
Abstract
Introduction
The pancreatoduodenal junction is a small anatomic area where pathologic processes involving the distal bile duct, duodenum, pancreatic head, ampulla de Vater, and retroperitoneum converge. Differential diagnosis includes a spectrum of entities that ranges from anatomical variants to malignancies.
Purpose
The aim of this paper was to review the anatomy and different pathologic conditions, whether tumoral, inflammatory, or congenital in origin, in this specific area that involves the pancreatic head, duodenum, duodenal ampulla, distal pancreatobiliary tract junction, and retroperitoneum.
Methods
Computed tomography (CT) and magnetic resonance (MR) help us to identify specific radiologic signs that allow to divide the pancreatic-duodenal junction abnormalities into three cathegories: (1) normal variants and congenital anomalies (pancreas divisum, santorinicele, annular pancreas,duodenal duplication cyst, choledocal cyst,...); (2) acquired non-tumoral: traumatic, iatrogenic, inflammatory (duodenal hematoma, duodenal iatrogenic perforation, groove pancreatitis, gastroduodenal artery pseudoaneurysm,...); (3) tumoral (pancreatic head adenocarcinoma, periampullary tumors, neuroendocrine pancreatic tumors, duodenal adenocarcinoma,...). The images illustrate morphologic aspects of these entities.
Results and Conclusions
CT and MR are the most appropiate imaging modalities to evaluate pancreatoduodenal junction. Knowing the imaging features is crucial to reach the right diagnosis and treatment of the different entities that involve this anatomic area.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
The pancreatoduodenal groove is a potential space bordered by the head of the pancreas, duodenum, and common bile duct. This is a very small anatomical area where pathologic processes that involve the pancreatic head, duodenum, distal pancreatobiliary tract, duodenal papilla, and retroperitoneum converge. Differential diagnosis includes a spectrum of entities that ranges from anatomical variants to malignancies.
Computed tomography (CT), magnetic resonance (MR) imaging have revolutionized the diagnostic imaging. The complex anatomic relationships of a variety of structures in this small area of the upper abdomen have given rise to diagnostic challenges in which a variety of benign and neoplastic processes often mimic primary neoplasia of the involved structures.
It is important for the radiologist and surgeons to be familiar with the wide spectrum of anatomic variants and pathologic entities that can involve this anatomic area in order to initiate the appropriate lesion-specific work-up and treatment, and avoid unnecessary tests or procedures.
The aim of this paper was to review by means of CT and MR the different pathologic conditions, whether tumoral, inflammatory, or congenital, that affect this area
Anatomic Landmarks
This anatomic area is bordered medially by the pancreatic head. The second portion of the duodenum forms the lateral border. The descending duodenal serosa surface is intimately related to the pancreatic head covering the pancreatoduodenal groove. The posterior border is formed by the third portion of the duodenum or the inferior vena cava, and the anterosuperior border by the first duodenal portion or duodenal bulb1
The pancreatic head contains distal bile duct and the main and accessory pancreatic ducts. In the medial duodenal wall, major and minor papillae are located.
Along the pancreatoduodenal groove runs the superior pancreatoduodenal artery, a branch of the gastroduodenal artery that anastomoses with the inferior pancreatoduodenal artery, a branch of superior mesenteric artery, establishing an anatomic and radiologic landmark between pancreatic head and duodenum (Fig. 1). There are small lymph nodes in the groove generally not depicted on imaging.

Vascularization of the pancreatoduodenal area. a On the left schematic drawing, shown is the gastroduodenal artery (green arrow) which supplies blood directly to the pylorus (distal part of the stomach) and proximal part of the duodenum, and indirectly to the pancreas via the superior pancreaticoduodenal artery (purple arrows) that establishes an anatomic landmark between pancreatic head and second portion of the duodenum. The inferior pancreaticoduodenal artery (yellow arrow) arises from the superior mesenteric artery (AMS) and establishes an anatomic landmark between pancreatic uncinate process and third portion of the duodenum. b On the right axial CT image, seen is the level of the second portion of the duodenum showing the superior pancreaticoduodenal artery (red arrow) as a landmark between pancreatic head and duodenum. c, d Coronal MPR and gross specimen (courtesy FJ. Sancho, MD) located in pancreatoduodenal area showing the relationship between the pancreatic head and the second duodenal portion
CT and MR help us to identify specific radiologic signs that allow to divide the pancreatoduodenal junction abnormalities into three categories:
-
1.
