had caregivers at home or in facilities who could inform assembly of the discharge medication regimen. Regarding the latter, Hasan et al. demonstrated that not being married was protective against hospital readmissions.29 Healthcare providers may focus their reconciliation efforts and discharge planning to prevent medication-related events in patients who live alone and may have little functional social support.
We found that having a recent medication list in the EMR was protective against PAML errors, similar to the MATCH study in which patients with a medication list had lower odds of an admission medication reconciliation error.14 We surmise that having a paper or electronic list provides evidence of prior medication management by the patient and/or a healthcare provider. Although perhaps not completely accurate, a previously assembled medication list provides a starting place to perform medication reconciliation on admission. Collectively, these studies underscore the importance of taking an accurate medication history on admission, as most medication errors originate from this step and can be perpetuated.
Interventions to reduce PAML errors have the potential to prevent medication errors during hospitalization. To avoid medication errors at discharge and potential harm thereafter, care transitions interventions have given special attention to medication reconciliation30,31, particularly for older adults and those with caregivers.32,33 To be most effective these efforts must begin at hospital admission, when medication histories are taken. Future interventions should address improving medication history-taking and cost-effective, timely medication reconciliation in order to reduce medication errors.
Our study has several strengths. First, we report on a large cohort of medical inpatients from two unaffiliated hospitals, allowing us to investigate the influence of several patient- and medication-related factors. Furthermore, the relationship between inpatient medication errors and some variables we utilized, such as health literacy and cognition, have not been previously reported. Additionally, we analyzed medication errors at three time points during hospitalization, whereas most prior studies have focused on either admission or discharge errors.
We note possible study limitations. We present a sub-study of a clinical trial which had a moderate consent rate (41%). Participants had ACS or ADHF, limiting the generalizability to individuals with other admitting diagnoses and/or taking fewer medications. We did not investigate medication errors from in-hospital transfers nor assess the clinical impact of medication errors, though the relationship between total errors, clinically relevant errors, and ADEs have been described in several prior studies.3,4,11,12,14,15,22,23,34 Clinically relevant medication errors were classified at the discretion of the pharmacists, thereby introducing possible bias in the judgment of these outcomes. The potential of errors to cause harm was not formally adjudicated by a blinded panel of clinicians. Our results may not be generalizable to smaller, community-based facilities or those with mostly paper-based medical records. Lastly, because both study sites utilize PAML-building software in their EMRs the error rates may be lower than in other hospitals.35
CONCLUSIONS
Medication reconciliation errors occur frequently on hospital admission and discharge. Older age and number pre-admission medications predicted PAML errors and admission order errors, whereas PAML errors and medication changes during hospitalization were associated with discharge medication errors.
In summary, errors in compiling the pre-admission medication list lead to errors in admission orders as well as discharge medications and are the strongest predictor of clinically relevant medication errors throughout hospitalization. Interventions to construct accurate pre-admission medication histories and to verify the accuracy of discharge orders in patients at high risk for medication errors are needed.
REFERENCES
Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Can Med Assoc J. 2005;173(5):510–5.
Boockvar KS, Liu S, Goldstein N, Nebeker J, Siu A, Fried T. Prescribing discrepancies likely to cause adverse drug events after patient transfer. Qual Saf Health Care. 2009;18(1):32–6.
Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–9.
Wong JD, Bajcar JM, Wong GG, et al. Medication reconciliation at hospital discharge: evaluating discrepancies. Ann Pharmacother. 2008;42(10):1373–9.
Rogers G, Alper E, Brunelle D, et al. Reconciling medications at admission: safe practice recommendations and implementation strategies. Jt Comm J Qual Patient Saf. 2006;32(1):37–50.
Commission J. Approved: 2010 National Patient Safety Goals. Joint Commission Perspectives. 2009;29(10):1–31.
Girard TD, Jackson JC, Pandharipande PP, et al. Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit Care Med. 2010;38(7):1513–20.
Institute for Healthcare Improvement. Medication reconciliation review. 2007. (Accessed January 19, 2012, at http://www.ihi.org/knowledge/Pages/Tools/MedicationReconciliationReview.aspx.)
Marvanova M, Roumie CL, Eden SK, Cawthon C, Schnipper JL, Kripalani S. Health literacy and medication understanding among hospitalized adults. Journal of Hospital Medicine (accepted) 2011.
