
Abstract
BACKGROUND
Overuse of antibiotics in the treatment of acute respiratory tract infection (ARI) contributes to the growing problem of antibiotic-resistant infections.
OBJECTIVE
To identify factors that influence community practitioners to prescribe antibiotics and examine how they differ from the recommendations of the Centers for Disease Control and Prevention (CDC) guideline for treatment of ARI.
DESIGN
Paper case vignette study using a fractional factorial design.
PARTICIPANTS
One hundred one community practitioners and eight faculty members.
MAIN MEASUREMENTS
We asked community practitioners to estimate how likely they would be to prescribe antibiotics in each of 20 cases of ARI and then used multiple regression to infer the importance weights of each of nine clinical findings. We then compared practitioners’ weights with those of a panel of eight faculty physicians who evaluated the cases following the CDC guidelines rather than their own judgments.
MAIN RESULTS
Practitioners prescribed antibiotics in 44.5% of cases, over twice the percentage treated by the panel using the CDC guidelines (20%). In deciding to prescribe antibiotic treatment, practitioners gave little or no weight to patient factors such as whether the patients wanted antibiotics. Although weighting patterns differed among practitioners, the majority (72%) gave the greatest weight to duration of illness. When illness duration was short, the rate of prescribing (20.1%) was the same as the rate of the faculty panel (20%).
CONCLUSIONS
Based on hypothetical cases of ARI, community practitioners prescribed antibiotics at twice the rate of faculty following CDC practice guidelines. Practitioners were most strongly influenced by duration of illness. The effect of duration was strongest when accompanied by fever or productive cough, suggesting that these situations would be important areas for practitioner education and further clinical studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Overuse of antibiotics in the treatment of acute respiratory tract infection (ARI) contributes to the growing problem of antibiotic-resistant infections. Although antibiotic use for ARIs is slowly declining1, prescription of antibiotics for these predominantly viral infections remains an important public health problem. The reasons for the persistence of this practice are not certain. Antibiotic prescription rates are greater when purulent manifestations of ARI are present2,3. Patient factors, time pressures, and practitioner type and specialty also may be important in the decision4,5.
If we understood better how clinical factors influence practitioners’ decisions to prescribe antibiotics, we could design education strategies to decrease the use of antibiotics in cases where they were not likely to be of any benefit. Thus, we designed paper case vignettes that depicted patients with ARI and asked community practitioners whether they would prescribe antibiotics in each case. We then inferred the importance of each clinical and patient factor from their answers.
We asked the following questions: Which clinical and patient factors were most important to practitioners in deciding to prescribe antibiotics? Were they influenced by patient wishes and patient pressure? Did the importance of clinical and patient factors vary from clinician to clinician? How do the community practitioners’ decisions compare with those that would result from the application of the Centers for Disease Control and Prevention (CDC) guidelines regarding antibiotic treatment of respiratory infections?
METHODS
Paper Cases
To determine the importance of clinical and patient factors, we designed 20 case vignettes describing patients with ARI symptoms. After reading each case, respondents were asked whether or not they would prescribe antibiotics for this patient (yes/no), how likely it was they would prescribe antibiotics (0–100 scale), how comfortable they were with their decision, and how strongly they would urge the patient to take antibiotics if the patient did not want to (0–100 scale). We added these latter questions to explore the effect of uncertainty on and to measure the strength of practitioners’ convictions about the decision. A second set of cases, designed to investigate the differential diagnosis of ARI, was included but is not reported in this paper.
We selected the variables of interest through a review of clinical and patient factors that had proved important in previous studies of ARIs2–4,6–9 as well as results of previous case vignette studies of clinicians’ diagnoses in ARIs10–13. We also included non-clinical patient factors that might affect treatment but not diagnosis, such as patient expectation for antibiotics, or impending travel. Several previous studies suggested these factors influence prescribing decisions4,5,14–16. Each case presented the same variables in either a positive or negative form (e.g., “no cough” or “productive cough with yellow sputum”). The positive levels were chosen by the frequency of values in clinical studies of ARIs, interviews with clinicians to identify important thresholds, and review of the literature. Additionally, we avoided variables and values that would provide strong evidence for a particular diagnosis, such as tonsillar exudate (pharyngitis), pain resembling a maxillary toothache (sinusitis), and positive transillumination (sinusitis) in order to get a broad distribution of likelihood estimates. Variables and levels are shown in Table 1.
