
Abstract
OBJECTIVE
To determine if the combined effects of patient-level (demographic and clinical characteristics) and organizational-level (structure and strategies to improve access) factors are uniformly associated with utilization of Indian Health Service (IHS) and/or Veterans Health Administration (VHA) by American Indian and Alaska Native (AIAN) Veterans to inform policy which promotes dual use.
METHODS
We estimated correlates and compared two separate multilevel logistic regression models of VHA-IHS dual versus IHS-only and VHA-IHS dual versus VHA-only in a sample of 18,892 AIAN Veterans receiving care at 201 VHA and IHS facilities during FY02 and FY03. Demographic, diagnostic, eligibility, and utilization data were drawn from administrative records. A survey of VHA and IHS facilities defined availability of services and strategies to enhance access to healthcare for AIAN Veterans.
RESULTS
Facility level strategies that are generally associated with enhancing access to healthcare (e.g., population-based services and programs, transportation or co-location) were not significant factors associated with dual use. In both models the common variable of dual use was related to medical need, defined as the number of diagnoses per patient. Other significant demographic, medical need and organizational factors operated in opposing manners. For instance, age increased the likelihood of dual use versus IHS-only but decreased the likelihood of dual use versus VHA-only.
CONCLUSIONS
Efforts to enhance access through population-based and consumer-driven strategies may add value but be less important to utilization than availability of healthcare resources needed by this population. Sharing health records and co-management strategies would improve quality of care while policies allow and promote dual use.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
Increasing access to healthcare resources for eligible American Indian and Alaska Native (AIAN) Veterans is one goal of a Memoranda of Understanding between the Veterans Health Administration (VHA) and the Indian Health Service (IHS) executed in 2003 and in 2010. Some AIAN Veterans are eligible for healthcare from both of these federal healthcare organizations and 26% of these Veterans are dual users of these organizations.1 Since the original Memorandum of Understanding, 30% of facilities across both organizations increased targeted services and focused clinics for this population.2 Dual use has been described as the result of either patient level factors (e.g., health-seeking strategy to improve access, dissatisfaction or preference, knowledge) or organization-level factors (e.g., reducing resource outflow, lack of resources, service strategies to improve utilization), yet neither level of factors fully accounts for utilization.3–8 The purpose of this report is to determine if the combined effect of patient-level and organization-level factors predict dual use uniformly in comparison to either VHA or IHS. Our aim is to inform policy and practices as the VHA and IHS move forward with organizational strategies to improve access, which incidentally promote dual use.
BACKGROUND
VHA and IHS have developed exemplary organizations,9–11 which differ in eligibility, benefits, and resources. VHA, a branch of the Department of Veterans Affairs (VA), provides basic healthcare to all eligible veterans based on need and income; Service connected injuries or illnesses (SCII) determines priority and out-of-pocket costs for limited types of care as well as an amount of monthly monetary compensation for all injured veterans.12 For fiscal planning purposes, the Veterans Equitable Resource Allocation (VERA) also encourages equitable access by accounting for the complexity of veteran’s medical needs in allocating resources to support continuing, on-going medical care. IHS, an agency within the Department of Health and Human Services (DHHS), is responsible for providing federal health services to federally recognized AIAN Tribes, either directly or through Tribal health programs, in the 35 reservation states.13 IHS provides for direct services at no charge to eligible individuals but medical care that is purchased from outside of the IHS or the Tribal health program is subject to a variety of limitations.
At the organizational-level, dual use for IHS-eligible populations has been driven by limited IHS resources.5,14 IHS healthcare providers and managers sometimes encouraged dual use by recommending that Veterans use their VHA benefits for medical services that were not immediately available through IHS,15 particularly for post traumatic stress syndrome (PTSD).2
We surveyed a sample of 227 VHA and IHS facilities and found that 30% had developed population-based, focused services targeting the AIAN Veteran population.2 These services included special health programs (e.g., counseling for AIAN Veterans), enhanced access options (e.g., transportation, telehealth) and formal agreements to provide care to mutually eligible patients (e.g., specialty consultation, pharmaceutical dispensing). Facility-level enhancements also included culturally appropriate services (e.g., Native health modalities).