Normal variants and congenital anomalies (páncreas divisum, santorinicele, annular pancreas, duodenal duplication cyst, choledochal cyst,...)
-
2.
Acquired non-tumoral: traumatic, iatrogenic, inflammatory (duodenal hematoma, duodenal iatrogenic perforation, groove pancreatitis, pancreatoduodenal artery pseudoaneurysm,...)
-
3.
Tumoral (pancreatic head adenocarcinoma, periampullary tumors, neuroendocrine pancreatic tumors, duodenal adenocarcinoma,...)
-
1.
Normal variants and congenital anomalies.
-
Pancreas divisum: is the most frequent variant of pancreatic ductal configuration and occurs in 2–7% of general population. In this condition, at the seventh/eighth week of gestation, dorsal and ventral pancreatic ducts fail to fuse. Dorsal duct drains directly in the minor papilla while ventral duct drains in the major papilla. The majority of patients are asymptomatic but a subset of patients has either unexplained abdominal pain or episodes of acute pancreatitis. A relative obstruction to the flow of pancreatic fluid at the level of an inadequately patent or stenosed minor papilla has been hypothesized to result in an increase in intraductal pressure with consequent pancreatitis. On imaging, CT or MR cholangiopancreatography (MRCP) demonstrate separate pancreatic ducts draining to the region of the minor and major ampulla2 (Fig. 2a, b).
Fig. 2 
Pancreas divisum. a 2D MRCP showing a complete pancreas divisum. Dorsal duct drains independently into the minor papilla (mP) whereas the ventral duct drains jointly with the common bile duct (CBD) into the major papilla (MP). b Axial T2 WI depicts the anterior crossing in the axial plane of the dorsal duct and its independent draining into the minor papilla
-
Duodenal duplication: duplication cyst can be localized in any part of gastrointestinal tract, and the duodenum is not an uncommon site. Although most of them are not communicated with the lumen, it can occur. The typical symptoms, if present, are related with obstruction or complication as distension, infection, volvulus, or intussusception. At ultrasonography, there is an anechoic or hypoechoic structure, uni- or multilocular. On CT scan, it is seen as an area of low density with an enhancing wall3 (Fig. 3a–d).
Fig. 3 
Duodenal duplication cyst. a Axial T2 WI showing duodenal duplication cyst (DC) bordered by the second and third duodenal portions (yellow arrows) and medially by pancreatic head (P). Thick-walled, well-defined cystic lesions in pancreatoduodenal groove not communicated with duodenal lumen. b Axial contrast-enhanced CT at the same level in (a). The gastroduodenal artery (red arrow) is displaced medially indicating non-pancreatic origin of the lesion. c MIP 3D MRCP reformation depicts the laterally displaced second and third duodenal portions (yellow arrow). d MIP 3D arterial CT showing the medial displacement of the gastroduodenal artery. It represents an indirect sign of non-pancreatic or duodenal origin of the lesion
-
Santorinicele: in a pancreas divisum setting, santorinicele represents a cystic dilatation of the distal dorsal duct, just proximal to the minor papilla (analogous to ureteroceles or choledochoceles). It is the result of relative obstruction and weakness of the distal ductal wall. It is a suggested cause of relative stenosis of the minor papilla resulting in high intraductal pressure, responsible for recurrent episodes of acute pancreatitis
Dynamic MRCP of the pancreatic duct can be performed after secretin stimulation. This technique improves depiction of pancreatic ducts and may be effective in diagnosing the presence of santorinicele in patients who have pancreas divisum and unexplained recurrent episodes of acute pancreatitis and who might benefit from endoscopic treatment (Fig. 4).4
Fig. 4 
Pancreas divisum and associated santorinicele. Secretin-stimulated MR-pancreatography helps to depict small cystic dilatation (arrow) of the terminal intramural portion of the main pancreatic dorsal duct in a pancreas divisum setting; it is the same case in Fig. 2
-
Annular pancreas: is the second most common congenital pancreatic anomaly and results in pancreatic tissue encircling, partially or completely, the second portion of the duodenum (Fig. 5). MR cholangiopancreatography delineates the pancreatic duct encircling the duodenum (Fig. 6).