To reduce the number of cases each participant had to evaluate, we used a fractional factorial design that presents all important combinations of variables and allows analysis of the main effects and selected first-order interactions in 20 cases rather than the 512 that would be required for a full factorial17.
Participants
We recruited 101 primary care practitioners in 2001–2002 from community practices in Colorado as part of the Minimizing Antibiotic Resistance in Colorado (MARC) Project (AHRQ R01 HS13001–01), a study testing different types of community educational campaigns to improve appropriate antibiotic use for ARIs18. Each practitioner reviewed all 20 cases. Practitioners who were in a predominantly pediatric practice received a version of the case vignettes with minor changes in wording to depict an adolescent rather than adult patient.
To provide a reference standard, we asked eight general internist faculty members at the University of Nebraska College of Medicine and at the University of California San Francisco to review each of the 20 cases with specific instructions to apply the CDC Principles of Appropriate Antibiotic Use for Adults with ARIs19–21. These guidelines were developed by a panel appointed by the CDC and were endorsed by the CDC, the American College of Physicians, the American Academy of Family Practice, and the Infectious Disease Society of America. The faculty members were each given the guidelines to study and were asked to answer the cases using the CDC guidelines. They were told not to use their own judgment or clinical practice, but to answer the questions regarding antibiotics as they would be answered according to the guidelines. For each case the faculty members were asked to answer four multiple choice questions according to the CDC guidelines: Should this patient be given antibiotics? Is the cause viral or bacterial? What is the most likely diagnosis? How confident are you in the diagnosis?
Analysis
We used the statistical programs of SAS to analyze the responses (SAS Institute, Inc. version v9.1 Cary, NC). First, we analyzed all responses at the level of the individual practitioner, then averaged all practitioner averages to obtain the overall average. We calculated the weights for each of the 101 practitioners using the method of judgment analysis22,23. A participant did not explicitly say whether they were influenced by a variable. Rather, we constructed a linear model for each practitioner using regression analysis to infer the weight of each variable from the judgment made about each case (the likelihood they would prescribe antibiotics). Where the outcome variable was continuous (e.g., likelihood), we used multivariate linear regression; where it was a yes/no question, we used logistic regression. We calculated weights similarly for the eight faculty using the CDC guidelines. In judgment analysis it is important to obtain the results at the level of the individual practitioner first and then combine the results in order to avoid missing individual variation. To confirm that the linear model was the best fit, we ran repeated monotonic transformations of the dependent variables using the variance explained (r2) as the test for fit.
RESULTS
Of the 101 practitioners from community practices in Denver and Colorado Springs, 30 were pediatric practitioners and 71 cared for adults and families. Of the 101, 35 were women and 66 were men. There were 58 physicians, 18 physician assistants, and 23 nurse practitioners. Twenty-three practiced in an internal medicine practice, 40 in family practice, 30 in pediatrics, and 7 in “other.” The average likelihood of prescribing an antibiotic was 43.6 (CI: 37.1–50.1) with considerable variability by the practitioner (median = 40, interquartile range = 10–77.5). Practitioners said they would prescribe an antibiotic (yes/no) in 44.5% of cases. The average rating (0–100) for being comfortable with the decision was 78.1 (CI: 74.4–81.8), and the average rating of “How strongly would you urge the patient to start antibiotics?” (0–100) was 24.1 (CI: 18.6–29.6).
Weighting of Clinical and Patient Variables by Individual Practitioners
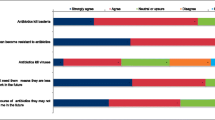
Figure 1 shows the average weight for each of the nine variables. Overall, practitioners gave the most weight to the duration of the illness. The next four variables had similar weights: sinus pressure and pain, temperature of 101.5° F (versus 99° F), productive cough with yellow sputum (versus none), and colored nasal drainage (versus no nasal drainage). None of the patient factors (expectation of antibiotics, pending trip or previous good results from antibiotics in a similar illness) had any appreciable influence on the decision.