At the patient-level, individual circumstances may favor use of VHA, IHS or both organizations. Administrative records documented that about one-quarter of IHS-enrolled veterans also used VHA, mainly for behavioral/mental health clinics and laboratory or diagnostic testing.1,16 Patients’ decisions of which organization(s) to use depended on many factors, including convenience, preference for treatments and perceptions of cultural competency, quality of care, professionalism and availability of services, as well as referrals from healthcare providers.6,7
Unlike past studies, this report examines the relationship between these multiple patient and organizational factors in driving utilization patterns. These organizational factors include the structure of the healthcare systems and local facilities as well as innovations in access that promote “ease and opportunity”17 for healthcare interactions with this population. The latter include local strategies that are in place at the facility-level to improve geographic access through consumer-based enhancements (e.g., transportation or co-location of clinics) or cultural access through clinics with enhanced linguistic and cultural competencies, as well as structural factors that may impact access or utilization.
METHODS
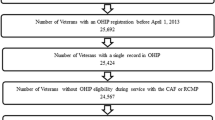
We used multilevel logistic regression modeling of patient and organizational factors to examine dual use versus use of a single organization (i.e., VHA-only or IHS-only), as shown in Figure 1. Our analytic goal was to examine the performance of the same variables in AIAN Veteran populations. Therefore, two separate multilevel models were estimated on a population of VHA-IHS dual versus VHA-only and on a population of VHA-IHS dual versus IHS-only to precisely account for the influence of unique factors which may influence use of healthcare services but that only apply in VHA (e.g., SCII rating) or that only apply in IHS (e.g., administrative management), respectively. These models were compared with respect to their predictive utility.

Multi-level model of dual use of VHA and IHS.
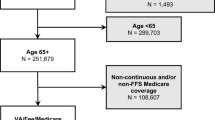
Four data sources were used in this study. We linked and merged patient data in administrative records from 1) IHS National Patient Information Reporting System (NPIRS), 2) VHA National Patient Care Database (NPCD) and 3) VHA-VERA files with 4) our survey of VHA and IHS facilities. The administrative records of patient encounters and registry information resulted in a unique dataset of 64,746 IHS AIAN Veterans who used VHA and/or IHS during fiscal years 2002 and 2003.1 We surveyed all medical center directors at VHA and IHS facilities in a sample of US states in the Pacific Northwest, Pacific Coast, Northern Plains and Southern Plains that met sampling criteria of a high proportion of AIAN Veterans: at least two VHA and two IHS facilities, both IHS management configurations (i.e., direct and Tribal) and both IHS resource configurations (i.e., states with and without IHS hospitals) were included in the sample.2 With a response rate of 68% in the nine-state sample area (Arizona, California, Minnesota, Montana, New Mexico, Oklahoma, South Dakota, Washington, and Wyoming), the survey documented the presence of local targeted services, programs, and interagency strategies to enhance access for AIAN Veterans in 114 VHA and 113 IHS facilities. The survey collected information on organizational complexity and on programs, services and joint local initiatives that focused on healthcare for AIAN Veterans. For this analysis, we retained 201 facilities from the survey sample that had at least two dual users, resulting in an average cluster size of 93.99 AIAN Veterans (range: 2 to 1277 patients) and the patient records for the 18,892 AIAN Veterans who received healthcare from these facilities.
Measures: Patient-Level
Patient-level factors were selected from administrative records representing demographic and clinical characteristics, which typically have been used in utilization studies of this population,14 and are based on the Anderson–Aday framework.18 We aggregated data for nine characteristics over the 2-year study period: Age, sex, residential location, total number of diagnoses, use of medical specialist, use of mental/behavioral health specialist, hospitalization, priority for VHA care and complexity of healthcare. The demographic characteristics included age, sex, residential location in a metropolitan, metro-adjacent or rural county using the 2003 US Office of Management and Budget definitions18 and priority for VHA healthcare services based a SCII rating of ≥50% (no equivalent in IHS) Individuals’ clinical characteristics were the total number of unique, unduplicated outpatient diagnoses as determined by healthcare professionals and recorded as International Classification of Diseases (ICD-9) codes, use of intensive outpatient resources as defined by an encounter in a medical specialty and/or a behavioral or mental health clinic, discharge from a short-stay hospital, and VHA-VERA determination of need for complex and on-going medical care (no equivalent in IHS).
