
Abstract
Background
Screening high-risk individuals (HRI) can detect potentially curable pancreatic ductal adenocarcinoma (PDAC) and its precursors. We describe the outcomes of high-risk individuals (HRI) after pancreatic resection of screen-detected neoplasms.
Methods
Asymptomatic HRI enrolled in the prospective Cancer of the Pancreas Screening (CAPS) studies from 1998 to 2014 based on family history or germline mutations undergoing surveillance for at least 6 months were included. Pathologic diagnoses, hospital length of stay, incidence of diabetes mellitus, operative morbidity, need for repeat operation, and disease-specific mortality were determined.
Results
Among 354 HRI, 48 (13.6%) had 57 operations (distal pancreatectomy (31), Whipple (20), and total pancreatectomy (6)) for suspected pancreatic neoplasms presenting as a solid mass (22), cystic lesion(s) (25), or duct stricture (1). The median length of stay was 7 days (IQR 5–11). Nine of the 42 HRI underwent completion pancreatectomy for a new lesion after a median of 3.8 years (IQR 2.5–7.6). Postoperative complications developed in 17 HRI (35%); there were no perioperative deaths. New-onset diabetes mellitus after partial resection developed in 20% of HRI. Fourteen PDACs were diagnosed, 11 were screen-detected, 10 were resectable, and 9 had an R0 resection. Metachronous PDAC developed in remnant pancreata of 2 HRI. PDAC-related mortality was 4/10 (40%), with 90% 1-year survival and 60% 5-year survival, respectively.
Conclusions
Screening HRI can detect PDAC with a high resectability rate. Surgical treatment is associated with a relatively short length of stay and low readmission rate, acceptable morbidity, zero 90-day mortality, and significant long-term survival.
Clinical Trial Registration Number
NCT2000089
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the third leading cause of cancer-related death in the USA and is expected to become the second leading cause of cancer-related death in the USA by the year 2020, surpassing colorectal cancer. The majority of PDACs present with advanced disease.1 The overall 5-year survival rate remains low, at only 9%, with only 20% of patients surviving one year.2 Pancreatic screening and early detection are considered by expert opinion and available evidence3,4,5,6 to be the best way to improve clinical outcomes. About 10% of patients with PDAC have a family history of pancreatic cancer or a known hereditary cancer-associated syndrome.7 Individuals at high risk (HRI) for PDAC include unaffected relatives from familial pancreatic cancer (FPC) kindreds with at least one affected first-degree relative and one affected second-degree relative and individuals who carry deleterious mutations in familial pancreatic cancer genes.4 The familial pancreatic cancer genes include BRCA2, ATM, PALB2, BRCA1, CDKN2A (familial atypical multiple mole melanoma syndrome or FAMMM syndrome), STK11 (Peutz-Jeghers syndrome), genes that cause Lynch syndrome (such as MLH1 and MSH2).7, 8 These HRI can be offered surveillance in formal multidisciplinary pancreatic cancer screening programs.4
It has been shown that some PDACs arise from well-defined precursor lesions such as microscopic pancreatic intraepithelial neoplasia (PanINs) or macroscopic intraductal papillary mucinous neoplasms (IPMNs)7, 9, 10 and detection of high-risk PDAC precursors might be suitable targets for screening.4 Consensus guidelines for the surveillance of HRI have been developed.4 The goal of screening and surveillance of HRI is to detect early stage pancreatic cancer and high-grade dysplasia (HGD) in precursor lesions (IPMN and PanIN).
Little has been reported regarding the outcome of HRI who have undergone pancreatic resection for screening-detected lesions. A recent paper from our group evaluated risk factors for neoplastic progression among HRI in the CAPS program.5 In this study, we report the outcomes after pancreatic surgery for screening-detected lesions.
Methods
Study Design
We analyzed prospectively collected data from the Cancer of the Pancreas Screening (CAPS) studies between 1998 and 201411,12,13 that consecutively enrolled HRI for one-time screening (CAPS 1–4) at The Johns Hopkins Hospital.11,12,13 In this report, outcomes were tracked for HRI who continued surveillance at The Johns Hopkins Hospital. Outcomes reported in the current study were updated from enrollment to November 2017 by review of the electronic medical chart, mailed or emailed patient survey, telephone call by a study team member, and internet searches of obituaries and registered deaths. The study protocols were approved by the Institutional Review Board at the Johns Hopkins University (study ID NA_00087754, NA_00044490, and NA_00005455).