Median of weights for each of the nine variables in deciding whether to prescribe antibiotics by 101 community practitioners.* All weights are given as the change in likelihood associated with the factor going from being absent to being present as defined in Table 1.
The r2 of the linear model derived from the practitioners’ answers indicates how much variation in the judgments is explained by the judgment policy, i.e., how well the model fits the actual judgments made. The median r2 for the 101 practitioners was 0.82 (25th, 75th percentile = 0.74, 0.87) a high degree of fit. With the first order interactions included, the r2 increases to 0.86.
Variation Among Individual Practitioners
Practitioners varied considerably in both the patterns of weights of the clinical or patient factors and the range of weights for each individual factor. The weight given to productive cough as a percent of total weight, for example, varied from −18.6 to 68.7 with a median of 11.4. There was good agreement, however, among individual practitioners regarding which variable had the greatest weight. Duration of illness was the most important variable for 72% of the practitioners followed by temperature (13%), sinus symptoms (6%), nasal drainage (6%), and productive cough (3%) (Table 2). This pattern was similar across specialties. Weights calculated using the yes/no outcome were nearly identical.
Most practitioners (78.1%) were comfortable with their treatment decisions. Comfort with the decision was inversely correlated with the likelihood of giving antibiotics (r = −0.22, p < 0.0001), but was not correlated with other clinical or patient factors.
CDC Guidelines
The eight faculty members asked to follow the CDC guidelines gave antibiotics in 20% of the cases, compared to 44.5% for the practitioners (p < 0.0001). They thought the cause was bacterial in 19.4% of cases. The findings weighted most heavily were duration of illness (four faculty members), sinus pressure (three faculty members), and nasal drainage (one faculty member). Average weights for the clinical and patient variables were similar to those of the community practitioners except that the average weight for productive cough was negative (against prescribing): −3.9 (CI: −11.7 to 3.8) compared with the community practitioners whose average weight for productive cough was 12.4 (CI: 10.0 to 14.8). Several faculty commented that their answers following the guidelines differed from how they would have answered if they had been following their own practice policies.
Interactions Among Variables
To determine if the weighting of any variable was influenced by the state of other variables, we calculated the first order interactions. Overall, four interactions were significant: cough × duration, cough × temperature, sinus pressure × duration, and temperature × duration all had greater weight when both were present (positive) than would have been predicted from their individual weights. When we calculated the weights for each of the 101 individuals, the interactions of sinus pressure × duration and temperature × duration replaced duration alone as the highest weighted variable for 24 practitioners. The interaction of cough × duration was the highest weighted variable for six practitioners. As an example of the effect, antibiotics were prescribed 52% of the time when cough was present, but 37% of the time when it was absent. When cough was absent and duration was long, practitioners prescribed antibiotics in 27.1% of cases, but when cough was present and duration was long, they prescribed antibiotics in 78.8% of cases. Overall, there were no significant interactions between cough and duration in the cases from the faculty members following the CDC guidelines, but there were strong interactions between temperature and duration and sinus pressure and duration.
DISCUSSION
In order to understand how clinical factors influence practitioners’ decisions about prescribing antibiotics in ARIs, we studied the decisions of 101 community practitioners in response to 20 case vignettes of patients with respiratory tract infection. On average, they prescribed antibiotics in 44.5% of the cases. Although the weighting of specific findings varied from individual to individual, 72% of practitioners placed the greatest weight on the duration of illness in making the decision to start antibiotics. In addition, there were significant interactions between the most important clinical factors. Non-clinical patient factors such as the patient’s desire for antibiotics did not play a significant role in the decisions, although many physicians say they are influenced by patient factors in antibiotic treatment decisions for ARIs4,5,14–16.
To provide a benchmark, eight internal medicine faculty members reviewed the published guidelines from a CDC expert panel before deciding whether to prescribe antibiotics in the same 20 cases. They prescribed antibiotics in 20% of the cases and thought that 19.4% of the cases were bacterial in nature. Four of the panelists placed the greatest weight on duration of illness, three on sinus pressure and pain, and one on colored nasal drainage.