Fig. 5 
Annular pancreas. CT image showing pancreatic tissue (green arrows) encircling the second portion of the duodenum (D)
Fig. 6 
Annular pancreas. MRCP of an annular pancreas where the ventral duct encircles the second portion of the duodenum for almost 360°. There is a mild dilatation of the ventral duct revealing its obstructive component and the cause of repeated episodes of acute pancreatitis. Choledochal cyst type Ic is present additionally
The presentation in adults differs from that in children. Congenital anomalies and duodenal obstruction are the predominant features in children, and pancreatitis is the main presentation in adults.
The radiologist is often the first to make the diagnosis of this entity.5
-
Choledochocele: is a rare abnormality consisting of cystic or diverticular dilatation of the terminal intramural portion of the common bile duct (Fig. 7). It is classified as choledochal cyst type III in Todani’s classification and represents 1.4–5% of choledochal cysts. Choledochocele can be further subdivided into three subtypes: type IIIa represents the choledochocele in the intraluminal duodenum and contains the terminal pancreatic and common bile duct as a common channel; type IIIb contains separate ductal structures with an intraluminal cyst, and type IIIc shows a cyst completely contained within the intramural portion of the duodenum.6
Fig. 7 
Choledochocele. a MRCP showing the cystic dilatation of the terminal intramural portion of the common bile duct. b scheme showing intraluminal choledochocele with separate openings for CBD and pancreatic duct (IIIb)37
Some authors have proposed that choledochoceles are congenital in origin while others suggest abnormal biliary motility could be a contributing factor in the pathogenesis of choledochoceles.
Complications of biliary duct cysts include recurrent pancreatitis, pancreatic necrosis, cholangitis, primary cyst stones, and cholangiocarcinoma (2.5%).7
-
-
2.
Acquired non-tumoral: can be further divided into traumatic, iatrogenic, and inflammatory.
-
Duodenal diverticulum: it is the most common acquired alteration of the duodenum. It more commonly arises in the periampullary region along the medial aspect of the second and third portions of the duodenum. Usually asymptomatic, it can become impacted with debris leading to duodenal diverticulitis and even perforation (Fig. 8) or hemorrhage.1
Fig. 8 
Duodenal diverticulum rupture. Unenhanced CT scan showing a ruptured diverticulum of the third portion of the duodenum. Oral contrast is out of the duodenal lumen outlining the outer wall of the duodenum, spreading into the retroperitoneum
When filled with fluid, it may mimic a cystic neoplasm, abscess, or pseudocyst. The finding of small amounts of gas or oral contrast in the diverticulum clarifies the diagnosis. Intradiverticular drainage of the main bile duct can occur (Fig. 9) and may cause biliary dilatation or preclude a successful endoscopic therapy.8
Fig. 9 
Intradiverticular papilla. a MRCP showing intradiverticular drainage of the main bile duct (arrow) in b duodenal diverticulapresent a major source of failure for endoscopic retrograde cholangiopancreatography (ERCP) if the common bile duct drains directly into a periampullary diverticulum, obscuring the orifice of the ampulla of Vater. In rare cases, a duodenal diverticulum may become obstructed, resulting in associated duodenal diverticulitis
-
Duodenal hematoma: is a rare abdominal injury most commonly seen in children after blunt abdominal trauma, sometimes minor (handlebar trauma, road traffic injury, and sports trauma). Bleeding disorders, Henoch–Schönlein purpura, anticoagulation therapy, alcoholism, pancreatitis, tumors, duodenal ulcers, and local or iatrogenic factors account for the remaining 30% of the cases.9
Duodenal hematoma is a well-recognized manifestation of child abuse.10
The duodenum is crushed against the vertebral body causing contusion or transection that can generate intramural bleeding and hematoma. This hematoma can increase and gradually obstruct the lumen (Fig. 10). Anatomic factors, such as duodenal retroperitoneal fixation, the rich submucosal and subserosal vascular plexus, and a weak muscular abdominal wall, are all contributory to the development of duodenal intramural hematomas.11
Fig. 10 
Duodenal hematoma. a Large duodenal hematoma. After an endoscopic procedure to sclerose a duodenal peptic ulcer, a hyperdense intramural mass is seen. On unenhanced CT, it occupies the second portion of the duodenum. b After intravenous contrast administration, a small point of active bleeding can be seen (arrow) (courtesy J Palmer, MD)
-
Pancreatoduodenal artery pseudoaneurysm: is an uncommon but important complication associated with chronic pancreatitis. Pseudoaneurysm develops because of the action of pancreatic enzymes over the arterial walls. Lesions originate from the erosion of an artery inside a pancreatic pseudocyst by enzymes, mainly elastases, released from the pancreas.
