
Abstract
Introduction
Complicated ventral hernias are often referred to tertiary care centers. Hospital costs associated with these repairs include direct costs (mesh materials, supplies, and nonsurgeon labor costs) and indirect costs (facility fees, equipment depreciation, and unallocated labor). Operative supplies represent a significant component of direct costs, especially in an era of proprietary synthetic meshes and biologic grafts. We aim to evaluate the cost-effectiveness of complex abdominal wall hernia repair at a tertiary care referral facility.
Methods
Cost data on all consecutive open ventral hernia repairs (CPT codes 49560, 49561, 49565, and 49566) performed between 1 July 2008 and 31 May 2011 were analyzed. Cases were analyzed based upon hospital status (inpatient vs. outpatient) and whether the hernia repair was a primary or secondary procedure. We examined median net revenue, direct costs, contribution margin, indirect costs, and net profit/loss. Among primary hernia repairs, cost data were further analyzed based upon mesh utilization (no mesh, synthetic, or biologic).
Results
Four-hundred and fifteen patients underwent ventral hernia repair (353 inpatients and 62 outpatients); 173 inpatients underwent ventral hernia repair as the primary procedure; 180 inpatients underwent hernia repair as a secondary procedure. Median net revenue ($17,310 vs. 10,360, p < 0.001) and net losses (3,430 vs. 1,700, p < 0.025) were significantly greater for those who underwent hernia repair as a secondary procedure. Among inpatients undergoing ventral hernia repair as the primary procedure, 46 were repaired without mesh; 79 were repaired with synthetic mesh and 48 with biologic mesh. Median direct costs for cases performed without mesh were $5,432; median direct costs for those using synthetic and biologic mesh were $7,590 and 16,970, respectively (p < .01). Median net losses for repairs without mesh were $500. Median net profit of $60 was observed for synthetic mesh-based repairs. The median contribution margin for cases utilizing biologic mesh was −$4,560, and the median net financial loss was $8,370. Outpatient ventral hernia repairs, with and without synthetic mesh, resulted in median net losses of $1,560 and 230, respectively.
Conclusions
Ventral hernia repair is associated with overall financial losses. Inpatient synthetic mesh repairs are essentially budget neutral. Outpatient and inpatient repairs without mesh result in net financial losses. Inpatient biologic mesh repairs result in a negative contribution margin and striking net financial losses. Cost-effective strategies for managing ventral hernias in a tertiary care environment need to be developed in light of the financial implications of this patient population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Abdominal wall hernia is one of the most challenging problems faced by the general surgeon. Over 2 million laparotomies are performed in the USA each year.1 With an incidence of 11–20 % based on long-term studies, incisional hernia is an extraordinarily common problem.2,3 Even after prosthetic mesh repair, dismal recurrence rates are reported in the literature, and many patients require multiple repairs, facing a higher likelihood of recurrence with each repair.4,5 This leads to increasing associated morbidity and a rising cumulative burden on healthcare costs.
As these cases become more technically challenging, often in patients with numerous co-morbid conditions, many are referred to tertiary care centers. Costs associated with management of these complex patients appear to be rising, despite increasing pressure for healthcare cost containment.6 The purpose of this study is to analyze hospital finances related to open ventral incisional hernia repair at a major academic medical center.
Methods
We queried our operating room scheduling system (Picis, Inc, Wakefield, MA) for both inpatient and outpatient open ventral incisional hernia repairs (VIHR) performed at our tertiary referral facility (University of Kentucky Medical Center) between 1 July 2008 and 31 May 2011 (CPT codes 49560, 49561, 49565, and 49566). We then examined hospital revenue and costs for these admissions from the hospital cost accounting system (Alliance for Decision Support, Avega Health Systems Inc, El Segundo, CA). Financial data related to any readmissions after the initial hospitalization at the time of surgery were not included. We grouped cases as inpatient or outpatient admissions and by whether the hernia repair was the primary or a secondary procedure during the stay. For example, a concomitant intestinal resection during a hernia repair or at any time during the same hospitalization would result in the hernia being listed as secondary. Twenty-six cases with diagnosis-related group (DRG) for tracheostomy and one case with DRG for liver transplant were excluded as these skewed cost and reimbursement data.