These results suggest that duration of illness plays a major role in the decision to prescribe antibiotics. Duration of illness has not received much attention previously. Dosh and colleagues had found that duration greater than 14 days was associated with increased prescribing in their univariate analysis, but the effect disappeared when the model was adjusted for other variables9. Does longer duration increase the likelihood that the illness is bacterial? In these 20 cases, the possible diagnoses included viral URI, influenza, bronchitis, rhinosinusitis, or pneumonia. Of these, only sinusitis and pneumonia would be treated with antibiotics according to the CDC guidelines20,21. Pharyngitis was not a consideration in these cases because none had a sore throat. Because there is evidence that rhinosinusitis of longer duration is more likely to be a bacterial infection21, it is reasonable to consider duration of illness in that setting. Routine antibiotic treatment of uncomplicated acute bronchitis, however, is not recommended in healthy individuals, regardless of the duration of the illness19. The median duration of viral bronchitis is 2 to 3 weeks, and longer duration does not correlate with a bacterial cause, with the notable exception of pertussis in patients with cough lasting more than 2–3 weeks24. With regard to pneumonia, a study of 1,436 patients with respiratory tract infection seen in the emergency department found that duration of illness was not an independent predictor of infiltrate on chest X-ray25, and it was not an important factor in the diagnosis of pneumonia in the studies reviewed by Metlay26.
Other findings given significant weight by the community practitioners were temperature, sinus tenderness, colored nasal drainage, and productive cough. In these case vignettes, the level of fever (101.5° F) does not reliably distinguish between viral and bacterial infections, but is a predictor of pulmonary infiltrate if pneumonia is under consideration25. Colored nasal drainage, but not sinus pressure and pain, is helpful in distinguishing bacterial from viral rhinosinusitis7. Productive cough usually suggests bronchitis unless a patient also presents with marked sinus congestion, but cough did not achieve significance as an independent predictor of pneumonia in two studies25,27. Gonzales found that findings suggesting purulence are associated with increased rates of antibiotic use2. Purulence, however, has not proved to be a reliable way to distinguish bacterial from viral bronchitis28,29. None of the three patient factors appeared to influence the decisions. Several studies have suggested that patient factors are important4,5,13–15, but an observational study of 482 patients found no independent effect on prescribing decisions9. There are several possible explanations for these differences. Since most studies of patient factors rely on physicians’ self-report of what influenced their decision, it may be that practitioners overestimate the effect of patient factors or may use them to rationalize a decision to prescribe. Previous studies have shown that decision makers often have poor insight into their own decision policies and that the weights derived from judgment analysis are better at predicting future decisions30. An alternative explanation is that patient factors are indeed important, but that the written descriptions of the patients’ wishes in this study did not have the impact of a face-to-face presentation and thus underestimated the effect.
Most of the practitioners were more comfortable with their decisions in the cases where they did not give antibiotics. The study cases were designed to have few clear-cut diagnoses, and it may be that the cases in which respondents prescribed antibiotics were those with more uncertainty about the diagnosis. Alternatively, practitioners may have been more concerned about error when giving antibiotics than when omitting them. A critical incident study of British practitioners found that the clinical situation that most frequently made them uncomfortable was deciding whether to prescribe antibiotics in respiratory tract conditions31.
What accounted for the lower antibiotic prescribing rate among the faculty applying the CDC guidelines (20% versus 44.5%)? The lower rate in the faculty could have been due to differences in the overall proportion of cases they thought should get antibiotics (the base rate). The general tone of the published CDC guidelines is that most respiratory tract infections are viral and do not need antibiotics. Additionally, the decreased weight given productive cough and the lack of interaction between cough and duration by the faculty members could have accounted for some or all of the lower rate. The CDC guidelines for bronchitis stated, “Routine antibiotic treatment of uncomplicated acute bronchitis is not recommended, regardless of duration of cough”20. The faculty group prescribing was consistent with this. They had a slightly negative weight for productive cough and no interaction between cough and duration.
There are several limitations to generalization of these findings. The decisions were made in response to paper case vignettes limited to nine features and not actual patients. Descriptions of clinical findings and patient factors may have lacked the force they would have in patient encounters. Practice patterns of these Colorado practitioners might not generalize to other geographic areas. Strongly diagnostic findings (e.g., tonsillar exudate, unilateral maxillary pain) were purposely omitted, and this could have increased the overall uncertainty and affected the rate of antibiotic prescribing. Finally, the vignettes did not allow ordering further examinations or tests as might have been appropriate if pneumonia had been suspected.