The most common affected artery by pseudoaneurysm is the splenic artery. Next in frequency are gastroduodenal and pancreatodudenal arteries, followed by left gastric artery, although any local artery can be involved (Fig. 11).12–14
Fig. 11 
Gastroduodenal artery pseudoaneurysm rupture. a, b An enhancing pancreaticoduodenal pseudoaneurysm with mural calcifications in an axial enhanced CT and 3D reconstruction. c, d. Enhanced CT scan showing a point of active bleeding (yellow arrow) from gastroduodenal artery. IV Contrast pools in the left retroperitoneum (white arrow)
The pancreatoduodenal artery runs along the pancreatoduodenal groove, establishing an anatomic and radiologic landmark between pancreatic head and duodenum. On CT imaging, it is seen as an enhanced rounded mass that arises at the pancreatoduodenal groove, rarely exceeding 5 cm in diameter, and usually presenting thin wall calcifications and mural thrombosis. Pseudoaneurysms are often fully asymptomatic, unless they rupture and bleed. About 50% of pseudoaneurysms eventually rupture with major hemorrhage into the retroperitoneum, peritoneal cavity, or intestinal lumen.15
-
Acute pancreatitis: inflammation and fluid collections can be located in duodenopancreatic junction, in the course of acute pancreatitis Serial studies showing changes in fluid collections can help to differentiate acute pancreatitis from groove pancreatitis.1
-
Groove pancreatitis: is an uncommon type of focal chronic pancreatitis affecting the groove between the head of the pancreas, the duodenum, and the common bile duct (Fig. 12). Patients affected by GP are relatively young men with a history of alcohol abuse in the majority of cases.16 The clinical setting is similar to other chronic pancreatitis, but recurrent vomiting due to progressive duodenal stenosis represents its main clinical feature.17
Fig. 12 
Groove pancreatitis. a Unenhanced CT scan showing mass-like occupation of the pancreaticoduodenal groove.Punctate calcification can be seen. b T1WI at the same level clearly depicts the hypointense band (arrow) between pancreatic head and the second portion of the duodenum. c Arterial phase dynamic Gd-MR shows hypovasculatiry of the T1WI hypointense area. d Delayed phase dynamic Gd-MR depicts delayed enhancement of the pancreatitic fibrotic area, characteristic of fibrous tissue
The pathogenesis of groove pancreatitis remains controversial. Several factors may be related, including previous diseases of the biliary system, peptic ulcers, gastric resections, duodenal wall or pancreatic head cysts, and pancreatic head heterotopia in the duodenum (Fig. 13). Chronic inflammation of the duodenum with scar tissue in the wall leads to fibrosis and stenosis. Cystic changes are frequently encountered according to most accepted theories; they represent cystic dystrophy of a heterotopic pancreas tissue in the duodenal wall.18
Fig. 13 
Groove pancreatitis. On the left, two axial enhanced CT scans showing fat stranding around pancreaticoduodenal area, mass-like occupation of the pancreaticoduodenal groove, duodenal wall thickening, and the presence of small cysts. According to the most accepted theories, they represent cystic dystrophy of a heterotopic pancreas in the duodenal wall. On the right, enhanced CT coronal reformation depicts the cystic and hypodense band between the pancreas (P) and the second portion of the duodenum (D)
Two forms of the disease can be recognized, the pure and the segmental one.19 The pure form affects the groove only, while the pancreatic parenchyma is preserved. The segmental form predominantly involves the head of the pancreas in proximity to duodenal wall.20
On CT, a hypodense mass-like lesion can be identified between the pancreatic head and the duodenum. The peripancreatic vessels used to be preserved, even in extensive disease. In the segmental form, the main pancreatic duct may be mildly dilated in the pancreatic body and tail, while, in the pure form of the disease, it usually appears normal.17
On MR, the mass is hypointense to pancreatic parenchyma on T1-weighted images and can be hypo-, iso-, or slightly hyperintense on T2-weighted images. Delayed images show heterogeneous enhancement due to the fibrous tissue.17 Main differential diagnosis of groove pancreatitis is the groove pancreatic adenocarcinoma of the pancreas which is often very difficult to differentiate due to the lack of specific discriminating imaging features. It is crucial to arrive at a right diagnosis since groove pancreatitis is usually managed with conservative medical treatment while pancreatic adenocarcinoma is treated with surgery in a radical curative attempt.