For primary repairs, we examined financial performance relative to mesh utilization (no mesh, synthetic, or biologic). Financial performance metrics included hospital net revenue, direct costs (with a breakout of operating room supply costs, which includes cost of mesh materials), contribution margin, indirect costs, and net profit. Hospital revenue in the accounting system includes the increased revenue associated with adjustments for co-morbid conditions and DRGs. Direct costs are those costs directly attributable to a particular patients’ care by the cost accounting system; they include most nursing and technical labor costs, supplies, and most room costs. Indirect costs include overhead costs such as facilities, large equipment depreciation, unallocated labor, and management costs. The contribution margin is the net revenue minus direct costs.
Financial metrics and length of stay were compared between groups using nonparametric Mann–Whitney U tests and Kruskal–Wallis tests. The threshold for significance was set at p < 0.05. SPSS™ statistics software (IBM Corp, Hawthorne, NY) version 19 was used for all calculations.
Results
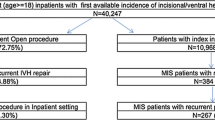
Four hundred and fifteen patients underwent open VIHR; the majority of these repairs took place in the inpatient setting (Fig. 1). Among inpatients, 173 underwent VIHR as the primary procedure. In the remaining 180, VIHR was listed as a secondary procedure. As shown in Table 1, hospital length of stay was longer in those undergoing hernia repair as a secondary procedure, and median net revenue was significantly higher as well ($17,310 vs. 10,360, p < 0.001). Median direct costs associated with VIHR as a secondary procedure were essentially double those observed when hernia repair was the primary procedure ($16,050 vs. 8,610, p < 0.001). Net financial losses were observed in both groups. In spite of greater median net revenue, net losses were significantly greater for those undergoing VIHR as a secondary procedure (3,430 vs. 1,700, p < 0.025).

Breakdown of open ventral incisional hernia repairs (VIHR) performed at the University of Kentucky Medical Center from 1 July 2008 through 31 May 2011
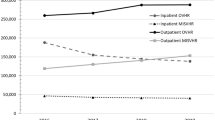
Financial results with respect to overall mesh utilization are listed in Table 2. Inpatient mesh utilization increased over the course of the study (Fig. 2). Financial metrics categorized by mesh utilization for inpatient open VIHR listed as the primary procedure are outlined in Table 3. Median direct costs for cases performed without mesh were $5,424; these figures increased significantly when synthetic and biologic meshes were employed. A concomitant increase in median net revenue was also observed with the use of mesh. A positive median contribution margin was observed in nonmesh repairs and in those undergoing synthetic mesh-based repairs. A median net financial loss of $500 was observed in repairs without mesh. Synthetic mesh-based repairs yielded a median net profit of $60.

Inpatient mesh utilization by year for primary open ventral hernia repair
Median direct costs associated with biologic mesh repairs reached $16,970, resulting in a negative median contribution margin of $4,560. Ultimately, a median net financial loss of $8,370 was observed in these patients. When examining the breakout of operating room supply costs as a component of direct costs, a significant difference was noted between synthetic and biologic mesh repairs ($1,830 vs. 10,230, p < 0.001). Specific biologic grafts and synthetic meshes used in these patients by size and type, along with their average costs and number of times charged, are highlighted in Table 4.
Out of 62 outpatients, open VIHR was listed as the primary procedure in 46. Biologic mesh was not utilized in any outpatient repairs. Financial metrics for these outpatients categorized by mesh utilization are shown in Table 5. Use of mesh in these patients was associated with a negative contribution margin. Median net losses of $1,560 and 230 were observed in patients undergoing repair with and without synthetic mesh, respectively.
Overall cumulative hospital readmission data up to a year of postsurgery are summarized in Fig. 3. Overall readmission rates were 24 % (100 patients) at 30 days, 40 % (167 patients) at 90 days, and 55 % (229 patients) at 1 year. Figure 4 highlights hospital readmission data by mesh utilization. The 30-day readmission rate for patients undergoing biologic mesh repair was 33 % (41/123 patients), compared with 18 % (21/117 patients) for synthetic mesh and 22 % (38/175 patients) for cases in which mesh was not utilized.

