
Abstract
Introduction
Matrix metalloproteinase-21 (MMP-21) is a member of the MMP family, which is overexpressed in some solid tumors and is thought to enhance the tumor invasion and metastasis ability. The aim of the present study is to examine the MMP-21 expression in human colorectal cancer and normal colorectal tissue using tissue microarray technique and to determine its association with clinicopathological characteristics and prognostic value.
Materials and Methods
Four array blocks including 256 cases of colorectal cancer and adjacent normal tissues were investigated by immunohistochemistry assay. Staining evaluation results were analyzed statistically in relation to various clinicopathological characters and overall survival.
Results
High level of MMP-21 expression was detected in colorectal cancer, significantly more than in normal colorectal epithelial cells. In colorectal cancer, MMP-21 was significantly positively correlated with depth of invasion, lymph node metastasis, and distant metastasis. The overall survival rate was significantly lower for patients with MMP-21 positive than those with MMP-21 negative tumors. However, no correlations between MMP-21 expression and patients’ age, sex tumor location, or differentiation status were detected.
Conclusion
Our findings emphasize the important role of MMP-21 in the invasion and metastasis process in human colorectal cancer. It might also serve as a novel prognostic marker that is independent of, and additive to, the TNM staging system.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer is one of most common malignant tumors in China and is the fifth most frequent cause of cancer-related death.1 In 2007, 153,760 cases of colorectal cancer were diagnosed, and 78,700 people died from the disease in China. Despite earlier diagnosis, progressions in radical surgery, radiotherapy, and neoadjuvant chemotherapy, many colorectal cancers remain incurable. In the last decades, the incidence and mortality of colorectal cancer in China have even been increasing due to the early metastases.2–5 The prognosis of colon cancer was directly correlated with the extent of tumor invasion and metastases.6 How to diagnose and prevent early tumor metastasis was one of the most important topics in recent tumor studies. Colorectal cancer initiation and progression are associated with stepwise genetic alterations. Molecules involved in cancer recurrence and metastasis might serve as markers for early detection of metastasis and prognostic judgment.7,8
Matrix metalloproteinases (MMPs) are a group of zinc-dependent proteins that are found in the extracellular milieu of various tissues.9 They are a multigene family of highly homologous enzymes sharing a similar structure, involved in extracellular matrix (ECM) proteins7-10 remodelling processes.10–13 To date, at least 26 human MMPs have been discovered.14 Based on sequence homology and substrate specificities, the MMPs can be divided into several distinct subclasses: collagenases, gelatinases, stromelysins, and matrilysins.15 MMPs are frequently overexpressed in various human cancers and have long been associated with malignancy.16–18 However, MMPs exhibit considerable promiscuity with respect to their substrates, leading to various redundancies in biological functions.19 There has been a great deal of interest in the role of MMPs in cancer invasion and metastasis due to their ECM-degrading capacity. To invade and metastasize, tumor cells must infiltrate blood vessels and lymphatics. A substantial subsequent body of work has provided evidence for an association between MMP expression and tumor aggressiveness.20 In colorectal cancer, 72-kDa gelatinase A (MMP-2), 92-kDa gelatinase B (MMP-9), matrilysin (MMP-7), and stromelysin-3 (MMP-11) were reported to be overexpressed.20–25 It has also been proven and widely accepted that MMPs expression, such as MMP-2 and MMP-9, were up-regulated in colorectal cancer.26–32 However, the expression and function of MMP-21, a recently discovered molecule, has not been described in colorectal cancer yet. To date, MMP-21 has been reported up-regulated and related to progression of human malignancy such as ovarian cancer, breast cancer, squamous cell carcinomas and melanoma.33–36
In this present study, we investigated the protein expression of MMP-21 and explored the possible relationship to clinical features and overall survival in a large scale of colorectal cancer patients who had not received neoadjuvant chemotherapy.