Murphy CR, Corbett CL, Setter SM, Dupler A. Exploring the concept of medication discrepancy within the context of patient safety to improve population health. ANS Adv Nurs Sci. 2009;32(4):338–50.
Climente-Marti M, Garcia-Manon ER, Artero-Mora A, Jimenez-Torres NV. Potential risk of medication discrepancies and reconciliation errors at admission and discharge from an inpatient medical service. Ann Pharmacother. 2010;44(11):1747–54.
Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–22.
Moore C, Wisnivesky J, Williams S, McGinn T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;186:46–51.
Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25(5):441–7.
Unroe KT, Pfeiffenberger T, Riegelhaupt S, Jastrzembski J, Lokhnygina Y, Colon-Emeric C. Inpatient medication reconciliation at admission and discharge: A retrospective cohort study of age and other risk factors for medication discrepancies. Am J Geriatr Pharmacother. 2010;8(2):115–26.
Schnipper JL, Roumie CL, Cawthon C, et al. The rationale and design of the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL–CVD) study. Circulation: Cardiovascular Quality & Outcomes 2010;3212–9.
Borson S, Scanlan JM, Watanabe J, Tu SP, Lessig M. Simplifying detection of cognitive impairment: comparison of the Mini-Cog and Mini-Mental State Examination in a multiethnic sample. J Am Geriatr Soc. 2005;53(5):871–4.
Borson S, Scanlan JM, Chen P, Ganguli M. The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc. 2003;51(10):1451–4.
Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive 'vital signs' measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry. 2000;15(11):1021–7.
Baker DW, Williams MV, Parker RM, Gazmararian JA, Nurss JR. Development of a brief test to measure functional health literacy. Patient Educ Couns. 1999;38:33–42.
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74.
Lessard S, DeYoung J, Vazzana N. Medication discrepancies affecting senior patients at hospital admission. Am J Health Syst Pharm. 2006;63(8):740–3.
Vira T, Colquhoun M, Etchells E. Reconcilable differences: correcting medication errors at hospital admission and discharge. Qual Saf Health Care. 2006;15(2):122–6.
Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C, Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health Syst Pharm. 2004;61(16):1689–95.
Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C, Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health Syst Pharm. 2004;61(16):1689–95.
Herrero-Herrero JI, Garcia-Aparicio J. Medication discrepancies at discharge from an internal medicine service. Eur J Intern Med. 2011;22(1):43–8.
Cumbler E, Carter J, Kutner J. Failure at the transition of care: challenges in the discharge of the vulnerable elderly patient. J Hosp Med. 2008;3(4):349–52.
Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549–55.
Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital Readmission in General Medicine Patients: A Prediction Model. J Gen Intern Med. 2010;25:211–219
Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–87.
Walker PC, Bernstein SJ, Jones JN, et al. Impact of a pharmacist-facilitated hospital discharge program: a quasi-experimental study. Arch Intern Med. 2009;169(21):2003–10.
Coleman EA, Parry C, Chalmers S, Min S. The Care Transitions Intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–8.
Project BOOST. Society of Hospital Medicine, 2009. (Accessed March 30, 2011, at http://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&TEMPLATE=/CM/HTMLDisplay.cfm&CONTENTID=27659.)
Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16):1842–7.
Poon EG, Blumenfeld B, Hamann C, et al. Design and implementation of an application and associated services to support interdisciplinary medication reconciliation efforts at an integrated healthcare delivery network. J Am Med Inform Assoc. 2006;13(6):581–92.
Acknowledgments
We thank CL Leak, A Munjal, E Swain, KJ Niesner, and C Bass. Grant support: National Heart, Lung and Blood Institute R01 HL089755 to Drs. Kripalani and Schnipper. The funding agency was not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Dr. Salanitro had full access to all study data and takes responsibility for data integrity and data analysis accuracy. Presented at the Society of General Internal Medicine 34th Annual Meeting in Phoenix, May 6, 2011.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Dr. Kripalani is a consultant to and holds equity in PictureRx, LLC.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Salanitro, A.H., Osborn, C.Y., Schnipper, J.L. et al. Effect of Patient- and Medication-Related Factors on Inpatient Medication Reconciliation Errors. J GEN INTERN MED 27, 924–932 (2012). https://doi.org/10.1007/s11606-012-2003-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-012-2003-y