Percent overall cumulative hospital readmissions

Percent cumulative readmissions by mesh utilization
Discussion
Complicated ventral hernias are often referred to experienced high-volume centers due to the technical challenge posed by these operations. Likewise, patients with numerous co-morbid conditions are frequently referred as multidisciplinary care resources are more readily available in these centers. Previous studies have examined the impact of preoperative risk factors and surgical complexity on hospital costs. In a National Surgical Quality Improvement Program (NSQIP) database study published from our institution in 2005, preoperative risk factors and surgical complexity (characterized by work relative value units) together predicted 49 % of cost variation in 5,875 patients on a total of six different surgical services.7 Similarly, a more recent NSQIP database study demonstrated increasing complications as preoperative functional health status declined from independent to partial and total dependence.8 When operative management is favored, many of these patients are treated in tertiary referral centers. While this study did not focus on costs, preoperative status clearly affects outcomes and hospital costs in this frail patient population. Our data show significantly greater median direct costs in patients undergoing ventral hernia repair as a secondary procedure compared with primary procedure ($16,050 vs. 8,610, p < 0.001). Net financial losses were significantly greater in these patients ($3,430 vs. 1,700, p < 0.025). This is likely a result of the higher degree of operative complexity involved when a concomitant procedure is required. These financial metrics demonstrate the need for more appropriate risk adjustment by payers and regulatory agencies. Reimbursement strategies for patients undergoing ventral hernia repair should be re-evaluated in light of preoperative risk factors, functional health status, and operative complexity.
Few studies in the literature have focused on the financial implications of VIHR. Earle and colleagues examined prospectively collected administrative data at a major academic medical center to compare costs between laparoscopic and open incisional hernia repair techniques.9 In a study of 884 cases performed between 1999 and 2004, laparoscopic repair was associated with lower total hospital costs ($6,396 vs. 7,197). These data effectively show that laparoscopic repair does not increase costs, but it is difficult to compare these monetary values to our cost data. While our study focused solely on incisional hernias, these data also includes umbilical, epigastric, spigelian, and parastomal defects. Differing reimbursement for these various types of hernias potentially undermines appropriate cost comparison. Furthermore, the lack of differentiation between inpatient versus outpatient repairs and the lack of appropriate adjustment for inflation to figures consistent with the time period of our study confound comparison. Standardized cost estimates for surgical procedures are elusive and this presents difficulty in comparison across published studies.
In an attempt to more adequately define the scope and cost of ventral hernia repair in the USA, a recently published study examined the cumulative incidence and estimated costs of both inpatient and outpatient ventral hernia repairs using data from the 2001–2006 Healthcare Cost and Utilization Project Nationwide Inpatient Sample and the 2006 Center for Disease Control National Survey of Ambulatory Surgery. Cost figures were adjusted to 2010 US dollars using the Consumer Price Index for Healthcare. Based on their 2006 data, 348,000 combined inpatient and outpatient ventral hernia repairs are performed annually (not including repairs performed in the Federal/Veterans Affairs system). A significantly higher number of inpatient repairs were performed each year from 2003 to 2006, and costs for inpatient repairs increased annually from 2001 to 2006. Estimated third party payer cost for an inpatient ventral hernia repair was $15,899 and 3,873 for an outpatient repair (2010 US dollars).6
While these figures are comparable to hospital net revenue values observed in our study for inpatient and outpatient open VIHR, several caveats accompany this comparison. First, this analysis was not limited to incisional hernias but based on International Classification of Diseases, Ninth Revision, Clinical Modification codes for the entire spectrum of ventral hernias (umbilical, epigastric, parastomal, etc). Second, there is no differentiation in this study between mesh and nonmesh repairs. Furthermore, this study used data sources that allow cost evaluation on a national level; regional variation in costs may potentially complicate comparison of these values with our single-center study. Nonetheless, these figures are perhaps the most appropriate cost estimates available for comparison to our data.6 This important study clearly highlights the problem of rising costs in patients undergoing ventral hernia repair and makes a solid case for funding of hernia research.
Our data provide an important insight into the extent of mesh utilization for VIHR. The superiority of open mesh repair to suture repair has been clearly established in a randomized controlled trial from the Netherlands. This group demonstrated a 3-year recurrence rate of 43 % for suture repair compared with 24 % for mesh repair. Similarly, 10-year recurrence rates were 63 % and 32 % for suture repair and mesh repair, respectively.4,10 An additional landmark study using a Washington state hospital discharge database containing over 10,000 patients demonstrated high cumulative rates of reoperative incisional hernia repairs with a 24.1 % higher hazard for recurrence if no mesh was used.5 In spite of these convincing studies, systematic use of mesh for incisional hernia repair is yet to be achieved. As shown in Fig. 2, while mesh utilization increased over the course of the study, it was not employed uniformly, as it was used in only 80 % of cases in 2011.