Measures: Organization-Level
For each patient, the relevant organizational factors were determined by the facility that was his/her most frequent source of healthcare. The organizational structures and strategies to improve access for AIAN Veterans at those facilities were described using administrative and survey data. Using administrative data, we characterized organizational characteristics by: 1) type of facility (i.e., medical center or ambulatory care center), 2) IHS Management (i.e., Tribe or federal direct; no equivalent in VHA), 3) characteristic of county in which facility was located19 and 4) location of facility in a state with or without an IHS hospital (no equivalent in VHA). A 5th organizational variable was derived from administrative records to determine the total number of AIAN Veterans that used each facility. We described organizational complexity along six dimensions based on survey responses to: Number of board certified specialties on staff, Gaps in staffing these specialties, Ancillary health programs (i.e., post acute rehabilitation, stroke rehabilitation, comprehensive geriatrics evaluation), On-site treatment programs for PTSD and for alcohol and substance abuse treatment programs and VHA-IHS local agreements to improve healthcare access or share resources.
Strategies to improve access for AIAN Veterans were also documented on the survey. We grouped these strategies into five categories, each of which were treated as a binary variables to characterize facilities: 1) targeted clinics or staffing (i.e., health or mental health clinics that designated space, clinics or specially-trained staff to direct care specifically to AIAN Veterans), 2) educational outreach (i.e., participation in local events, attendance at community forums, and distribution of enrollment and other informational materials), 3) educational programs for VHA/IHS staff on benefit, eligibility and services, 4) strategies to enhance access (i.e., transportation between VHA and IHS facilities, telemedicine, co-management of patients, co-location of services, sharing staff salaries and giving clinical staff privileges to practice at both VHA and IHS) and 5) cultural and linguistic competencies (i.e., health needs assessment, advisory group, native health modalities, required staff training, displays of material culture, targeted health education programs
The analysis was conducted using Stata version 10.0 with the xtmelogit command. We selected a logistic model for the binary outcome (i.e., dual use versus single organization), and a multilevel model to include both patient (level 1) and organization (level 2) variables in the same model. In these models the intercept was specified as random and all explanatory variables were fixed. The 25 patient-level and organization-level variables were tested in both backward and forward selection procedures in order to arrive at a final set of indicators. Both selection procedures yielded the same set of potential explanatory variables: all patient-level variables were retained but only 10 of the organization-level variables, as shown in boldface font in Figure 1.
RESULTS
Dual users comprised 28.8% of the sample; the remaining single users were evenly divided between VHA and IHS as shown in Table 1. Most AIAN Veterans in this sample were men and most were middle-aged or older. The distribution of county of residence characteristics was U-shaped; about half the population resided in metropolitan-adjacent counties and we selected that characteristic as the referent for the logistic analyses. While most Veterans did not receive care in medical specialty, behavioral/mental health or hospital services, a consistent pattern emerged that greater proportions of dual users and IHS-only users received these types of care. For instance, among VHA-only users, 8.1% received care in a behavioral/mental health clinic and 24.1% in a hospital in comparison to dual users (27.1% and 41.6%) and IHS-only users (26.9% and 48.2%), respectively. Like the general VHA-only user population, about 4% of these AIAN Veterans who were enrolled for care at VHA had been rated with complex healthcare needs; there is no equivalent rating system in IHS administrative data for comparison. About 40% of AIAN Veterans who received any care at VHA facility had high eligibility ratings with SCII of ≥50%.
At the organization-level, the sample was almost evenly divided between VHA facilities (103) and IHS facilities (98). As shown in Table 2, the majority of VHA and IHS facilities were ambulatory care centers with few medical subspecialty services on site; of facilities that did have subspecialty services, about the same proportion in each organization had a gap in staffing these subspecialists. Substance abuse and healthcare services targeted to AIAN Veterans were equally distributed across the VHA and IHS facilities but availability of other special programs varied across organizations. More PTSD programs and ancillary medical care were located at VHA facilities and more programs to enhance access were located at IHS facilities. The majority (68.4%) of IHS facilities in this sample were administered by Tribes.