Materials and Methods
Patients and Specimens
This study was approved by the ethics committee of the Fourth Military Medical University. Fresh colorectal carcinoma specimens and patient-matched adjacent tissues were collected from 256 patients in the Department of Gastrointestinal Surgery of Xijing Hospital at the Fourth Military Medical University (Xi’an, China) between October 2000 and November 2003. Only patients that did not receive neoadjuvant chemotherapy were recruited. Histomorphology of all the primary tumors specimens and regional lymph nodes were confirmed with hematoxylin–eosin staining according to the International Union against Cancer TNM classification by the Department of Pathology, Xijing Hospital at the Fourth Military Medical University (Xi’an, China). Clinical parameters such as gender, age, differentiation status, lymph node metastasis, and TNM stage were collected. Complete follow-up was made available for at least 5 years. In the follow-up period, overall survival was measured from diagnosis to death or last follow-up. Follow-up information of all participants was updated every 3 months by telephone visit and questionnaire letters. Death of participants was ascertained by reporting from the family and verified by review of public records. All specimens were fixed in 10% formalin, embedded in paraffin, and 4-μm serial sections were examined by immunohistochemistry.
Immunohistochemistry Assay
Immunohistochemistry was performed by the avidin–biotin–peroxidase method on all the 256 colorectal cancer tissue specimens. All sections were deparaffinized in xylene and dehydrated through a graduated alcohol series before endogenous peroxidase activity was blocked with 0.5% H2O2 in methanol for 10 min. Without washing, sections were incubated with rabbit polyclonal MMP-21 antibody (1:200) in PBS at 4°C overnight in a moist box. Negative controls were performed by replacing the primary antibody with pre-immune rabbit serum. Biotinylated anti-rabbit IgG (1:400, Sigma) was incubated with the sections for 1 h at room temperature and detected with a streptavidin–peroxidase complex. The brown color, indicative of peroxidase activity, was obtained by incubating with 0.1% 3,3-diaminobenzidine (Sigma) in PBS with 0.05% H2O2 for 5 min at room temperature. Images were obtained under a light microscope (Olympus BX51, Olympus, Japan) equipped with a DP70 digital camera.
Evaluation of Staining
The MMP-21 staining was viewed separately by two pathologists without knowing the clinical or clinicopathological status of the cases. The expression of MMP-21 on tissue microarray was evaluated by scanning the entire tissue specimen under low-power magnification (×40), and then confirmed under high-power magnification (×200 and ×400). An immunoreactivity score system was applied. The extensional standard: (1) number of positive stained cell ≤ 5% scored 0; 6∼25% scored 1; 26∼50% scored 2; 51∼75% scored 3; >75% scored 4. (2) Intensity of stain: colorless scored 0; pallide-flavens scored 1; yellow scored 2; brown scored. (3) Multiply (1) and (2). The staining score was stratified as − (0 score, absent), + (1∼4 score, weak), ++ (5∼8 score, moderate), and +++ (9∼12 score, strong) according to the proportion and intensity of positively stained cancer cells. Specimens will be rescored if the difference of scores from two pathologists was more than 3.37–39
Statistical Analysis
Associations between Notch1 expression and categorical variables were analyzed by X 2 test or Fisher’s exact test, as appropriate. Associations between MMP-21 expression and clinicopathological characteristics were analyzed by the Mann–Whitney and Kruskal–Wallis tests. Survival curves were estimated using the Kaplan–Meier method and differences in survival distributions were evaluated by the log-rank test. Cox’s proportional hazards modeling of factors potentially related to survival was performed in order to identify which factors might have a significant influence on survival, and controlling for age, gender, and differentiation status. Differences with a P value of 0.05 or less were considered to be statistically significant.
Results
Immunohistochemical Detection of MMP-21
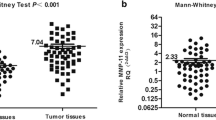
In the immunohistochemistry assay, 256 cases of normal and colorectal cancer tissues were investigated. MMP-21 staining mainly located in cytoplasm of tumor cells. The negative staining (−) of MMP-21 were detected in 89 samples of colorectal cancer, the weakly positive staining (+) of MMP-21 was detected in 75 samples, the moderate positive staining (++) of MMP-21 was detected in 58 samples and the strong positive staining (+++) of MMP-21 was detected in 34 samples of colorectal cancer. In contrast, only 5 strong positive stainings (+++) of MMP-21 was detected in normal colorectal tissues, 16 moderate positive stainings (++), 21 weakly positive stainings (+), and 214 negative stainings (−) of MMP-21 were detected. The difference of MMP-21 staining between normal epithelium and colorectal cancer tissues is statistically significant (P < 0.05).