As mentioned above, in groove pancreatitis, peripancreatic vessels used to be preserved while pancreatic carcinoma is expected to invade along large peripancreatic vessels.16
As reported by Yu et al. on MR cholangiopancreatography, the stenosed intrapancreatic portion of the bile duct in patients with segmental form of groove pancreatitis used to be longer and smoother, in contrast to the abrupt and irregular ductal stenosis seen in patients with pancreatic carcinoma.1
To consider groove pancreatitis in the differential diagnosis of pancreatic carcinoma is fundamental for an appropriate management. Differentiating both entities is difficult based only on radiologic features.21 MRCP can be helped by endoscopic retrograde cholangiopancreatography (ERCP). Both may show the smooth and regular stenosis of the common bile duct, characteristic of groove pancreatitis or the irregular ductal stenosis typically seen in pancreatic carcinoma.22 Unfortunately, despite the advances in technology and the exhaustive use of imaging techniques, surgical resection is required to reach the diagnosis.
Although discussing the surgical technique is beyond the aim of this article, the Whipple technique is the most frequently performed. The information provided by CT scans about vascular and invasion of surrounding structures, and by endoscopic ultrasonography and ERCP in case of extrahepatic biliary obstruction,23 is crucial in order to plan a pancreatoduodenectomy.
-
-
3.
Acquired tumoral:
-
Groove pancreatic adenocarcinoma: pancreatic ductal head adenocarcinoma arises from the epithelium of the main pancreatic duct or a side branch and sometimes can present as a pancreatic exophitic mass arising in groove area; the main pancreatic duct can be spared from invasion. In these cases, it cannot be reliably differentiated from groove pancreatitis by means of CT and MR.17 The findings of cystic lesions within the mass, lack of gastroduodenal artery invasion, and thickened duodenal wall with scarring and stenosis of duodenal lumen are more common in groove pancreatitis. On the contrary, vascular encasement suggests malignancy (Fig. 14). Main pancreatic duct dilatation can occur in both cases. Biopsy of duodenal mucosa invaded is the clue to reach the diagnosis. Groove pancreatitis should be considered in the differential diagnosis of pancreatic head tumor.24
Fig. 14 
Groove pancreatic adenocarcinoma. a–c Descending contiguous enhanced CT scans showing a pancreatic adenocarcinoma arising in the pancreaticoduodenal groove as a solid infiltrating mass that encases gastroduodenal artery. No cystic lesions are seen within the mass. Although endoscopic biopsy of the duodenum ulcers are required, the findings on CT make pancreatic adenocarcinoma the more likely diagnosis
-
Duodenal adenocarcinomas: is the most common primary malignant neoplasm, with the 50–70% of small bowel adenocarcinomas arising from duodenum or proximal jejunum. It is most prevalent at seventh decade. Jaundice, bleeding, or obstruction can be the clinical signs. At CT, the diagnosis arises from a polypoid or intramural mass site, typically in the second or third portions of duodenum (Fig. 15). MR can show a soft-tissue mass or thickening of duodenal wall too. It is usually diagnosed in the advanced stage with more than 50% of patients having nodal metastasis at the time of diagnosis, although the 5-year survival rate approaches 50%. Secondary involvement of the duodenum can occur by local involvement, as in pancreatic tumor, or metastases from distant sites as colon or ovarian carcinoma.25,26
Fig. 15 
Duodenal adenocarcinoma. CT scan shows a solid intraluminal soft-tissue mass in the medial wall of the second duodenal portion with transmural invasion into the pancreatic head