Study Population
HRIs were defined as those with any of the following conditions: (1) three or more affected blood relatives with PDAC, including at least two related by first-degree, and with at least one of the affected related to the at-risk relative by first degree, (2) at least two affected first-degree relatives with PDAC, (3) Peutz-Jeghers syndrome regardless of family history of PDAC, (4) deleterious germline p16 (CDKN2A) gene mutation or familial atypical multiple mole melanoma syndrome with one affected first-degree relative, (5) deleterious germline BRCA2 gene mutation with one affected first-degree relative, (6) deleterious germline BRCA2 gene mutation with two affected family members (non-first-degree) with PDAC, (7) deleterious germline PALB2 gene mutation with one affected first-degree relative, (8) deleterious germline ATM gene mutation, and/or (9) deleterious germline mismatch repair gene mutation, such as Lynch syndrome, with one affected first-degree relative4 Those with Peutz-Jeghers syndrome were screened starting at the age of 30 years.4 Individuals at high risk based on their family history began screening at the age of 50 years.5
Exclusion criteria were (1) established or clinically suspected pancreatic cancer, (2) prior pancreas-specific imaging protocol performed in the past 3 years, (3) medically unable to have an endoscopy, CT, or MRI procedure, (4) advanced or end-stage medical disease, and (5) follow-up < 6 months from baseline screening at The Johns Hopkins CAPS program.
Screening and Surveillance Methods
Endoscopic ultrasonography (EUS) was used for baseline screening from 1998 to 2002 (CAPS 1 study),12 and pancreatic protocol computed tomography (CT) was added to EUS from 2002 to 2004 (CAPS 2 study).11 In the CAPS 3 study, 216 subjects underwent one-time screening with EUS, CT, and magnetic resonance imaging (MRI) pancreatic protocol with cholangiopancreatography (MRCP).13 Since 2005, surveillance of enrolled HRI was performed mainly with EUS and MRCP, given higher detection rates of small pancreatic lesions compared with computed tomography (CT) without repeated radiation exposure.4, 7, 9, 13 CT was used if there was any solid pancreatic lesion, rapid cyst growth, or an indeterminate imaging abnormality such as benign-appearing cyst with mild main duct dilation detected by EUS or MRCP.
Highly experienced gastroenterologists (MC, EJS, and AML) performed sedated upper endoscopy followed by EUS imaging using an electronic radial and/or linear echoendoscope (Olympus Corporation, Center Valley, PA). Fine-needle aspiration was performed during the same sedation procedure as indicated by the presence of a pancreatic mass or mural nodule in a cyst, according to standard medical care guidelines, with on-site cytopathology review of specimens for adequate tissue acquisition. Highly experienced radiologists (I.K. and E.F.) interpreted MRI and CT results. Gadolinum-enhanced MRCP was used using a specific pancreas protocol. All MRI sequences were obtained at a minimum of 1.5 or 3.0 Tesla (GE, Waukesha, WI or Siemens, Malvern, PA) using a phased-array torso coil. Axial breath-hold unenhanced and dynamic contrast-enhanced (0.1 mmol/kg of body weight), T1-weighted, 3-dimensional, fat-suppressed, spoiled gradient-echo imaging were acquired in the arterial, portal venous, and delayed phases at 20 seconds, 70 seconds, and 3 min, respectively.
HRI with no pancreatic abnormalities at baseline were followed at 12-month intervals, typically alternating between EUS and MRI. HRI with a low-risk cyst without worrisome features (cyst size > 3 cm, mural nodules, thickened/enhancing cyst walls, main duct dilation 5–9 mm, abrupt change in duct caliber with distal atrophy, lymphadenopathy)14, 15 or rapid cyst growth (defined as > 2 mm in 6 months or > 4 mm per year)5 continued surveillance at 6–12 months. Those with an indeterminate solid lesion had follow-up screening at 3 months, if surgery was not imminent. For those with a dilated pancreatic duct with or without a benign-appearing cyst, or main pancreatic duct stricture without a mass, repeat imaging was performed at 3 months.5 Surveillance intervals were adjusted depending upon the stability of the indeterminate lesion and absence of radiologic features of neoplastic progression.5
HRI with a suspicious soft tissue lesion or discrete solid pancreatic mass were referred to a pancreatic surgeon. All patients with indeterminate lesions, masses, or cysts with worrisome features were discussed at regular scheduled multidisciplinary conference involving surgeons, radiologists, gastroenterologists, and pathologists.
Patients with planned total pancreatectomy or completion pancreatectomy saw a local endocrinologist and received counseling on glucose monitoring, diet, and postoperative diabetes management from a physician specializing in diabetes and diabetes nurse.
