
Abstract
BACKGROUND: Postoperative complications are a significant source of morbidity and mortality. There are limited studies, however, assessing the impact of common postoperative complications on health care resource utilization.
OBJECTIVE: To assess the association of clinically important postoperative complications with total hospital costs and length of stay (LOS) in patients undergoing noncardiac surgery.
METHODS: We determined total hospital costs and LOS in all patients admitted to a single tertiary care center between July 1, 1996 and March 31, 1998 using a detailed administrative hospital discharge database. Total hospital costs and LOS were adjusted for preoperative and surgical characteristics.
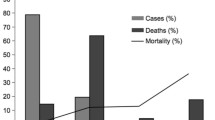
RESULTS: Of 7,457 patients who underwent noncardiac surgery, 6.9% developed at least 1 of the postoperative complications. These complications increased hospital costs by 78% (95% confidence interval [CI]: 68% to 90%) and LOS by 114% (95% CI: 100% to 130%) after adjustment for patient preoperative and surgical characteristics. Postoperative pneumonia was the most common complication (3%) and was associated with a 55% increase in hospital costs (95% CI: 42% to 69%) and an 89% increase in LOS (95% CI: 70% to 109%).
CONCLUSIONS: Postoperative complications consume considerable health care resources. Initiatives targeting prevention of these events could significantly reduce overall costs of care and improve patient quality of care.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Weingart SN, Iezzoni LI, Davis RB, et al. Use of administrative data to find substandard care: validation of the complications screening program. Med Care. 2000;38:796–806.
Fleischmann KE, Goldman L, Young B, Lee TH. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med. 2003;115:515–20.
Dimick JB, Chen SL, Taheri PA, Henderson WG, Khuri SF, Campbell DA Jr. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531–7.
Naglie G, Tansey C, Krahn MD, O’Rourke K, Detsky AS, Bolley H. Direct costs of coronary artery bypass grafting in patients aged 65 years or more and those under age 65. CMAJ. 1999;160:805–11.
Keon WJ, Menzies SC, Lay CM. Cost of coronary artery bypass surgery: a pilot study. Can J Surg. 1985;28:283–6.
Krueger H, Goncalves JL, Caruth FM, Hayden RI. Coronary artery bypass grafting: how much does it cost? CMAJ. 1992;146:63–8.
Lawrence VA, Dhanda R, Hilsenbeck SG, Page CP. Risk of pulmonary complications after elective abdominal surgery. Chest. 1996;110:744–50.
Kalish RL, Daley J, Duncan CC, Davis RB, Coffman GA, Iezzoni LI. Costs of potential complications of care for major surgery patients. Am J Med Quality. 1995;10:48–54.
Naessens JM, Huschka TR. Distinguishing hospital complications of care from pre-existing conditions. Int J Qual Health Care. 2004;16(suppl 1):i27–35.
U.S. Department of Health and Human Services. International Classification of Diseases, 9th revision (Clinical Modification). Washington, DC: Public Health Service, U.S. Department of Health and Human Services; 1998.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
Southern DA, Quan H, Ghali WA. Comparison of the Elixhauser and Charlson/Deyo methods of comorbidity measurement in administrative data. Med Care. 2004;42:355–60.
Quan H, Parsons GA, Ghali WA. Assessing accuracy of diagnosis-type indicators for flagging complications in administrative data. J Clin Epidemiol. 2004;57:366–72.
Bugar JM, Ghali WA, Lemaire JB, Quan H. Canadian Perioperative Research Network. Utilization of a preoperative assessment clinic in a tertiary care centre. Clin Invest Med. 2002;25:11–8.
McCarthy EP, Iezzoni LI, Davis RB, et al. Does clinical evidence support ICD-9-CM diagnosis coding of complications? Med Care. 2000;38:868–76.
Lawthers AG, McCarthy EP, Davis RB, Peterson LE, Palmer RH, Iezzoni LI. Identification of in-hospital complications from claims data. Is it valid? Med Care. 2000;38:785–95.
Collins TC, Daley J, Henderson WH, Khuri SF. Risk factors for prolonged length of stay after major elective surgery. Ann Surg. 1999;230:251–9.
McAlister FA, Khan NA, Straus SE, et al. Accuracy of the preoperative assessment in predicting pulmonary risk after nonthoracic surgery. Am J Respir Crit Care Med. 2003;167:741–4.
Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–9.
Zhan C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. 2003;290:1868–74.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have no conflicts of interest to declare for this paper.
Dr. Khan is funded by Canadian Institutes of Health Research (CIHR) and Michael Smith Foundation for Health Research postdoctoral fellowship awards. Dr. Khan also received postdoctoral fellowship funding from the Alberta Heritage Foundation for Medical Research (AHFMR) during the analysis of this data. Dr. Ghali is funded by AHFMR as a Scholar and holds a Canada Research Chair. Dr. Hude Quan is funded by CIHR as New Investigator and AHFMR as a Population Health Investigator.
Rights and permissions
About this article
Cite this article
Khan, N.A., Quan, H., Bugar, J.M. et al. Association of postoperative complications with hospital costs and length of stay in a tertiary care center. J Gen Intern Med 21, 177–180 (2006). https://doi.org/10.1007/s11606-006-0254-1
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s11606-006-0254-1