-
Duodenal gastrointestinal estromal tumor (GIST): GISTs are the most common mesenchymal neoplasm of the gastrointestinal tract. The best defining feature of GIST is the expression of KIT (CD117), a tyrosin kinase growth receptor. The most common clinical sign or manifestation is bleeding from ulceration mucosa or small intestine obstruction when located in gastrointestinal tract (radiographics). It represents 10–33% of overall malignant duodenal tumors, most of them located in the second or third portion of the duodenum and often with extraserosal component causing a significant mass effect over adjacent organs. On CT images, they can appear as intramural mass or endoluminal polyps (Fig. 16) or as a large well-circumscribed tumor, usually with extraluminal growing and heterogeneous enhancement with peripheral rim and low-atenuation necrotic center. Whereas lymph node enlargement is not a predominant feature, liver and peritoneum are the most common sites for distant metastasis.27,28
Fig. 16 
Duodenal gastrointestinal stromal tumor. a Unenhanced CT scan shows a large tumoral mass, predominantly extraluminal, arising in the medial wall of the second portion of the duodenum. b Contrast-enhanced CT scan shows well-defined mass with peripheral high attenuating rim and central areas of low attenuation
-
Neuroendocrine tumor: Gastrinoma is the most common neuroendocrine tumor located in the groove and is often extrapancreatic or multiple. Most of them are located in the so-called “gastrinoma triangle”, whose vertices are the cystic duct confluence, the junction of the pancreatic neck and body, and the junction of the second and third portion of the duodenum1 (Fig. 17).
Fig. 17 
Gastrinoma triangle. Schematic drawing of the gastrinoma triangle whose vertices are the cystic duct confluence, the junction of the pancreatic neck and body, and the junction of the second and third portions of the duodenum. Gastrinoma is the most common neuroendocrine tumor at the pancreatoduodenal groove
Symptoms of peptic ulcer disease and diarrhea, and elevated serum levels of gastrin are present in those patients, although hypergastrinemia alone is not diagnostic.29
A triple-phased contrast enhancement is recommended in CT studies.30 Its intense enhancement on CT (Fig. 18) and MR, the high signal intensity in T2-weighted sequences, and the presence of hypervascular liver metastases help to differentiate them from pancreatic adenocarcinoma.1
Fig. 18 
Gastrinoma in pancreaticoduodenal groove. Enhanced CT scan showing small well-defined hypervascular tumor inside the gastrinoma triangle area (pancreaticoduodenal groove). The patient had Zollinger–Ellison Syndrome, and the resected tumor corresponded to a gastrinoma
-
Intraductal papillary mucinous tumor (IPMT): It refers to a spectrum of mucin-secreting proliferation of the pancreatic duct epithelium at any level of the pancreatic ductal system. IPMT has intraductal growth pattern, and the progressive duct dilatation is associated with mucin secretion.31
Although the tumor is usually small and flat, the entire main pancreatic duct is dilated because the mucin secretions impede the correct flow of pancreatic secretion. It is considered a low-grade malignancy, but prognosis for the different types are still not well-known. It can produce pain and laboratory abnormalities consistent with pancreatitis. It can be localized in the main pancreatic ducts or in branch ducts, the latest especially, in the branch ducts of the uncinate process, but it may be also diffuse, affecting a large number of pancreatic ducts. When it affects the uncinate process branches, it can protrude into the papilla and duodenal lumen (Fig. 19).