Pancreatic surgery at The Johns Hopkins Hospital was performed by highly experienced pancreatic surgeons (MW, CY, RS, JH, MM, and CW). Pathologic specimens were processed according to an established protocol involving careful examination of the frozen sections during surgery, the final gross specimen, and histologic sections obtained at a maximum of 1-cm intervals. One expert pathologist (R.H.) provided a pathologic diagnosis using a standard,10 consensus international classification system and revised classification system from the Baltimore consensus meeting.16
To report surgical morbidity, we report the specific complications following pancreatic resection proposed by the International Study Group of Pancreatic Surgery in 2017.17 Delayed gastric emptying (the inability to return to a standard diet by the end of the first postoperative week requiring prolonged nasogastric intubation) as well as postoperative pancreatic fistula (drain output of any measurable volume of fluid with an amylase level > 3 times the upper limit of institutional normal serum amylase activity, associated with a clinically relevant development/condition related directly to the postoperative pancreatic fistula).17 Other postpancreatectomy complications included postpancreatectomy hemorrhage.17 Other determined outcomes were overall mortality,18, 19 morbidity, length of stay,20, 21 and 30-day readmission and 90-day mortality.19 We assessed the incidence of new-onset diabetes mellitus in those with partial pancreatic resection (either pancreaticoduodenectomy or distal pancreatectomy, without subsequent completion pancreatectomy), which was defined by the American Diabetes Association, to include (1) hemoglobin A1C ≥ 6.5%, (2) fasting plasma glucose ≥ 126 mg/dL, (3) 2-h plasma glucose ≥ 200 mg/dL during an oral glucose tolerance test, and/or (4) those with classic symptoms of hyperglycemia or hyperglycemic crisis with a random plasma glucose ≥ 200 mg/dL.22
Statistical Analyses
The chi-square, Fisher’s exact test, and t test were performed for categorical and numeric variables, where appropriate, to compare outcomes. Two-tailed p values less than 0.05 were considered statistically significant. Statistical analyses were performed using Stata version 14.1 (Stata Corporation, Dallas, TX) and JMP Pro 13.0 (SAS Institute Inc., Cary, NC) software packages.
Results
Baseline Patient Characteristics
From 584 HRIs enrolled in the CAPS 1–4 studies beginning in 1998, 123 HRIs were excluded because of < 6-month follow-up and 104 were not included due to continued surveillance at other institutions. For the current study, 354 asymptomatic HRIs who continued surveillance at the Johns Hopkins Hospital with follow-up of more than 6 months after baseline screening were included. The mean follow-up time at study closure to November 2017 was 7.6 years (range 0.7–16.6 years). Among 48 HRI (mean age ± SD 69 ± 10.5 years, 27 males (56.3%)) who had screening-detected lesions and underwent pancreatic resections, 42 patients (87.5%) had first-degree relatives with PDAC, of which 30/42 patients (71.4%) also had second-degree relatives with PDAC. All patients were non-Hispanic white. There were 19/48 patients (39.6%) with history of cigarette smoking, and 6/48 (12.5%) had active smoking at the index screening. There were 6 patients (12.5%) with baseline diabetes, of which one patient was insulin dependent, prior to the index screening. Mean body mass index prior to index pancreatic resection was 27.9 ± SD 5.4 kg/m2.
Type and Number of Pancreatic Operations
Among 48 HRI who had screening-detected lesions and underwent pancreatic resections, 57 operations were performed (48 initial and 9-second surgery procedures) between November 1998 and January 2017. The type of the initial operation included pancreaticoduodenectomy (n = 16, 33.3%), distal pancreatectomy (n = 26, 54.2%), and total pancreatectomy (n = 6, 12.5%). Eight operations (16.7%) were minimally invasive (5 laparoscopic and two robotic-assisted distal pancreatectomy, 1 laparoscopic total pancreatectomy) (Table 1).
The first 16 operations performed between 1998 and 2007 were partial resections aimed at treating the detected lesion or the most concerning dominant lesion(s) in HRI with multiple pancreatic lesions. All 6 total pancreatectomies and 9 completion pancreatectomies were performed for multifocal and/or metachronous lesions beginning in March 2007.
Among 48 patients who underwent initial partial pancreatic resection, 9 patients (19%) that eventually had completion pancreatectomy (4 pancreaticoduodenectomy, 5 distal pancreatectomy) were operated for new lesions in the remnant gland detected at a median of 3.8 years. Six of these patients had new and/or enlarging cysts—1 BD-IPMN with HGD, 2 BD-IPMN with moderate-grade dysplasia, 3 with BD-IPMN with low-grade dysplasia but 1 HRI also had 10 synchronous PanIN-3 lesions. Three of the remaining 9 patients had second surgeries for new solid masses (1 HRI with a well differentiated, grade 1, nonfunctional pancreatic neuroendocrine tumor (PanNET); 1 HRI with PanIN-2 with lobulocentric atrophy, and 1 HRI with PDAC detailed below). Another patient who initially had a Whipple for a well-differentiated T3N1M0 grade 1 PanNET presenting as an asymptomatic mass in the head at baseline screening developed a new 1 cm low-grade well-differentiated PanNET in the tail, which was resected at completion distal pancreatectomy 6 years after the index surgery (Table 1).