The Relationship of MMP-21 to Clinicopathological Characteristics
According to the statistical results immunohistochemical assay, the correlation between the MMP-21 expression and clinicopathological characteristics is shown in Table 1. In colorectal cancer samples with different invasion status, the expression of MMP-21 tends to increase from T1 to T4 (P < 0.001). Although no significant differences were detected between colorectal cancer (CRC) samples with T1 and T2 (P = 0.656); statistical differences were observed between T2 and T3 (P = 0.005), T1 and T4 (P < 0.001), T2 and T4 (P < 0.001), T3 and T4 (P = 0.017). Then, we analyzed the relation between MMP-21 expression and node status. As a result, colorectal cancer samples with positive lymph node metastasis tended to have more MMP-21 positive expression than node negative ones (P < 0.001). As far as distant metastasis was concerned, colorectal cancer samples with distant metastasis had more positive staining of MMP-21 than M0 ones. MMP-21 was also detected to be increased with TNM stage. The expression of MMP-21 was not correlated to patient’s gender, age, tumor location, or differentiation status.
The Relationship of MMP-21 to Overall Survival
The mean follow-up time of patients in the study cohort was 72.8 months with median follow-up time of 64.2 months, and the 5-year survival rate of 192 patients was 54.7%. Kaplan–Meier postoperative survival curve was used to evaluate the overall survival rate of patients with colorectal cancer and MMP-21 expression (Fig. 1, log-rank test, P = 0.001). The postoperative median overall survival time of all patients with colorectal cancer cannot be estimated due to good overall survival. The median survival time of patients with strong positive (+++) and moderate positive (++) expression of MMP-21 was 30 months (95% CI, 18–42) and 43 months (95% CI, 35–51; log-rank test, P < 0.05). The median survival time of patients with weak positive (+) and negative expression of MMP-21 cannot be estimated either. Unadjusted hazard ratio (HR) set 1.00 as reference in MMP-21 negative (−) expression group, the unadjusted HR of weak positive (+), moderate positive (++) and strong positive (+++) groups were 3.15 (95% CI, 1.61–6.18; P < 0.05), 6.13 (95% CI, 3.09–12.15; P < 0.001) and 7.71 (95% CI, 5.10–18.48; P < 0.001), respectively. Moreover, differentiation status (log-rank test, P < 0.001), lymph node metastasis (log-rank test, P < 0.001) and TNM stage (log-rank test, P < 0.001) were also proved to be prognostic factors for overall survival of patients with colorectal cancer. Patients with positive lymph node metastasis or vascular invasion had shorter overall survival. However, sex, age, differentiation status or vascular invasion had no prognostic value on overall survival of patients with colorectal cancer. Unadjusted HR was shown in Table 2.

Kaplan–Meier postoperative survival curve for patterns of patients with gastric cancer and MMP-21 expression
Cox proportional hazards model adjusted for age, gender, differentiation, tumor location and TNM stage were shown in Table 2. In multivariate analysis, TNM stage and MMP-21 expression were two independent prognostic factors. Adjusted HR was 1.00 (as a reference) in MMP-21 negative (−) expression group, the adjusted HR of weak positive (+), moderate positive (++), and strong positive (+++) groups were 3.41, 3.58, and 6.12, respectively. Thus, MMP-21 could be an independent predictor of survival for patients with colorectal cancer. In addition, there was no significant correlation between age, gender, or differentiation distribution and survival in the patients.
Discussion
Colorectal cancer is one of the most common malignant tumors all over the world. One of the greatest challenges in colorectal cancer management is to accurately predict outcome for each patient so that we can determine who will benefit from adjuvant therapy. To achieve this, presently, people rely heavily on traditional pathologic variables, such as tumor size, lymph node status, and tumor grade. Currently, TNM and Dukes’ staging system of tumors is the gold standard for determining prognosis in patients with colorectal cancer; whereas the staging system, relying on the extent of disease at the time of diagnosis, is less informative for each individual patient. Patients with similar stages of disease even showed a big discrepancy in survival. Although several new molecular prognostic factors such as P53 and KRAS mutations are being evaluated in the hope that they may contribute to better assessment of the survival probability. It is still not possible to accurately predict the prognosis of patients following surgery and consequently to make tailored treatment for each individual patient.40
Neoadjuvant chemotherapy prior to surgery has been proven to alter MMPs expression such as MMP-9.41,42 It might due to the effects of 5-fluorouracil on NF-κB activity which can regulate MMPs in human malignancy.43–45 Neoadjuvant chemotherapy prior to surgery can alter not only MMPs expression but also postoperative survival time, thus inevitably raise a higher possibility to generate false-negative results. It has been proved that, compared with patients who did not receive 5-Fu based chemotherapy, patients treated with 5-Fu would lose the prognostic value of MMP-9.46 Therefore, only patients who had not received neoadjuvant chemotherapy were recruited in our present study in order to diminish the influence of the neoadjuvant on MMPs and survival of patients.