Table 3 shows the results of the two multi-level models. At the patient-level in model 1 (VHA-only use versus dual use), the odds of being a dual user were significantly greater for those who lived in rural areas in comparison to metro-adjacent (OR = 0.53) and for those who had increasing numbers of unique medical diagnoses. The odds of being a dual user as compared to VHA-only user were significantly lower for AIAN who were middle-aged or older than for those aged ≤44 years, for those living in a metropolitan county than in a metro-adjacent county, for those who had received care in a specialty and behavioral clinic or at a short stay hospital in comparison to those who had not received those types of care, and for those rated with higher levels of service connected injury or illness. At the organization-level, for every unit increase in board certified subspecialty departments on staff, the odds of being a dual user were lower (OR = 0.78).
At the patient-level in model 2 (IHS-only versus dual use), the odds of being a dual user as compared to IHS-only user were significantly greater for AIAN elders than for those aged 44 and younger (OR = 1.52), for those who lived in metropolitan rather than metro-adjacent areas, for those who had received care in a specialty and behavioral clinic or at a hospital in comparison to those who had not received those types of care, for those who had increasing numbers of unique medical diagnoses. At the organization-level, the odds of being a dual user were significantly greater when the usual source of care had an increasing number of board certified subspecialty departments on staff (OR = 2.99).
The models represent different samples (i.e., dual use versus VHA-only use; dual use versus IHS-only use) with similar but not identical outcomes. The similarities and differences between these two models were notable. In both models, a greater number of unique diagnoses were a significant explanatory variable of dual use. Other significant variables exhibit an opposite effect in the single use models. For instance, older age, use of intensive medical care services and increasing number of board certified subspecialty departments on staff were positively related to dual use in comparison to IHS-only use but not to the comparison with VHA-only. The impact of the residential county varied across the two models. In model 1, the odds of dual use were higher among rural county residents and lower among metropolitan county residents, while the characteristics of the county of residence was not a significant indicator in model 2. Only one organization variable remained in the final models: the number of medical subspecialties on-site at the home facility. This indicator also had opposite effects across the two models. In model 2, the odds of dual use increased by a factor of 2.99 for each additional specialty at the usual source of care, while in model 1 the odds decreased by factor of 0.78.
DISCUSSION
Unlike previous studies of dual use, our multilevel approach allowed us to explore the effects of patient and organizational factors. Our two models shared several significant explanatory variables of dual use; however, some explanatory variables operated in an opposing manner. These contradictory results suggest a temporal element. The IHS, which may have cared for these veterans since their childhoods, may have been the primary provider until the need for specialized or intensive healthcare services resulted in dual use. It appeared that once a Veteran had enrolled in the VHA system, these health factors were no longer related to dual use as the Veteran may transition to exclusive use of VHA. This scenario may reflect relative differences in 1) resources to care for the aged, very ill, and multiple complex conditions, 2) greater availability and/or lower cost of services for veterans with higher SCII ratings or 3) impact of financial compensation for SCII. It may also arise from the lack of clinical coordination between these organizations, leading to a scheduling of all follow-up visits within the VHA instead of managing follow-up in the IHS primary care setting. Dual use might also be a temporary phenomenon that is related to a specific episode of care. Our interpretations are limited by the cross-sectional nature of our data and future research should examine the temporal and longitudinal nature of dual use, as well as patterns of care for specific medical conditions. Future research might also investigate factors, which were beyond the scope of this project (e.g., Tribal membership at the IHS point of care) that may influence exclusive use of VHA versus IHS.