Two of the 48 patients (4%) under surveillance developed a metachronous PDAC in the remnant pancreas after initial surgery; both for benign IPMN. One of these patients with an incident PDAC underwent pancreaticoduodenectomy for BD-IPMN with low-grade dysplasia and developed a mass with distal atrophy and duct dilation in the body of the pancreas 7 years later while under surveillance. He delayed surgery for almost a year and final pathology showed a T3N0M0 PDAC. The second patient with a metachronous PDAC had Whipple procedure for a mixed IPMN with moderate dysplasia in a BD-IPMN and low-grade dysplasia in the main duct. He developed PDAC in the tail with the metastatic disease despite annual CT surveillance after his first surgery 5 years later. The PDAC presented with duct dilation and an indeterminate soft tissue lesion at the anastomosis.
Nonoperable PDAC in HRI Without Prior Surgery
Three of the 354 screened HRI presented with unresectable and/or metastatic PDAC after their initial screening visit; all were either late or had stopped pancreas surveillance. One Ashkenazi Jewish patient with 2 affected first-degree relatives had a mildly dilated main pancreatic duct with mild features of chronic pancreatitis at baseline. He developed new subcentimeter pancreatic cysts in the tail and head of the pancreas. He was 2 years overdue for his annual surveillance imaging due to intervening medical problems, which in retrospect, were manifestations of a paraneoplastic syndrome (peripheral neuropathy, coagulopathy). He presented with a PDAC in the head with liver metastases.
The second patient underwent initial screening EUS, CT, and MRI as part of the CAPS 3 study. He tested negative for germline mutations in the BRCA1 and BRCA2 genes and stopped surveillance. Seven years later, he presented with symptomatic unresectable PDAC and opted for palliative care. He tested positive for a germline PALB2 gene mutation.
A third patient had a BRCA2 mutation who had been diagnosed with stage 3 ovarian cancer with a baseline screening CT, developed a subcentimeter cyst in the head of the pancreas 1 year later. She was advised to have surgery for rapid enlargement of the cyst after a 3-month follow-up EUS. She declined surgery. Unfortunately, she developed a symptomatic primary PDAC in the head of the pancreas with liver metastases 21 months after her initial visit.
Surgical Outcomes: Length of Stay, Operative Morbidity, and Mortality
The median length of stay for pancreatic resection was 7 days (IQR 5–11). Those receiving total pancreatectomy required longer length of stay (median 11.5 days, IQR 8.5–13.3) compared with those received Whipple operation or distal pancreatectomy (p = 0.0009, Table 2). There were 10 patients in this cohort with screening-detected PDAC who underwent pancreatic resection(s), of which 9 patients (90%) achieved negative margin (R0) resection. The tenth patient with resectable PDAC had a microscopic positive margin (Whipple).
Overall, postpancreatectomy complications developed in 17 of 48 patients (35.4%) (Table 2). Patients receiving Whipple operation at initial surgery had more complications (10/16, 62.5%) compared with other groups (p = 0.02), particularly delayed gastric emptying (6/16, 37.5%, p = 0.01). Other complications such as surgical site infection, anastomotic leak, and cholangitis were comparable among partial and total pancreatectomy groups (Table 2). Length of stay was longest in total pancreatectomy patients. Weight loss was lowest in distal pancreatectomy patients compared with pancreaticoduodenectomy and total pancreatectomy patients. Minimally invasive pancreatic resection was not associated with improved outcomes compared with open pancreatic resection in this cohort.
There were 3 hospital readmissions within 30 days (6.2%). These included an intra-abdominal abscess on postoperative day 10 requiring a 12-day hospitalization and percutaneous drainage, dehydration on postoperative day 18 requiring a 3-day hospitalization, and admission for delayed gastric emptying on postoperative day 28 initially requiring total parenteral nutrition followed by percutaneous endoscopic gastrostomy. There was no 90-day mortality or intra-abdominal hemorrhage.
Postoperative Diabetes Mellitus
Six patients had diabetes at baseline screening (1 type 1 diabetes, 5 type 2 diabetes). There were 30 patients without diabetes mellitus prior to surgery who had partial pancreatic resection. Six of these patients (20%) developed diabetes, with no difference in those who had a Whipple procedure (20%) versus distal pancreatectomy (20%) (Table 2). One of the 6 patients who underwent total pancreatectomy had prior history of diabetes. Preoperative obesity, defined as a body mass index of 30 kg/m2 or higher, was not associated with new-onset diabetes (odds ratio 7.2, 95% CI 0.58–175.3, p = 0.12).
Among 48 HRI who had pancreatic resections, 10 patients (21%) received an insulin pump after pancreatic resection. One of these patients (10%) had partial pancreatic resections. Patients with diabetes at baseline prior to pancreatic resection were more likely to be managed with an insulin pump postoperatively compared with those without preexisting diabetes (4/6 (67%) versus 6/42 (14%) patients, respectively, p = 0.01). Two of the 15 (13%) patients with eventual complete pancreatectomy (6 initial total pancreatectomy plus 9 with completion pancreatectomy) developed severe dysglycemia requiring an emergency department visit, including one who required a hospitalization. However, no severe hypoglycemic complications (syncope, seizure, death) occurred in any patient.
