
Abstract
Introduction
While there is consensus on how to treat acute appendicitis, the most suitable treatment for an appendiceal inflammatory mass is still debated. This study compares the outcomes of operative and nonoperative management.
Material and Methods
We retrospectively evaluated 119 patients (2007–2011) with an appendiceal inflammatory mass, 85 of whom were treated nonoperatively and 34 operatively. Of the nonoperative patients, 69 did not receive interventional treatment and 16 underwent percutaneous drainage of an accompanying abscess; the data for these patients were analyzed separately.
Results
Of the noninterventional managed patients, 49 (71.0 %) experienced at least one recurrence and 37 (53.6 %) ultimately needed an acute surgical or radiological intervention. Of the 16 patients who underwent percutaneous drainage, 7 (43.8 %) experienced at least one recurrence and 6 (37.5 %) underwent an acute surgical or (second) percutaneous intervention. None of the operated patients had a recurrence and the incidence of complications was 17.6 %. The incidence of underlying malignant tumor in our study population was 5.9 %. In 35 patients, the definitive diagnosis remained unclear because the patients did not undergo surgery or follow-up colonoscopy after nonoperative treatment. The rate of extensive (ileocecal + hemicolonic) resection in all operated patients was 30.8 %.
Conclusion
We conclude that the high rate of recurrence and intervention in the nonoperative group and the high proportion of these patients who did not receive adequate follow-up despite the relatively high rate (5.9 %) of bowel malignancy support the operative management of an appendiceal inflammatory mass. Noninterventional management or a percutaneous intervention should be reserved as a bridge to surgery for patients with a large accompanying abscess or as treatment for patients with significant comorbidity. If nonoperative treatment is chosen, follow-up colonoscopy is mandatory to exclude malignancy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Appendicitis is the main cause of the surgical abdomen. Clinically, it can manifest in two ways. The classical and most common form is acute appendicitis, whereby the appendix rapidly becomes inflamed, potentially leading to perforation of the appendix and localized or generalized peritonitis. However, in a significant minority of cases, symptoms appear to develop gradually and are less severe. These patients present later, when the (perforated) appendix is enclosed in inflammatory tissue and an appendiceal inflammatory mass, sometimes partly suppurated, has formed.
In contrast to the treatment of acute appendicitis, in which the gold standard is appendectomy, the most suitable treatment for an appendiceal inflammatory mass has not yet been established.1 Although both operative and nonoperative treatment options are available, nonoperative management, first described by Ochsner in 19022 and popularized by Bailey,3 is probably the more common option, especially after it became possible to percutaneously drain an accompanying intra-abdominal abscess.
In our clinic, both operative and nonoperative methods are used to treat patients with an appendiceal inflammatory mass, with varying success. The complicated clinical course of a number of our nonoperatively treated patients prompted debate about the best way to manage these patients. We therefore evaluated the outcomes of all of our patients treated for an appendiceal inflammatory mass and hypothesized that nonoperative treatment would be associated with a lower success rate and higher morbidity than operative treatment.
Methods
All patients treated for appendicitis between January 1, 2007 and December 31, 2011 in the Medical Centre Alkmaar, the Netherlands, were reviewed. Eligibility was based on patient history, physical examination, and additional investigations so that appendiceal inflammatory mass was the working diagnosis at hospital admission. Patients with acute appendicitis were excluded. Data on patient status at admission, treatment outcome, and follow-up were retrieved.
Patients who underwent surgery within 24 h of diagnosis formed the operative group, and patients whose initial treatment was not surgery formed the nonoperative group. The latter group was further subdivided into patients who received conservative treatment without any intervention and those who underwent prompt percutaneous drainage of an accompanying abscess.
Analysis
Data are expressed as means ± the standard deviation (SD). Differences between the data of the treatment groups were analyzed by using a Chi-square test or a Kruskal–Wallis test where appropriate. A two-tailed p value of < 0.05 was considered statistically significant. Statistical analyses were performed by using SPSS Statistics version 21 (IBM, Chicago, IL, USA).