Pressure for cost containment in today’s healthcare climate is a potential barrier to the uniform use of mesh in VIHR. The lower risk of recurrence with open mesh repair must be carefully weighed against higher costs and the potential for mesh-related complications. Finan and colleagues were able to construct a decision analysis model from the payer’s perspective for comparison of cost-effectiveness between open suture versus mesh repair of primary incisional hernias. All costs associated with incisional hernia repair and treatment of a first recurrence, to include complications and the subsequent operation for recurrence, were derived from 2005 Medicare reimbursement rates. Probabilities for complications and outcomes were derived from the literature. The overall model cost for open suture repair was $16,355 compared with $16,889 for open mesh repair. The suture repair group incurred 58.1 % more recurrences than the mesh repair group. The incremental cost to prevent one recurrence by the placement of polypropylene mesh (incremental cost effectiveness ratio) was $1,878. When the model focused only on hernia defects less than 10 cm2 in size, the overall model cost for mesh repair was less than suture repair. The authors concluded that open mesh repair is overall a more cost-effective treatment than suture repair, with a lower risk of recurrence at a small cost to the payer.11 A similar retrospective cost analysis from Sweden examined 44 patients who underwent either open suture or mesh repair. In addition to hospital costs, this study incorporated the societal impact in terms of sick leave costs. Although higher costs were incurred in the operating theatre, mesh repair was overall found to be less costly than suture repair.12 While mesh use is associated with higher direct costs, its global value in the treatment of incisional hernia is clear. This is underappreciated in current reimbursement strategies.
Our results highlight the economics of open VIHR at a major academic medical center. To our knowledge, this is the first study to systematically evaluate hospital net revenue and profits/losses in the context of open VIHR. Inpatient synthetic mesh based repairs performed as the primary procedure were essentially budget-neutral, yielding a modest median net profit of $60. All other groups were found to result in net financial losses for the hospital. Inpatient biologic mesh based repairs performed as the primary procedure were found to have a negative median contribution margin of $4,560. These repairs ultimately resulted in a striking median net financial loss of $8,370. When examining the breakout of operating room supply costs as a component of direct costs, a significant difference was noted between synthetic and biologic mesh repairs ($1,830 vs. 10,230, p < 0.001). Mesh materials represent a significant component of operating room supply costs. In this study, operating room supply costs are perhaps the most directly attributable reason for the net financial losses observed in patients undergoing biologic mesh-based repair.
The use of biologic mesh has previously been implicated in the rising cost of VIHR. In a previously mentioned epidemiologic study, Poulose et al documented increasing costs for inpatient repairs from 2001 to 2006, a period of time when biologic meshes were increasing in popularity.6 Furthermore, biologic grafts were found to be a significant cost contributor in a retrospective comparison between open and endoscopic techniques for component separation. In this analysis, all patients undergoing open component separation were repaired with biologic mesh; median mesh costs were significantly higher in this group compared with the endoscopic group ($8,415 vs. 733, p = 0.05). Median cumulative direct costs (assessed at index hospitalization and at 3 and 6 months postsurgery) were significantly higher in the open group ($20,326 vs. 12,528, p = 0.05). Along with the increased wound morbidity observed in the open group, the authors concluded that the use of biologic mesh was a significant contributor to the increased costs seen in patients undergoing open component separation.13
Pinpointing the actual cost of different biologic meshes is difficult due to individual hospital contracts and regional variations. Nevertheless, these products are known to be very expensive. Although there are proponents of synthetic mesh use in clean-contaminated and contaminated wounds,14 their use in these scenarios is generally felt to be contraindicated. Likewise, biologic meshes are thought by many surgeons to be the material of choice in contaminated or infected fields. Since their introduction approximately a decade ago, biologic grafts have gained widespread acceptance in spite of little scientific evidence supporting their use in these clinical scenarios. In fact, most available data for these materials stems from industry sponsored studies. While biologic meshes have certainly given the hernia surgeon more options for complex abdominal wall reconstruction, their use should be considered carefully. In light of their financial implications in our study, more comprehensive research is needed to clearly define appropriate indications and expectations for the use of these biologic materials.15