Pathologic and Oncologic Outcomes According to Surgical Indication
The final diagnoses, indication for surgery, survival, and cause of death for these patients are summarized in Table 1. Twenty-two HRI underwent surgery for detected solid pancreatic masses. Four of these HRI who had surgery for a pancreatic mass had a PanNET without evidence of PDAC or PanIN-3 (Table 1). All 4 PanNET were confirmed preoperatively by EUS-guided fine needle aspiration. Of the remaining 9 surgical patients who developed solid pancreatic masses during surveillance, 8 were proven to be PDAC and 1 was an IPMN with HGD.
Three patients with pancreatic cysts (1 with associated duct dilation, and the two other with rapid cyst growth) developed PDAC (Table 1). Five HRI with cysts with at least one worrisome feature according to the International Consensus Guidelines (specifically, mural nodule (1), main duct dilation with mural nodules (1), rapid growth (3)) were proven to have IPMN with HGD. In 4 patients who had surgery for a pancreatic cyst with main duct dilation (1) or rapid growth plus multifocal cysts (2), incidental PanIN-3 was found in the resected pancreas along with benign branch duct IPMN. One duct stricture without a mass proved to be an unusual isolated PanIN-3 in the main duct.
The remaining 24 HRI presenting with indeterminate small solid masses (10) or cysts with worrisome features (14) had only low or moderate grade precursor lesions (Table 1).
There were no significant differences in the proportion of PDAC and tumors with HGD resected during the early, middle, and later study periods, 6/15 (40%) between 1998 and 2006; 6/17 (35%) between 2006 and 2010; and 8/16 (50%) from 2010 to 2017 (p = 0.68).
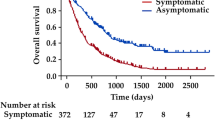
In summary, 11 PDAC and 10 PDAC high-grade precursor neoplasms (6% of the 354 cohort) were detected during surveillance and surgically treated during the 19-year study period. The final pathological staging for the 10 resected PDAC patients is detailed in Table 1, including two stage I and eight stage II cancers. Seven of the 10 HRI with resected PDACs received adjuvant chemoradiation therapy. Importantly, the overall mortality and disease-specific mortality for operated PDAC detected during 19-year study period were 60% and 40%, respectively. Two of the resected PDAC patients died of non-PDAC causes. One patient survived 12 years after surgery but died of complications from surgery for an incident gastric cancer. The other PDAC survivor with stable recurrent disease died from complications after a motor vehicle accident 2 years after his total pancreatectomy.
The 1-year overall survival was 90% and 5-year overall survival of 60% for PDAC patients (Table 1). All but two of the 34 HRI that underwent resection for with pancreatic precursor lesions were alive at study end. The 2 deceased HRI with benign precursors died of non-PDAC causes at 7 and 11 years after surgery.
Discussion
The CAPS cohort (consisting of HRI enrolled in the CAPS 1–4 studies) is the largest single center cohort of individuals at high risk for pancreatic cancer with the longest follow-up (19 years) to date. We recently reported the incidence, rate, and risk factors for neoplastic progression to PDAC or IPMN-HGD/PanIN3 after baseline screening in this long-term cohort.5 We found that the majority (93%) of progressors (neoplastic progression was defined by the development of pathologically proven PDAC and/or IPMN-HGD/PanIN3, radiologic progression was defined as the development of a lesion with one or more worrisome features after baseline imaging)5 had lesions with worrisome features prior to their diagnosis (solid mass, dilated main pancreatic duct, abrupt change in duct caliber, and rapid cyst growth > 4 mm/year) that were detectable by EUS, MRI, and/or CT. We also noted the presence of multiple cysts (> 3) at baseline was a significant risk factor for neoplastic progression, which occurred at an average age of 67 years. The median time from baseline to PDAC diagnosis of 4.8 years (interquartile range 1.6–6.9 years).5
The current study focuses on the outcomes of operated HRI. The overall postoperative complication rate was 35% with zero 90-day mortality, which compares favorably with previously published data regarding complications and death after pancreatic resection of 30–60%18 and 1.89%17 to 7.4%,18 respectively. In this study, we used the definitions of delayed gastric emptying, pancreatic fistula, and pancreatic hemorrhage following those proposed by the International Study Group of Pancreatic Surgery.17 The complications found in this cohort were comparable with prior published data using the same definitions, including 14.6–24.2% risk of delayed gastric emptying23 and 12% risk of grade B pancreatic fistula.24 There was no intra-abdominal hemorrhage in our cohort; prior prospective studies have reported postpancreatectomy hemorrhage rates as high as 5.7%.25Other surgical-related outcomes, without established definitions by the International Study Group of Pancreatic Surgery, remained low, including surgical site infection as well as cholangitis.