Fig. 19 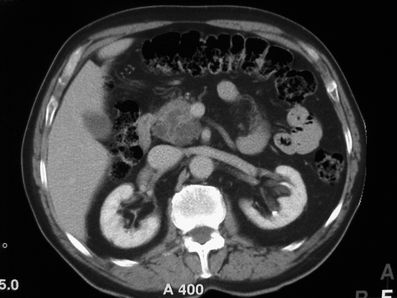
Intraductal papillary mucinous tumor of the uncinate process. Enhanced CT scan shows a cystic lesion with solid component at the uncinate process
Total resection is the treatment of choice for the main duct type, and local resection is enough if only segmental involvement is present. Cystic lesions less than 2.5 cm and with no communication with the main duct can be followed up. Ductal nodules, intraductal mucin, and herniation of the papilla into the duodenal lumen can help to differentiate from chronic pancreatitis.32
-
Periampullary tumors are the third most frequent gastrointestinal tumors following gastric and colorectal tumors. They arise 2 cm from the ampulla and comprise carcinoma of the ampulla, distal common bile duct, pancreas, and duodenum. They share similar clinical presentation, anatomic location, and therapeutic approaches, but the long-term outcome depends on the specific type. Presurgical staging depends on infiltration of surrounding tissue, and differentiation among them is important for treatment planning. Both CT and MR can be used to evaluate local invasion to choose the most accurate treatment.
Ampullary carcinoma and distal bile duct carcinoma can be seen as a small mass, bulging or not, into the papilla, or periductal thickening (Fig. 20) while a pancreatic hypoattenuating mass is typical of pancreatic carcinoma. Dilatation of two proximal and two distal pancreatic or biliary ducts or the side pancreatic branches orientate to pancreas origin whereas proximal biliary duct dilatation with normal distal bile duct and no dilated pancreatic duct is seen in distal bile carcinoma. Duodenal carcinomas present only a minimum or absent bile or pancreatic duct dilatation.25
Fig. 20 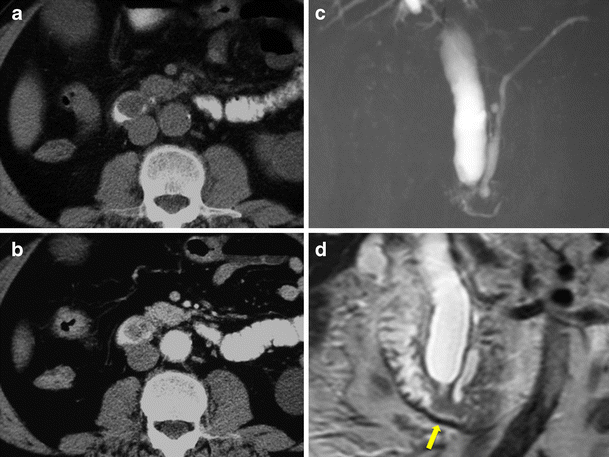
Ampullary tumor. a–b Unenhanced and enhanced CT image shows an intraluminal well-defined tumor dependent from the medial duodenal wall at the level of the papilla corresponding to an ampullary tumor. c, d MR cholangiopancretography SSH SE image and coronal T2 fast SE sequence shows an important billiary tree dilatation untill the major papilla. Note the lack of dilatation of the main pancreatic duct (yellow arrow), the called “single duct sign” common in ampullary tumors
The prognosis of ampullary carcinoma and duodenal periampullary carcinoma is better than bile distal ducts and pancreatic carcinoma. The small size at diagnosis and the early symptoms due to the localization and the intraluminal growth are some of the reasons of the better prognosis of ampullary carcinoma, and the rare extraluminal extension and perineural or lymphatic spread contributes too.33,34
-
Lymph nodes: small lymph nodes in the groove is an usual finding in both hepatopancreatic CT and MR. Spread from distant malignancies to duodenopancreatic lymph nodes is common and difficult to differentiate from primary local tumors. Liver, biliary tract, pancreas, and duodenum disease may cause lymph node enlargement (Fig. 21a). Lymphoma and local inflammation can involve groove lymph nodes.26
Fig. 21 
Necrotic lymph nodes. a Shows a hypodense necrotic lymph node in the pancreaticoduodenal groove corresponding to a metastasic gallbladder squamous tumor. Note the anterior displacement of the duodenum (arrow). b Shows another necrotic hypodense lymph node corresponding to disseminated tuberculosis
Lymphadenopathy below the level of renal veins favors the diagnosis of lymphoma in front of local neoplasm. Inflammatory diseases include rare entities as a sarcoidosis or Castleman disease. Concomitant liver or spleen lesions are seen in the first, while the second one presents with intense enhancement adenopathy.35
Due to the increase prevalence both inmunocompetent and inmunocompromised patients, tuberculosis is a disease to consider. As lymphadenopathy is the most common manifestation of abdominal tuberculosis, large and multiple central low-density nodes, often accompanying large nodes in other abdominal locations, makes tuberculosis the most likely diagnosis in this case. The hypoattenuating center with hyperattenuating rim are characteristics of caseous necrosis36 (Fig. 21b).