Results
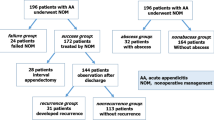
We identified 119 patients treated for an appendiceal inflammatory mass. Eighty-five patients (71.4 %) were treated nonoperatively, and 34 patients (28.6 %) were treated operatively. In the nonoperative group, 69 (58.0 %) patients underwent no intervention and 16 patients (13.4 %) underwent prompt percutaneous drainage of an accompanying abscess.
Patient characteristics and assessment are described in Table 1. There were no significant differences in sex, age, ASA classification, presence of a palpable mass, temperature, C-reactive protein level, and white blood cell count between the two main groups. The duration of symptoms before presentation was significantly shorter in the operative group (5.4 days) than that in the nonintervention (8.3 days) and drainage (8.4 days) groups. Radiological imaging was performed in all patients in the nonoperative group and in 30 patients (88.2 %) in the operative group. An accompanying abscess was diagnosed in 14 patients (20.3 %) in the nonintervention group, in 16 patients (100 %) in the drainage group, and in 14 patients (14.2 %) in the operative group. The 14 patients who were diagnosed with an accompanying abscess that was not promptly drained had an abscess <3 cm in diameter inaccessible for percutaneous drainage and lacked clinical parameters that coerced intervention.
Outcome variables are shown in Table 2. The average hospital stay was 13.9 days in the nonintervention group, 12.3 days in the drainage group, and 9.2 days in the operative group; the rate of re-admission was 47.7 %, 31.3 %, and 5.9 %, respectively.
In the nonintervention group, 38 patients (55.1 %) experienced one recurrence, 9 patients (13.0 %) experienced two recurrences, and 2 patients (2.9 %) experienced three recurrences. Management of these recurrences required one or multiple interventions in 37 patients (53.3 %). In the drainage group, five patients (31.3 %) experienced one recurrence and two patients (12.5 %) experienced two recurrences. Management of these recurrences required one or multiple interventions in six patients (37.5 %). There were no recurrences in the operative group. The rate of complications other than recurrence was 8.7 % in the nonintervention group, 31.1 % in the drainage group, and 17.6 % in the operative group. The various complications are listed in Table 2.
In the nonintervention group, 25 patients (36.2 %) had a colonoscopy as follow-up investigation and 44 patients (63.8 %) did not; this last group included 19 patients in whom the diagnosis was established by histological examination of a specimen taken during surgery for a recurrence. In the drainage group, 5 patients (31.3 %) had a colonoscopy and 11 patients (68.8 %) did not; the latter group included 3 patients who underwent surgery for a recurrence. In the operative group, in most cases, the diagnosis was established by pathological examination of surgical specimens; however, appendectomy was not performed in three patients (8.8 %), so there was no material available for pathological examination. One of these patients had a follow-up colonoscopy. All patients who were diagnosed with a malignant tumor by histopathological investigation of surgical specimens had a follow-up colonoscopy to exclude malignancy in the remaining colon.
Overall, 69 patients (58.0 %) were diagnosed with appendicitis, 12 patients (10.1 %) with a tumor (malignant in 7 patients), 1 patient (0.85 %) with Crohn’s disease, 1 patient (0.85 %) with diverticulitis, and 1 patient (0.85 %) with endometriosis. A definitive diagnosis was not established in 35 patients (29.4 %) because these patients did not undergo surgery or have follow-up investigations.
In total, 30 (46.2 %) appendectomies were performed, 16 (24.6 %) ileocecal resections, 9 (13.8 %) interval appendectomies, 6 (9.2 %) surgical drainages, and 4 (6.2 %) right hemicolectomies. None of the patients needed an ileostomy, and anastomotic healing was uncomplicated.