With regard to index length of stay, our HRI treated with pancreaticoduodenectomy had relatively shorter average length of stay of 7 days, compared with that reported in a recent analysis of pancreaticoduodenectomy procedures in the ACS-NSQIP targeted pancreatectomy database (length of stay 10–11 days).20 The index length of stay in our CAPS cohort that underwent distal pancreatectomy (6 days) was comparable with that reported in large Norwegian database including 546 distal pancreatic resections (length of stay 7 days).21 Furthermore, the 30-day readmission rate (3/48 patients, 6.2%) in our CAPS cohort was lower than that reported in recently published surgical series (13.9–19.1%).20, 21
The incidence rates of postoperative diabetes from this series (20% after Whipple, 20% after distal resection) are comparable with those noted in prior published studies reporting 18% and 29% of patients who underwent pancreaticoduodenectomy and distal pancreatectomy, respectively.26 However, recent data suggest a lower incidence of diabetes after pancreatic surgery than previously reported. In patients treated with a Whipple procedure, the incidence of postoperative diabetes was 10.6% in a large multicenter prospective study and 14.5% in a systematic review and meta-analysis.27 A systematic review showed that 14% of patients developed new-onset diabetes after distal pancreatectomy.28 Our relatively higher rates of new-onset diabetes compared with more recent data might be related to the presence of lobulocentric atrophy and chronic pancreatitis associated with PanIN,29 the small study sample size, and the accumulating risk for diabetes in older patients.30
Prophylactic pancreatectomy is not recommended as the operative approach for HRI.4 Only 20 of 48 (42%) HRI who underwent partial pancreatectomy had PDAC or high-grade precursors in their resected pancreata; these are the main targets for screening defined by the International CAPS Consortium.4 The remaining HRI (58%) had lower-grade neoplasms, which one could argue did not, in hindsight, require surgery. Many of these pancreatic resections occurred in the earlier years of the CAPS program when the indications for surgery included resection of lower grade neoplasms.11 Selection of HRI for surgery remains challenging. When a solid mass is detected in a HRI, surgery is indicated in an operable patient, regardless of the EUS-guided cytological diagnosis. False positive and false negative cytology results have been reported in several pancreatic screening studies.6, 11,12,13, 31 Furthermore, the management of detected cystic lesions in HRI is even more difficult, particularly when the patient is healthy and asymptomatic. Pancreatic cysts are the most common imaging abnormality in HRI and the majority are low-risk BD-IPMNs.4, 13 The worrisome features and high-risk stigmata previously described to aid in the management of sporadic mucinous cysts14, 15 are not sufficiently specific for PDAC or precursors with HGD. Their absence also does not assure us of the absence of malignancy.11,12,13, 31,32,33,34 Hence, the data from our CAPS studies5, 11,12,13 and other surveillance studies 6, 31,32,33,34,35,36 suggest that pancreatic imaging is insufficient for the optimal selection of patients for surgery. Early detection and prevention of PDAC could be improved by the discovery and validation of biomarkers in cyst fluid,37, 38 juice,39,40,41 and blood 42,43,44 that may minimize unnecessary surgery for low-risk tumors.
Some limitations of our study should be considered. First, the CAPS studies were conducted in an academic tertiary referral center with highly skilled endoscopists, pancreatic surgeons, radiologists, and pathologists, limiting generalizability of pancreatic surgery outside a specialized center with a multidisciplinary surveillance program. Second, the current study only reports the outcomes from patients diagnosed and followed at one hospital. Third, the proportion of patients in our CAPS cohort that underwent pancreatic surgery was small precluding more extensive evaluation of surgical management. Fourth, practice has evolved over the study period, with improved understanding, and better imaging technology. The indications for surgical resection have evolved over time but remain individualized tailored to estimated cancer risk based on lesion characteristics by imaging, estimated cancer risk based on age, inherited/familial risk factors, and patient preferences. Finally, the CAPS study HRI are a highly motivated, relatively healthy group of patients that may have better outcomes that are not representative of other patients.
In conclusion, pancreatic resection for screening-detected lesions in HRI was associated with reasonable morbidity, relatively short length of stay and low readmission rate, no 90-day mortality, and significant survival compared with the national data on sporadic pancreatic cancer.
References
Clancy TE. Surgery for pancreatic cancer. Hematol Oncol Clin North Am 2015;29:701–16.
Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2019. CA Cancer J Clin 2019;69:7–34.
Corral JE, Mareth KF, Riegert-Johnson DL, et al. Diagnostic yield from screening asymptomatic individuals at high risk for pancreatic cancer: a meta-analysis of cohort studies. Clin Gastroenterol Hepatol 2019.
Canto MI, Harinck F, Hruban RH, et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013;62:339–47.