We developed two models to account for unique factors in VHA and IHS that prior studies suggested might influence dual use. Patient and organizational factors performed differently across these models. These contradictory models also suggest that expectations about the same dual user population may differ, potentially affecting planning efforts to enhance access as set forth in the Memorandum of Understanding. While it is a logical assumption, given the organizational differences in funding and expertise, that medical needs (old age, use of intensive resources, visits to facilities staffed with subspecialty services) predicted dual use in comparison exclusive use of IHS (model 2), these same factors actually reduced the odds of dual use in comparison to exclusive use of VHA (model 1). In other words, increasing access to VHA services for IHS-enrollees may not substantially increase utilization of VHA resources among the most medically needy patients. The actual availability of targeted services or activities to enhance access were not significantly related to utilization patterns. Improving perceived access through population-based and consumer-driven strategies may add value but be less important to actual access than availability of healthcare resources needed by this population. Our models may have been insufficiently sensitive to discern these value-added features.
Our models are subject to the limitations of the data sources, although both VHA and IHS have processes in place to assure accuracy in the medical information.19,20 IHS registry information may undercount the number of Veterans.21 At the patient-level, all medical encounters were aggregated and diagnoses were unduplicated, nevertheless dual users may have has the opportunity to acquire more diagnoses. These encounter data do not include some personal characteristics that may be relevant to current or future utilization patterns or new outreach strategies among veterans (e.g., active duty National Guard or reserve units that were called to combat zones by Presidential order). While it was expected that medical directors or their designed survey respondents would be most familiar with the types of care available at their own facility, respondents may have included recent hires or designees who were less knowledgeable. We are unable to evaluate the quality or variation of the specialized clinics for AIAN Veterans or outreach strategies that were reported through our survey; future research might focus on these organizational factors. Finally, the study population may not adequately represent AIAN Veterans living in the remaining 26 IHS-service states where either IHS or VHA resources may be sparser.
While dual use may extend the range of resources available for this population, it has also lead to unnecessary duplication, treatment conflicts and inefficiencies.15 The need to improve coordination and communications between federal healthcare agencies is well recognized,22 authorized in the recent Memorandum of Understanding and endorsed by VHA and IHS staff.23 Sharing health records and co-management strategies would improve quality of care at the same time as VHA and IHS policies allow and promote dual use. Our models suggest that policy-makers and planners should also recognize that organizations may characterize the same potential population of dual-users differently. For VHA, AIAN dual users appear to be younger and less likely to use intensive healthcare resources than those who use VHA exclusively; for IHS, these dual users are older and more likely to need intensive healthcare resources than those who use IHS exclusively. The current utilization pattern, which has resulted from both patient and organizational factors, suggests that IHS may already be serving a segment of the increasingly younger VHA user-population. Improving healthcare and access for AIAN Veterans should include the recognition that this population may be managed or co-managed over time by three federal healthcare organizations: IHS, Department of Defense and VHA.
REFERENCES
Kramer BJ, Wang M, Jouldjian S, Lee ML, Finke B, Saliba D. Veterans Health Administration and Indian Health Service: Healthcare utilization by Indian Health Service enrollees. Med Care. 2009;47(6):670–6.
Kramer BJ, Jouldjian S, Finke B, Saliba D, Yano EM, Mitchell M, Dang, J. VHA and Indian Health Service: Access for American Indian Veterans: Survey of VHA and IHS Facilities’ Leadership. Sepulveda, CA: VA Greater Los Angeles HSR&D Center of Excellence (Technical Report #VHA-IHS07_002), 2007. Available upon request.
Borowsky SJ, Cowper DC. VA resource allocation based on # of Vets in each VISN. Neither allocation of resources not quality measures account for those Vets who receive care from non-VA. Dual use of VA and non-VA primary care. J Gen Intern Med. 1999;14(5):274–80.
Couper DC, Manheim LM, Weaver FM, Pawlow AJ. Mix and match: VA and non-VA care for elderly veterans. VA Practioner 1993:41–4.
Cunningham PJ, Altman BM. The use of ambulatory health care services by American Indians with disabilities. Med Care. 1993;31:606–16.
Gurley D, Novins DK, Jones MC, et al. Comparative use of biomedical and traditional healing options by American Indian veterans. Psychiatr Serv. 2001;52:68–74.
Harada ND, Villa VM, Reifel N, Bayhylle R. Exploring veteran identity and health services use among Native American veterans. Mil Med. 2005;170:782–6.