The primary aim of this study is to determine the MMP-21 expression and the relation to clinicopathological characteristics and prognosis of patients. As a result, we confirmed a significant elevated expression level of MMP-21 in this cohort of colorectal cancer compared to adjacent normal tissues. Moreover, MMP-21 was highly expressed with depth of invasion, especially in T4 carcinomas, since statistical differences were detected between T1/T2/T3 and T4 tumors, suggesting the role of the MMP-21 involved in the breakdown the ECM, which is important for the invasion of solid tumor. As far as lymph node status and distant metastasis were concerned, both node-positive and distant-metastasis-positive CRC samples tend to show elevated MMP-21 expression. However, its expression was not correlated with age, gender, tumor location, or tumor differentiation. In this perspective, MMP-21 expression may increase as tumor invades, suggesting the possible role of MMP-21 in the invasion and metastasis process of CRC. Kaplan–Meier analysis of the survival curves showed a significantly worse overall survival for patients whose tumors had high MMP-21 levels (log-rank test P = 0.001), indicating that high MMP-21 tumor protein level is a marker of poor prognosis for patients with colorectal cancer. Cox proportional hazards model adjusted for age, gender, tumor location, differentiation status and TNM stage showed the same trend as Kaplan–Meier postoperative survival curve. Moreover, multivariate analysis showed MMP-21 expression to be a marker of worse outcome independent of the known clinical prognostic indicators such as TNM stage. These data suggested that MMP-21 expression was correlated with worse outcome and might be an independent prognostic factor for patients with colorectal cancer. It could constitute a useful prognostic marker additive to the TNM staging system for these patients, identifying patients that are more likely to have disease recurrence and are, thus, good candidates to receive an aggressive adjuvant chemotherapeutic treatment.
Our study provides first evidence that MMP-21 expression is elevated in primary CRC and related to tumor invasion, metastasis, and prognosis. Although prospective studies will be needed to determine the prognostic utility of MMP-21 in malignant tumors, our findings support the notion that MMP-21 may be a molecule involved in tumor invasion and metastasis and indicated that MMP-21 was an independent prognostic factor for patients with colorectal cancer. MMP-21 might also serve as a potential target for anti-metastatic therapy via selective MMP inhibition.
References
Jianping Wang. Current and future situation of colorectal carcinoma screening .Journal of Digestive Surgery 2006; 5: 303–305
Fang SG, Yang JZ, Yang F. Clinical characteristics of 610 cases with multiple primary malignant neoplasm’s in digestive tract. Shijie Huaren Xiaohua Zazhi 1999; 7: 812
Wang MR, Guo CH, Li MS, et al. A case-control study on the dietary risk factors of upper digestive tract cancer. Zhonghua Liuxingbingxue Zazhi 1999; 20: 95–97
Yu BM, Zhao R. Molecular biology of colorectal carcinoma. Shijie Huaren Xiaohua Zazhi 1999; 7: 173–175
Chen SY, Wu TF, Liu HY, et al. Hospital-based ten-year data of gastroendoscopy. Shijie Huaren Xiaohua Zazhi 1999; 7: 15–17
Jundt F, Anagnostopoulos I, Forster R, et al. Activated Notch1 signaling promotes tumor cell proliferation and survival in Hodgkin and anaplastic large cell lymphoma. Blood 2002; 99:3398–403.
Miele L, Osborne B. Arbiter of differentiation and death: Notch signaling meets apoptosis. J Cell Physiol 1999; 181: 393–409.
Brown R S, Wahl R L. Overexpression of Glut-1 glucose transporter in human breast cancer: an immunohistochemical study. Cancer 1993: 2979–2985.
Parsons SL, Watson SA, Brown PD, et al. Matrix metalloproteinases. Br J Surg. 1997; 84:160–6.