Canto MI, Almario JA, Schulick RD, et al. Risk of neoplastic progression in individuals at high risk for pancreatic cancer undergoing long-term surveillance. Gastroenterology 2018;155:740–51 e2.
Vasen H, Ibrahim I, Ponce CG, et al. Benefit of surveillance for pancreatic cancer in high-risk individuals: outcome of long-term prospective follow-up studies from three European expert centers. J Clin Oncol 2016;34:2010–9.
Hruban RH, Canto MI, Goggins M, et al. Update on familial pancreatic cancer. Adv Surg 2010;44:293–311.
Hu C, Hart SN, Polley EC, et al. Association between inherited germline mutations in cancer predisposition genes and risk of pancreatic cancer. JAMA 2018;319:2401–2409.
Hruban RH, Pitman MB, Klimstra D. Tumors of the pancreas. Rockville, Maryland: American Registry of Pathology, 2007.
Hruban RH, Takaori K, Klimstra DS, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol 2004;28:977–87.
Canto MI, Goggins M, Hruban RH, et al. Screening for early pancreatic neoplasia in high-risk individuals: a prospective controlled study. Clin Gastroenterol Hepatol 2006;4:766–81; quiz 665.
Canto MI, Goggins M, Yeo CJ, et al. Screening for pancreatic neoplasia in high-risk individuals: an EUS-based approach. Clin Gastroenterol Hepatol 2004;2:606–21.
Canto MI, Hruban RH, Fishman EK, et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology 2012;142:796–804; quiz e14-5.
Tanaka M, Fernandez-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183–97.
Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006;6:17–32.
Basturk O, Hong SM, Wood LD, et al. A revised classificaiton system and recommendations from the Baltimore consensus meeting for neoplastic precursor lesions in the pancreas. Am K Surg Pathol 2015;39:1730–41.
Dusch N, Lietzmann A, Barthels F, et al. International study group of pancreatic surgery definitions for postpancreatectomy complications: applicability at a high-volume center. Scand J Surg 2017;106:216–223.
Vollmer CM, Jr., Sanchez N, Gondek S, et al. A root-cause analysis of mortality following major pancreatectomy. J Gastrointest Surg 2012;16:89–102.
Swanson RS, Pezzi CM, Mallin K, et al. The 90-day mortality after pancreatectomy for cancer is double the 30-day mortality: more than 20,000 resections from the national cancer data base. Ann Surg Oncol 2014;21:4059–67.
Xourafas D, Pawlik TM, Cloyd JM. Independent predictors of increased operative time and hospital length of stay are consistent across different surgical approaches to pancreatoduodenectomy. J Gastrointest Surg 2018;22:1911–1919.
Lassen K, Nymo LS, Olsen F, et al. Benchmarking of aggregated length of stay after open and laparoscopic surgery for cancers of the digestive system. BJS Open 2018;2:246–53.
American Diabetes Association. Diagnosis and classifciation of diabetes mellitus. Diabetes Care 2010;33:S62–9.
Wente MN, Bassi C, Dervenis MD, et al. Delayed gastric emptying after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007;142:761–8
Bassi C, Marchegiani G, Dervenis C, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 2017;161:584–91.
Wente MN, Veit JA, Bassi C, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007;142:20–5.
Burkhart RA, Gerber SM, Tholey RM, et al. Incidence and severity of pancreatogenic diabetes after pancreatic resection. J Gastrointest Surg 2015;19(2):217–25.
Beger HG, Poch B, Mayer B, Siech M. New onset of diabetes and pancreatic exocrine insufficiency after pancreaticoduodenectomy for benign and malignant tumors: a systematic review and meta-analysis of long-term results. Ann Surg 2018;267(2):259–70.
De Bruijin KM, van Eijck CH. New-onset diabetes after distal pancreatectomy: a systematic review. Ann Surg 2015;261(5):854–61.
Brune K, Abe T, Canto M, et al. Multifocal neoplastic precursor lesions associated with lobular atrophy of the pancreas in patients having a strong family history of pancreatic cancer. Am J Surg Pathol 2006;30:1067–76.
Narayan KM, Boyle JP, Thompson TJ, et al. Lifetime risk for diabetes mellitus in the United States. JAMA 2003;290;1884–90.
Harinck F, Konings IC, Kluijt I, et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2016;65:1505–13.
Al-Sukhni W, Borgida A, Rothenmund H, et al. Screening for pancreatic cancer in a high-risk cohort: an eight-year experience. J Gastrointest Surg 2012;16:771–83.
Ludwig E, Olson SH, Bayuga S, et al. Feasibility and yield of screening in relatives from familial pancreatic cancer families. Am J Gastroenterol 2011;106:946–54.
Poley JW, Kluijt I, Gouma DJ, et al. The yield of first-time endoscopic ultrasonography in screening individuals at a high risk of developing pancreatic cancer. Am J Gastroenterol 2009;104:2175–81.