Several limitations of this study must be considered. First, a breakdown of the payer mix was not performed. While it would be interesting to examine this distribution, our data provide a collective representation of hospital revenue associated with the patient population undergoing VIHR at a tertiary referral center. Second, because the study is based solely on a search for CPT codes, we have no information regarding hernia defect size and other potential complicating factors. However, because our median net revenue values reflect adjustments carried out for co-morbid conditions and DRGs, we believe that these numbers are fairly reliable. In patients undergoing component separation, a breakdown of endoscopic versus open technique was not possible. This could skew costs in terms of wound complications. While procedure coding is given careful attention due to its importance in billing, the potential for coding errors exists. For instance, the CPT codes for laparoscopic ventral hernia repair (49652, 49653, 49654, 49655, 49656, and 49657) were introduced in 2009. Given the time period of our study, it is certainly possible that some repairs may have been coded incorrectly. Finally, costs associated with hospital readmissions were not included in the study. As shown in Fig. 4, there appeared to be a trend towards higher postoperative readmission rates in patients undergoing repair with biologic mesh. This further illustrates the higher costs involved in managing these complex patients. Omission of financial metrics related to hospital readmissions leads to an underestimation of hospital costs in our analysis.
A further limitation is that this is a single center study at a tertiary referral center. Although we believe this data is likely similar at other academic institutions, it is unclear whether it is applicable to community-based hospitals. Community hospitals often operate on a significantly lower fixed cost base and thus likely experience lower indirect costs. Due to volume, product standardization, and aggressive contractual agreements with vendors, direct costs at tertiary centers are kept to a minimum. At best, direct costs at community hospitals would be similar, though they are likely to be higher because of lower overall volume. Community-based facilities may represent an ideal environment for repairing certain hernias that do not demand the resources of a tertiary referral center. Nonetheless, biologic mesh repairs are occurring at a loss, irrespective of indirect costs, and these would still result in net financial losses at a community hospital.
In summary, at our tertiary referral center, the vast majority of open VIHRs are performed at a financial loss for the hospital. Inpatient synthetic mesh-based repairs performed as the primary procedure were budget-neutral, but all other groups resulted in net financial losses. Inpatient biologic mesh-based repairs resulted in a sizable negative median contribution margin of $4,560, and a median net financial loss of $8,370. Operating room supply costs (including biologic mesh materials) are the most directly attributable reason for the net financial losses observed in this group of patients. While mesh utilization is associated with higher direct costs, its role in decreasing hernia recurrence adds to its global cost-effectiveness, and this should be considered in reimbursement strategies. There are certain clinical scenarios in which the patient is best served with a biologic graft for abdominal wall reconstruction, especially in the tertiary care environment. Biologic mesh adds significant costs, and this should be thoughtfully considered when utilizing these materials.
To the extent that reasonable comparison can be made, our cost figures are consistent with other published studies, and it is likely that similar financial plight is experienced at other tertiary centers serving these patients. These net financial losses are not sustainable. More cost-efficient strategies need to be implemented in managing this complex group of patients. There is significant need for re-evaluation of reimbursement strategies, with more appropriate adjustment for preoperative risk factors and operative complexity.
References
Wechter ME, Pearlman MD, Hartmann KE. Reclosure of the disrupted laparotomy wound; a systematic review. Obstet Gynecol 2005;106:376–383.
Mudge M, Hughes LE. Incisional hernia: a 10-year prospective study of incidence and attitudes. Br J Surg 1985;72:70–71.
Cengiz Y, Israelsson LA. Incisional hernias in midline incisions: an eight-year follow up. Hernia 1998;2:175–177.
Burger JW, Luijendijk RW, Hop WC, Halm JA, Verdaasdonk EG, Jeekel J. Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 2004;240:578–583.
Flum DR, Horvath K, Koepsell T. Have outcomes of incisional hernia repair improved with time? A population-based analysis. Ann Surg 2003;237:129–135.
Poulose, BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Beck W, Holzman MD. Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 2012;16:179–183.