Discussion
Nonoperative treatment for an appendiceal inflammatory mass, the Ochsner-Sherren regimen,3 followed or not by interval (à froid) appendectomy, is widespread. The main reason for this choice is avoidance of operating on a sick patient with a hazardous abdomen that could give rise to complications. Furthermore, nonoperative treatment has a good and extensively documented success rate, particularly after percutaneous drainage became possible.4 – 8 Most patients (71.4 %) in our clinic were also initially treated nonoperatively.
However, compared with operative management, nonoperative management requires time and patience, i.e., incapacitated and/or hospitalized patients and, in our study, multiple episodes of recurrent symptoms. In this study, 71.0 % of the nonintervention patients and 43.8 % of the patients who underwent percutaneous drainage experienced at least one recurrence and 53.3 % and 37.5 % ultimately underwent a surgical or radiological intervention, respectively. Another disadvantage of nonoperative treatment is that the actual pathology remains unclear. Unfortunately, a tumor is not an uncommon cause of an appendiceal inflammatory mass, and therefore, all patients managed nonoperatively should undergo colonoscopy as additional investigation. It is worrying that while most patients who were managed nonoperatively did not undergo colonoscopy follow-up; the overall rate of malignancy was 5.9 % (7 of 119 patients). Unfortunately, we do not have a conclusive explanation for why this investigation was not performed.
The abovementioned disadvantages of conservative treatment of an appendiceal inflammatory mass prompted surgeons to investigate its alternative - immediate surgery. Several investigators have reported morbidity to be similar to that after nonoperative management and have established the feasibility of operating on an appendiceal inflammatory mass.9 – 12 We also found an acceptable incidence of, mostly minor, complications (17.6 %) after immediate surgery. In the operative group, while the rate of extensive (ileocecal + hemicolonic) resection was 30.8 %, there were no recurrences, and the average length of stay was relatively short (9.2 days); few (5.9 %) patients had to be re-admitted, and a histopathological diagnosis was established in most (91.2 %) patients. We do not think that patients who undergo immediate surgery need a follow-up colonoscopy because the cecal area is thoroughly inspected and palpated during surgery, and resected tissue is sent for histopathological investigation, which should demonstrate or exclude malignancy.
So, the question remains: what is the recommended treatment for patients with an appendiceal inflammatory mass? Indirect investigations of the superiority of one treatment over the other have yielded inconsistent conclusions.13 – 17 Two recent meta-analyses1 , 18 favored nonoperative treatment, but the authors urged the readers to be cautious because the conclusion was based mainly on the findings of heterogenic retrospective studies with poorly or undefined study variables and no control group. A recent guideline19 addressing the matter relied on the same level of evidence. A prospective study might yield more persuasive evidence for the safety and efficacy of immediate surgery for an appendiceal inflammatory mass, but despite the agreement that such a study is necessary, it has not yet been performed.
We believe that our findings, namely, a high recurrence and intervention rate after nonoperative treatment, the low proportion of patients who receive adequate follow-up, and the high incidence of underlying malignancy indicate that nonoperative management of an appendiceal inflammatory mass is not an acceptable treatment option and that such patients should undergo immediate surgical treatment. Percutaneous drainage should probably only be used to reduce the risk of perioperative spread of pus and as a bridge to surgery for patients with sepsis or significant comorbidity. If nonoperative treatment is chosen, follow-up colonoscopy is mandatory to exclude malignancy.
References
Simillis C, Symeonides P, Shorthouse AJ, and Tekkis PP. A meta-analysis comparing conservative treatment versus acute appendectomy for complicated appendicitis (abscess or phlegmon). Surgery. 2010, Jun;147(6):818–29.
Ochsner AJ. Handbook of Appendicitis. Chicago: G.P. Engelhard & Company; 1902.
Bailey H. The Ochsner-Sherren (delayed) treatment of acute appendicitis: indications and technique. Br Med J. 1930, Jan 25;1(3603):140–3.