Curran S, Murray GI. Matrix metalloprteinases: Molecular aspects of their roles in tumour invasion and metastasis. Eur J Cancer 2000; 36:1621–30.
Nagase H, Woessner JF Jr. Matrix metalloproteinases. J Biol Chem 1999; 274: 21491–4.
Nelson AR, Fingleton B, Rothenberg ML, et al. Matrix metalloproteinases: Biologic activity and clinical implications. J Clin Oncol 2000; 18:1135–49.
Park HI, Ni J, Gerkema FE, et al. Identification and characterization of human endometase (matrix metalloproteinase-26) from endometrial tumor. J Biol Chem 2000; 275: 20540–4.
Stetler-Stevenson WG. The role of matrix metalloproteinases in tumor invasion, metastasis and angiogenesis. Surg Oncol Clin N Am 2001; 10:383–92.
Hidalgo M, Eckhardt SG. Development of matrix metalloproteinase inhibitors in cancer therapy. J Natl Cancer Inst 2001; 93:178–93.
Curran S, Murray GI. Matrix metalloproteinases in tumour invasion and metastasis. J Pathol 1999; 189: 300–8.
Stetler-Stevenson WG. Type IV collagenases in tumor invasion and metastasis. Cancer Metastasis Rev Cancer Metastasis Rev 1990; 9: 289–303.
Chambers AF, Matrisian LM. Changing views of the role of matrix metalloproteinases in metastasis. J Natl Cancer Inst 1997; 89:1260–70.
Liotta LA, Stetler-Stevenson WG. Metalloproteinases and cancer invasion. Semin Cancer Biol 1990; 1: 99–106.
McDonnell S, Navre M, Coffey RJ Jr, et al. Expression and localization of the matrix metalloproteinase pump-1 (MMP-7) in human gastric and colon carcinomas. Mol Carcinog 1991; 4: 527–33.
Pyke C, Ralfkiaer E, Tryggvason K, et al. Messenger RNA for two type IV collagenases is located in stromal cells in human colon cancer. Am J Pathol 1993; 142: 359–65.
Yoshimoto M, Itoh F, Yamamoto H, et al. Expression of MMP-7 (PUMP-1) mRNA in human colorectal cancers. Int J Cancer 1993; 54: 614–8.
Zeng ZS, Guillem JG. Colocalisation of matrix metalloproteinase-9 mRNA and protein in human colorectal cancer stromal cells. Br J Cancer 1996; 74: 1161–7.
Zeng ZS, Huang Y, Cohen AM, et al. Prediction of colorectal cancer relapse and survival via tissue RNA levels of matrix metalloproteinase-9. J Clin Oncol 1996; 14: 3133–40.
Poulsom R, Pignatelli M, Stetler-Stevenson WG, et al. Stromal expression of 72 kDa type IV collagenase (MMP-2) and TIMP-2 mRNAs in colorectal neoplasia. Am J Pathol 1992; 141: 389–96.
Liabakk NB, Talbot I, Smith RA, et al. Matrix metalloprotease 2 (MMP-2) and matrix metalloprotease 9 (MMP-9) type IV collagenases in colorectal cancer. Cancer Res 1996; 56: 190–6.
Ring P, Johansson K, Höyhtyä M, et al. Expression of tissue inhibitor of metalloproteinases TIMP-2 in human colorectal cancer--a predictor of tumour stage. Br J Cancer 1997; 76: 805–11.
Oberg A, Höyhtyä M, Tavelin B, et al. Limited value of preoperative serum analyses of matrix metalloproteinases (MMP-2, MMP-9) and tissue inhibitors of matrix metalloproteinases (TIMP-1, TIMP-2) in colorectal cancer. Anticancer Res 2000; 20: 1085–91. (not differentiation survival, stage)
Sis B, Sağol O, Küpelioğlu A, et al. Prognostic significance of matrix metalloproteinase-2, cathepsin D, and tenascin-C expression in colorectal carcinoma. Pathol Res Pract 2004; 200: 379–87.
Pesta M, Topolcan O, Holubec L Jr, et al. Clinicopathological assessment and quantitative estimation of the matrix metalloproteinases MMP-2 and MMP-7 and the inhibitors TIMP-1 and TIMP-2 in colorectal carcinoma tissue samples. Anticancer Res 2007; 27: 1863–7.