These results indicate that these practitioners are strongly influenced by the duration of illness in deciding to prescribe antibiotics. The influence of duration of illness is particularly strong in cases where the patient had a productive cough. Omission of this effect would bring the prescription rate close to that of faculty members following the published CDC guidelines. This demonstrates the importance of the weight the clinician gives to individual findings in deciding whether to prescribe antibiotics. It suggests, further, that clinical studies aimed specifically at whether antibiotics are effective in cough illnesses that last 2 weeks or more are particularly important. Targeted education of practitioners about the utility of antibiotics in this specific situation may be of great help in reducing antibiotic use.
References
Roumie CL, Halasa NB, Grijalva CG, Edwards KM, Zhu Y, Dittus RS, Griffin MR. Trends in antibiotic prescribing for adults in the United States-1995 to 2002. J Gen Intern Med. 2005;20:697–702.
Gonzales R, Barrett PH Jr, Crane LA, Steiner JF. Factors associated with antibiotic use for acute bronchitis. J Gen Intern Med. 1998;13(8)541–8. Aug.
Gonzales R, Barrett PH, Steiner JF. The relation between purulent manifestations and antibiotic treatment of upper respiratory tract infections. J Gen Intern Med. 1999;14:151–6.
Macfarlane J, Holmes W, Macfarlane R, Britten N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: questionnaire study. BMJ. 1997;315(7117)1211–4. Nov 8.
Scott JG, Cohen D, DiCicco-Bloom B, Orzano AJ, Jaen CR, Crabtree BF. Antibiotic use in acute respiratory infections and the ways patients pressure physicians for a prescription. J Fam Pract. 2001;50(10)853–8. Oct, Erratum in: J Fam Pract 2001 Dec;50(12):1077.
Steinman MA, Landefeld CS, Gonzales R. Predictors of broad-spectrum antibiotic prescribing for acute respiratory tract infections in adult primary care. JAMA. 2003;289:719–25.
Little DR, Mann PL, Godbout CJ. How family physicians distinguish acute sinusitis from upper respiratory tract infection: a retrospective analysis. J Am Board Fam Pract. 2000;13:101–6.
Williams JW, Simel DL. Does this patient have sinusitis? Diagnosing acute sinusitis by history and physical examination. JAMA. 1993;270:1242–6.
Dosh SA, Hickner JM, Mainous AG, Ebell MH. Predictors of antibiotic prescribing for nonspecific upper respiratory infections, acute bronchitis, and acute sinusitis. An UPRNet study. Upper Peninsula Research Network. J Fam Pract. 2000;49(5)407–14. May.
Sorum PC, Stewart TR, Mullet E, et al. Does choosing a treatment depend on making a diagnosis? US and French physicians’ decision making about acute otitis media. Med Decis Making. 2002;22(5)394–402. Sep-Oct.
Wigton RS, Poses RM, Collins M, Cebul RD. Teaching old dogs new tricks: using cognitive feedback to improve physicians’ diagnostic judgments on simulated cases. Acad Med. 1990;65(9)S5–6.
Gonzalez-Vallejo C, Sorum PC, Stewart TR, Chessare JB, Mumpower JL. Physicians’ diagnostic judgments and treatment decisions for acute otitis media in children. Med Decis. 12.
Murray S, Del Mar C, O’Rourke P. Predictors of an antibiotic prescription by GP’s for respiratory tract infections: a pilot. Fam Pract. 2000;17:386–8.
Linder JA, Singer DE. Desire for antibiotics and antibiotic prescribing for adults with upper respiratory tract infections. J Gen Intern Med. 2003;18(10)795–801. Oct.
Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N. Understanding the culture of prescribing: qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ. 1998;317(7159)637–42. Sep 5.
Avorn J, Soumerai SB. Improving drug-therapy decisions through educational outreach. A randomized controlled trial of academically based “detailing”. N Engl J Med. 1983;308:1457–63.
Plackett RL, Burman JP. The design of optimum multifactorial experiments. Biometrika. 1946;33:305–25.