Oliak D, Yamini D, Udani VM, Lewis RJ, Vargas H, Arnell T, and Stamos MJ. Nonoperative management of perforated appendicitis without periappendiceal mass. Am J Surg. 2000, Mar;179(3):177–81.
Willemsen PJ, Hoorntje LE, Eddes EH, and Ploeg RJ. The need for interval appendectomy after resolution of an appendiceal mass questioned. Dig Surg. 2002;19(3):216–20; discussion 221.
Kumar S, and Jain S. Treatment of appendiceal mass: prospective, randomized clinical trial. Indian J Gastroenterol. 2004;23(5):165–7.
Tekin A, Kurtoğlu HC, Can I, and Oztan S. Routine interval appendectomy is unnecessary after conservative treatment of appendiceal mass. Colorectal Dis. 2008, Jun;10(5):465–8.
You KS, Kim DH, Yun HY, Jang LC, Choi JW, Song YJ, and Ryu DH. The value of a laparoscopic interval appendectomy for treatment of a periappendiceal abscess: experience of a single medical center. Surg Laparosc Endosc Percutan Tech. 2012, Apr;22(2):127–30.
Cunnigaiper ND, Raj P, Ganeshram P, and Venkatesan V. Does Ochsner-Sherren regimen still hold true in the management of appendicular mass? Ulus Travma Acil Cerrahi Derg. 2010, Jan;16(1):43–6.
Bahram MA. Evaluation of early surgical management of complicated appendicitis by appendicular mass. Int J Surg. 2011;9(1):101–3.
Shindholimath VV, Thinakaran K, Rao TN, and Veerappa YV. Laparoscopic management of appendicular mass. J Minim Access Surg. 2011, Apr;7(2):136–40.[cited 2012, Jul 4]
Kaya B, Sana B, Eriş C, and Kutaniş R. Immediate appendectomy for appendiceal mass. Ulus Travma Acil Cerrahi Derg. 2012, Jan;18(1):71–4.
Oliak D, Yamini D, Udani VM, Lewis RJ, Arnell T, Vargas H, and Stamos MJ. Initial nonoperative management for periappendiceal abscess. Dis Colon Rectum. 2001, Jul;44(7):936–41.
Senapathi PS, Bhattacharya D, and Ammori BJ. Early laparoscopic appendectomy for appendicular mass. Surg Endosc. 2002, Dec;16(12):1783–5.
Gibeily GJ, Ross MN, Manning DB, Wherry DC, and Kao TC. Late-presenting appendicitis: a laparoscopic approach to a complicated problem. Surg Endosc. 2003, May;17(5):725–9.
Arshad M, Aziz LA, Qasim M, and Talpur KA. Early appendicectomy in appendicular mass--a Liaquat University Hospital experience. J Ayub Med Coll Abbottabad. 2008; 20(1):70–2.
Aranda-Narváez JM, González-Sánchez AJ, Marín-Camero N, Montiel-Casado C, López-Ruiz P, Sánchez-Pérez B, et al. Conservative approach versus urgent appendectomy in surgical management of acute appendicitis with abscess or phlegmon. Rev Esp Enferm Dig. 2010, Nov;102(11):648–52.
Andersson RE, and Petzold MG. Nonsurgical treatment of appendiceal abscess or phlegmon: a systematic review and meta-analysis. Ann Surg. 2007, Nov;246(5):741–8.
Bakker OJ, Go PM, Puylaert JB, Kazemier G, Heij HA, and Werkgroup en klankbordgroup "Richtlijn acute appendicitis". [Guideline on diagnosis and treatment of acute appendicitis: imaging prior to appendectomy is recommended]. Ned Tijdschr Geneeskd. 2010;154A303.
Conflict of Interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Deelder, J.D., Richir, M.C., Schoorl, T. et al. How to Treat an Appendiceal Inflammatory Mass: Operatively or Nonoperatively?. J Gastrointest Surg 18, 641–645 (2014). https://doi.org/10.1007/s11605-014-2460-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-014-2460-1