Washington DL, Yano EM, Simon B, Sun S. To use or not to use. What influences why women veterans choose VA health care. J Gen Intern Med. 2006;21(Suppl 3):S11–8.
Selim AJ, Kazis LE, Qian S, Rothendler JA, Spiro A 3rd, Rogers W, Haffer SC, Wright SM, Miller D, Selim BJ, Fincke BG. Differences in risk-adjusted mortality between Medicaid-eligible patients enrolled in Medicare advantage plans and those enrolled in the veterans health administration. J Ambul Care Manage. 2009;32(3):232–40.
Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs health care system on the quality of care. N Engl J Med. 2003;348(22):2218–27.
Kunitz SJ. The history and politics of US health care policy for American Indian and Alaska natives. Am J Public Health. 1996;86(10):1464–73.
US Department of Veterans Affairs. Eligibility for health benefits. Available at: http://www.va.gov/healtheligibility/. Accessed May 9, 2011.
US Department of Health and Human Services, Indian Health Service. IHS Fact Sheets. Available at: http://info.ihs.gov/TrblSlfGov.asp. Accessed October 5, 2009.
Cunningham PJ. Access to care in the Indian Health Service. Health Aff. 1993;12:224–33.
Kramer BJ, Vivrette RL, Satter DE, Jouldjian S, McDonald LR. Dual use of Veterans Health Administration and Indian Health Service: healthcare provider and patient perspectives. J Gen Intern Med. 2009;24(6):758–64.
Kramer BJ, Sarkisyan S, Yano E, Washington D, Harker JO. Dual use of VHA and IHS healthcare by women. Women’s Health Issues. 2009;19(2):135–43.
Fortney JC, Booth BM, Bosworth HB, Kaboli P, Burgess J. A re-conceptualization of access for 21st century healthcare. Paper commissioned for the September 2010 VA State of the Art Conference on Access, Arlington, VA.
US Department of Agriculture, Economic Research Service. Measuring Rurality: Rural-Urban continuum codes. Available at: http://www.ers.usda.gov/Briefing/Rurality/RuralUrbCon/. Accessed June 14, 2011.
Ashton CM, Petersen NJ, Wray NP, Yu H. The Veterans Affairs medical care system: Hospital and clinic utilization statistics for 1994. Med Care. 1997;36:793–803.
USDHHS, PHS, Indian Health Service Office of Planning, Evaluation and Legislation, Division of Program Statistics. Regional differences in Indian health. 1993.
Kramer BJ, Wang M, Hoang T, Harker JO, Finke B, Saliba D. Identification of American Indian and Alaska Native Veterans in administrative data of the Veterans Health Administration and the Indian Health Service. Am J Pub Health. 2006;96(9):1577–8.
Institute of Medicine, Committee on Enhancing Healthcare Quality Programs. Leadership by example: Coordinating government roles in improving health care quality. JM Corrigan & BM Smith, Eds, Washington DC: National Academy Press, 2002.
Kramer BJ, Finke B, Saliba D, Jouldjian S, Yano EM. Fostering closer alignment of the Veterans Health Administration and the Indian Health Service. Mil Med. 2010;175(7):463–5.
Acknowledgements
This research was supported by a grant from the VA Health Services Research and Development, ACC 03–304. This report presents findings and conclusions of the authors; it does not necessarily reflect the opinions or policies of the Department of Veterans Affairs or the Indian Health Service. An earlier version of this paper was presented in a paper session at the Gerontological Society of America, annual scientific meetings in New Orleans, November 2010.
Conflict of Interest
None disclosed.
Institutional Review Board
The project was reviewed and approved by the VA Greater Los Angeles Healthcare System Institutional Review Board, the national Indian Health Service and Tribal Institutional Review Boards as required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kramer, B.J., Jouldjian, S., Wang, M. et al. Do Correlates of Dual Use by American Indian and Alaska Native Veterans Operate Uniformly Across the Veterans Health Administration and the Indian Health Service?. J GEN INTERN MED 26 (Suppl 2), 662 (2011). https://doi.org/10.1007/s11606-011-1834-2
Published:
DOI: https://doi.org/10.1007/s11606-011-1834-2