Davenport DL, Henderson WG, Khuri SF, Mentzer RM Jr. Preoperative risk factors and surgical complexity are more predictive of costs than postoperative complications: a case study using the National Surgical Quality Improvement Program (NSQIP) Database. Ann Surg 2005;242:463–468.
Albright EL, Davenport Dl, Roth JS. Preoperative functional health status impacts outcomes after ventral hernia repair. Am Surg.2012;78:230–234.
Earle D, Seymour N, Fellinger E, Perez A. Laparoscopic versus open incisional hernia repair: a single institution analysis of hospital resource utilization for 884 consecutive cases. Surg Endosc 2006;20:71–75.
Luijendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, Ijzermans JN, Boelhouwer RU, de Vries BC, Salu MK, Wereldsma JC, Bruijninckx CM, Jeekel J. A comparison of suture repair with mesh repair for incisional hernia. N Eng J Med 2000;343:392–398.
Finan KR, Kilgore ML, Hawn MT. Open suture versus mesh repair of primary incisional hernias: a cost-utility analysis. Hernia 2009;13:173–182.
Israelsson LA, Jönsson L, Wimo A. Cost analysis of incisional hernia repair by suture or mesh. Hernia 2003;7:114–117.
Harth C, Rose J, Delaney CP, Blatnik JA, Halaweish I, Rosen MJ. Open versus endoscopic component separation: a cost comparison. Surg Endosc 2011;25:2865–2870.
Kelly ME, Behrman SW. The safety and efficacy of prosthetic hernia repair in clean-contaminated and contaminated wounds. Am Surg 2002;68:524–528.
Rosen MJ. Biologic mesh for abdominal wall reconstruction: a critical appraisal. Am Surg 2010;76:1–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. Daniel J. Deziel (Chicago,IL): Dr. Reynolds and colleagues have painted a discouraging financial profile for ventral hernia repair which would become even more grim if the cost of readmissions was added. Related readmissions yield, at best, only commodity level returns and are not in the financial core. Two primary drivers of direct cost were use of mesh, particularly biologic mesh, and length of stay. Perhaps you could clarify whether the mesh cost figures were actual institutional costs or patient charges. Since there is no consensus on the specific value of various biologics, have you done anything to standardize use of these expensive products? With the exception of biologic mesh, all hernia repair categories would have been money makers before indirect costs. Indirect costs are allocated differently at different medical centers and within medical centers. Your indirect costs ranged up to 58 % of direct cost and up to nearly 800 % of OR supply cost (from tables in manuscript). Is an excess of overhead being misallocated to these patients?
Thank you for the privilege of discussion.
Closing Discussant
Dr. Drew Reynolds: Thank you, Dr. Deziel, for your comments and thoughtful critique of our manuscript. To begin with, I wholeheartedly agree with your assessment of the bleak financial picture. I believe it is appropriate to assume that if the cost of readmissions were included, the financial picture would be even more dismal. Analysis of cost data related to readmissions is an area of further investigation for our group. Biologic mesh materials were a significant driver of cost in this analysis. To answer your question, we used actual hospital costs and did not evaluate hospital charges, as these numbers are often inflated and individual insurance contracts result in different negotiated rates. Additionally, in an era of DRG-based hospital reimbursement, actual hospital charges are frequently irrelevant as reimbursements are based upon contractual agreements for the vast majority of patients. With respect to standardization of mesh use, as of 2009, a contractual agreement was made with one company (BARD). And most of the meshes used at our facility are their products. And we only use biologic grafts for ventral hernia when we feel that a synthetic is contraindicated. Indirect costs include overhead depreciation, enterprise transfers, goods and services, and personnel, and are based on direct costs. We agree that contribution margin is a more relevant number in looking at these finances, but hospitals still need to cover indirect costs to remain fiscally solvent. With the help of our finance staff, we have investigated the methodology associated with assigning these indirect costs to each patient and feel that in fact the calculations are appropriate.
Based upon selection, this manuscript was presented as an oral presentation at Digestive Disease Week 2012 in San Diego, California
Rights and permissions
About this article
Cite this article
Reynolds, D., Davenport, D.L., Korosec, R.L. et al. Financial Implications of Ventral Hernia Repair: A Hospital Cost Analysis. J Gastrointest Surg 17, 159–167 (2013). https://doi.org/10.1007/s11605-012-1999-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-012-1999-y