Schneider R, Slater EP, Sina M, et al. German national case collection for familial pancreatic cancer (FaPaCa): ten years experience. Fam Cancer 2011;10:323–30.
Verna EC, Hwang C, Stevens PD, et al. Pancreatic cancer screening in a prospective cohort of high-risk patients: a comprehensive strategy of imaging and genetics. Clin Cancer Res 2010;16:5028–37.
Springer S, Wang Y, Dal Molin M, et al. A combination of molecular markers and clinical features improve the classification of pancreatic cysts. Gastroenterology 2015;149:1501–10.
Maker AV, Carrara S, Jamieson NB, et al. Cyst fluid biomarkers for intraductal papillary mucinous neoplasms of the pancreas: a critical review from the international expert meeting on pancreatic branch-duct-intraductal papillary mucinous neoplasms. J Am Coll Surg 2015;220:243–53.
Suenaga M, Yu J, Shindo K, et al. Pancreatic Juice Mutation Concentrations Can Help Predict the Grade of Dysplasia in Patients Undergoing Pancreatic Surveillance. Clin Cancer Res 2018;24:2963–2974.
Yu J, Sadakari Y, Shindo K, et al. Digital next-generation sequencing identifies low-abundance mutations in pancreatic juice samples collected from the duodenum of patients with pancreatic cancer and intraductal papillary mucinous neoplasms. Gut 2017;66:1677–1687.
Kanda M, Sadakari Y, Borges M, et al. Mutant TP53 in duodenal samples of pancreatic juice from patients with pancreatic cancer or high-grade dysplasia. Clin Gastroenterol Hepatol 2013;11:719–30 e5.
Cohen JD, Javed AA, Thoburn C, et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc Natl Acad Sci U S A 2017;114:10202–7.
Cohen JD, Li L, Wang Y, et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018;359:926–30.
Poruk KE, Valero V, 3rd, He J, et al. Circulating epithelial cells in intraductal papillary mucinous neoplasms and cystic pancreatic lesions. Pancreas 2017;46:943–7.
Acknowledgments
CAPS 3 study participating centers and co-investigators (listed in alphabetical order) Dana Farber Cancer Institute, Boston, MA (Koenraad Mortele, John Saltzman, Sapna Syngal); The Mayo Clinic, Rochester, MN (Joel Fletcher, Gloria Petersen, Naoki Takahashi, Mark Topazian), MD Anderson Cancer Center, Houston, TX (Priya Bosale, Jeffrey Lee, Eric Tamm, Raghunandan Vikram), and University of California, Los Angeles, CA (James Farrell, Daniel Margolis).
Funding
This work was supported by the National Institutes of Health grants (CA210170, CA176828, CA62924, CA154823, CA132829), Susan Wojcicki and Dennis Troper, the Pancreatic Cancer Action Network, the Lustgarten Foundation for Pancreatic Cancer Research, the Rolfe Pancreatic Cancer Foundation, the John and Peter Hooven Memorial Endowment, Hugh and Rachel Victor, and ChiRhoCin, Inc.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: Marcia Canto and Michael Goggins.
Acquisition of data: Tossapol Kerdsirichairat, Madeline Ford, Ammar Javed, Marcia Canto, Anne Marie Lennon, Eun Ji Shin, Elliott Fishman, Ihab Kamel, Jin He, Richard Burkhart, Martin Makary, Richard Schulick, Charles Yeo, Matthew Weiss and Christopher Wolfgang.
Analysis and interpretation of data: Tossapol Kerdsirichairat, Amanda Blackford, Alison Klein, Marcia Canto, Michael Goggins, Ralph Hruban.
Drafted the manuscript: Tossapol Kerdsirichairat and Marcia Canto.
Statistical analysis: Tossapol Kerdsirichairat, Marcia Canto, Amanda Blackford.
Revised the manuscript and agreed with the manuscript’s results and conclusions: all authors.
Study support: Marcia Canto and Michael Goggins.
Obtained funding: Marcia Canto, Ralph Hruban, and Michael Goggins.
Study supervision: Marcia Canto, Michael Goggins.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Marcia I. Canto, MD MHS and Tossapol Kerdsirichairat, MD are co-first authors.
Michael Goggins and Christopher Wolfgang are co-senior authors.
All authors have met the criteria for authorship including (1) providing substantial contributions, (2) drafting the work and/or critically revising the intellectual content, (3) providing final approval, and (4) providing agreement to be accountable for all aspects of the work.
Rights and permissions
About this article

Cite this article
Canto, M.I., Kerdsirichairat, T., Yeo, C.J. et al. Surgical Outcomes After Pancreatic Resection of Screening-Detected Lesions in Individuals at High Risk for Developing Pancreatic Cancer. J Gastrointest Surg 24, 1101–1110 (2020). https://doi.org/10.1007/s11605-019-04230-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-019-04230-z