Gonzales R, Corbett KK, Leeman-Castillo BA, et al. The “minimizing antibiotic resistance in Colorado” project: impact of patient education in improving antibiotic use in private office practices. Health Serv Res. 2005;40(1)101–16. Feb.
Gonzales R, Bartlett JG, Besser RE, et al. Principles of appropriate antibiotic use for treatment of acute respiratory tract infections in adults: background, specific aims, and methods. Ann Intern Med. 2001;134(6)479–86. Mar 20.
Gonzales R, Bartlett JG, Besser RE, et al. Principles of appropriate antibiotic use for treatment of uncomplicated acute bronchitis: background. Ann Intern Med. 2001;134(6)521–9. Mar 20.
Hickner JM, Bartlett JG, Besser RE, et al. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001;134(6)498–505. Mar 20.
Cooksey RW. Judgment Analysis: Theory, Methods, and Applications. Academic Press; 1996.
Wigton RS. Use of linear models to analyze physicians’ decisions. Journal of Medical Decision Making. 1988;8:241–52.
Ward JI, Cherry JD, Chang SJ, et al. Efficacy of an acellular pertussis vaccine among adolescents and adults. N Engl J Med. 2005;353(15)1555–63. Oct 13.
Heckerling PS, Tape TG, Wigton RS, et al. Clinical prediction rule for pulmonary infiltrates. Ann Intern Med. 1990;113:664–70.
Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997;278(17)1440–5. Nov 5.
Diehr P, Wood RW, Bushyhead J, Krueger L, Wolcott B, Tompkins RK. Prediction of pneumonia in outpatients with acute cough-a statistical approach. J Chronic Dis. 1984;37(3)215–25.
Wenzel RP, Fowler AA. Clinical practice. Acute bronchitis. N Engl J Med. 2006;355(20)2125–30. 16.
Braman SS. Chronic cough due to chronic bronchitis: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 Suppl)104S–15S.
Kirwan JR, Chaput de Saintonge DM, Joyce CRB, Holmes J, Currey HLF. Inability of rheumatologists to describe their true policies for assessing rheumatoid arthritis. Ann Rheum Dis. 1986;45:156–61.
Bradley CP. Uncomfortable prescribing decisions: a critical incident study. BMJ. 1992;304(6822)294–6. PMID: 1739831, Feb 1.
Acknowledgments
Parts of this study were presented at the 2002 Annual Meeting of the Society of General Internal Medicine.
The study was funded through grants and contracts from the Agency for Health Care Research and Quality. Minimizing Antibiotic Resistance in Colorado (MARC) Project (AHRQ R01 HS13001–01), a study testing different types of community educational campaigns to improve appropriate antibiotic use for ARIs18.
The funding source had no role in the design, conduct, and analysis of the study or in the decision to submit the manuscript for publication. Drs. Gonzales, Darr, Corbett, and Nickol had full access to the data.
The authors would like to thank Thomas Tape, MD, for his review and comments on this manuscript.
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Sample Case
This patient has the following history:
-
colored nasal drainage
-
no cough
-
no sinus symptoms
-
The patient has had this illness for 14 days
-
Feels this illness is so severe that treatment is needed
Examination:
-
temperature = 99° F
The patient has come in specifically to get antibiotic treatment
Patient is leaving on vacation soon and worries about the illness getting worse
No prior antibiotics for this sort of illness
-
1.
Mark an “x” on the line below to indicate how likely you are to prescribe an antibiotic in this case

-
2.
In your practice, would you prescribe an antibiotic for this patient? (Circle one) Yes No
-
3.
Mark an “x” on the line to indicate how comfortable you are with your decision about antibiotics?

-
4.
Imagine this same patient does not want to take antibiotics: Mark an “x” on the line to indicate how strongly you would urge the patient to start antibiotics right away.




Rights and permissions
About this article
Cite this article
Wigton, R.S., Darr, C.A., Corbett, K.K. et al. How Do Community Practitioners Decide Whether to Prescribe Antibiotics for Acute Respiratory Tract Infections?. J GEN INTERN MED 23, 1615–1620 (2008). https://doi.org/10.1007/s11606-008-0707-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0707-9