Cho YB, Lee WY, Song SY, et al. Matrix metalloproteinase-9 activity is associated with poor prognosis in T3-T4 node-negative colorectal cancer. Hum Pathol 2007; 38: 1603–10.
Hilska M, Roberts PJ, Collan YU, et al. Prognostic significance of matrix metalloproteinases-1, -2, -7 and −13 and tissue inhibitors of metalloproteinases-1, -2, -3 and −4 in colorectal cancer. Int J Cancer 2007; 121: 714–23.
Ahokas K, Lohi J, Lohi H, et al.Matrix metalloproteinase-21, the human orthologue for XMMP, is expressed during fetal development and in cancer. Gene 2002; 301: 31–41.
Ahokas K, Lohi J, Illman SA, et al. Matrix metalloproteinase-21 is expressed epithelially during development and in cancer and is up-regulated by transforming growth factor-beta1 in keratinocytes. Lab Invest 2003; 83: 1887–99.
Kuivanen T, Ahokas K, Virolainen S, et al.MMP-21 is upregulated at early stages of melanoma progression but disappears with more aggressive phenotype.Virchows Arch 2005; 447: 954–60.
Boyd S, Virolainen S, Pärssinen J, et al. MMP-10 (Stromelysin-2) and MMP-21 in human and murine squamous cell cancer. Exp Dermatol. 2009; 18: 1044–52.
Rhodes A, Jasani B, Barnes DM, et al. Reliability of immunohistochemical demonstration of oestrogen recep tors in routine practice: interlaboratory variance in the sensitivity of detection and evaluation of scoring systems. J Clin Pathol 2000; 53: 125–130
Curran S, Dundas SR, Buxton J, et al. Matrix metalloproteinase/tissue inhibitors of matrix metalloproteinase phenotype identifies poor prognosis colorectal cancers. Clin Cancer Res 2004; 10: 8229–34.
Lyall MS, Dundas SR, Curran S, Murray GI. Profiling markers of prognosis in colorectal cancer. Clin Cancer Res 2006; 12: 1184–91.
Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 1990; 322: 352–8.
Peng ZR, Zhong WH, Liu J, Xiao PT. Effects of the combination of hyperbaric oxygen and 5-fluorouracil on proliferation and metastasis of human nasopharyngeal carcinoma CNE-2Z cells. Undersea Hyperb Med 2010; 37: 141–50.
Coskun U, Yamac D, Gulbahar O, et al. Locally advanced breast carcinoma treated with neoadjuvant chemotherapy: are the changes in serum levels of YKL-40, MMP-2 and MMP-9 correlated with tumor response? Neoplasma 2007; 54: 348–52.
Wang W, McLeod HL, Cassidy J. Disulfiram-mediated inhibition of NF-kappaB activity enhances cytotoxicity of 5-fluorouracil in human colorectal cancer cell lines. Int J Cancer 2003; 104: 504–11.
Tamatani T, Azuma M, Ashida Y, et al. Enhanced radiosensitization and chemosensitization in NF-kappaB-suppressed human oral cancer cells via the inhibition of gamma-irradiation- and 5-FU-induced production of IL-6 and IL-8. Int J Cancer 2004; 108: 912–21.
Chu D, Zhang Z, Li Y, et al. Matrix metalloproteinase-9 is associated with disease-free survival and overall survival in patients with gastric cancer.Int J Cancer 2010 Oct 18.
Kyllönen H, Pasanen AK, Kuittinen O, et al. Lack of prognostic value of MMP-9 expression and immunohistochemically defined germinal center phenotype in patients with diffuse large B-cell lymphoma treated with modern chemotherapy with or without CD20 antibody. Leuk Lymphoma 2009; 50: 1301–7.
Acknowledgments
This work was supported by the Science Foundation of Shaanxi Province (No. 2009 K01-81).
Author information
Authors and Affiliations
Corresponding author
Additional information
Yi Huang and Wenhai Li contributed equally to this work.
Rights and permissions
About this article
Cite this article
Huang, Y., Li, W., Chu, D. et al. Overexpression of Matrix Metalloproteinase-21 is Associated with Poor Overall Survival of Patients with Colorectal Cancer. J Gastrointest Surg 15, 1188–1194 (2011). https://doi.org/10.1007/s11605-011-1519-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-011-1519-5