-




















Conclusion
CT and MR are the most appropiate imaging modalities to evaluate pancreatoduodenal junction. The knowledge of normal anatomy, most frequent variants, and the imaging features of the different entities that involve this small anatomic area is crucial to reach the right diagnosis and treatment.
References
Yu J, Fulcher AS, Turner MA, et al. Normal anatomy and disease processes of the pancreatoduadenal groove: imaging features.AJR 2004;183:839–846.
Steinberg, William M.; Chari, Suresh T.; Forsmark, Chris E.; Sherman, Stuart; Reber, Howard A.; Bradley, Edward L. III; DiMagno, Eugene. Controversies in Clinical Pancreatology: Management of Acute Idiopathic Recurrent Pancreatitis. Pancreas: August 2003 - Volume 27 - Issue 2 - pp 103–117
Liechtenstein et al. Imaging interpretation session: 1995. Radiographics 1996;16:215–239.
Manfredi R, Costamagna G, Brizi MG, Spina S, Maresca G, Vecchioli A, Mutignani M, Marano P. Pancreas divisum and “santorinicele”: diagnosis with dynamic MR cholangiopancreatography with secretin stimulation..Radiology November 2000 217:403–408
Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA. Annular pancreas in adults. AJR 2009; 193:455–460.
Greene FL, Brown JJ, Rubinstein P et al. Choledochocele and recurrent pancreatitis. Diagnosis and surgical management. Am J Surg 1985; 149(2):306–9.
Todani T, Watanabe Y, Narusue M et al. Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg 1977; 134(2):263–9
Rajnakova A, Goh PM, Ngoi SS, Lim SG. ERCP in patients with periampullary diverticulum. Hepatogastroenterology. 2003 May–Jun;50(51):625–8.)
Megremis S, Segkos N, Andrianaki A, Gavridakis G, Psillakis K, Triantafyllou L, Katsougris N, Michalakis M, Sfakianaki E. Sonographic diagnosis and monitoring of an obstructing duodenal hematoma after blunt trauma: correlation with computed tomographic and surgical findings. J Ultrasound Med 23:1679–1683 • 0278–4297.
Hahn PF, Stark DD, Vici LG, Ferrucci JT Jr. Duodenal hematoma: the ring sign in MR imaging..Radiology May 1986 159:379–382.
Miguel Iuchtman MD PhD, Tzvi Steiner MD, Tzvi Faierman MD, Alla Breitgand MD and Gabriel Bartal MD. Post-Traumatic Intramural Duodenal Hematoma in Children Isr Med Assoc J. 2006 Feb;8(2):95–7.
B.E. Stabile, S.E. Wilson and H.T. Debas, Reduced mortality from bleeding pseudocysts and pseudoaneurysms caused by pancreatitis. Arch Surg 118 (1983), pp. 45–51.
M. De Perrot, T. Berney, L. Bühler, X. Delgadillo, G. Mentha and P. Morel, Management of bleeding pseudoaneurysms in patients with pancreatitis. Br J Surg 86 (1999), pp. 29–32.
J.S. Bender and M.A. Levison, Pseudoaneurysm of the gastroduodenal artery arising within a pancreatic pseudocyst. Ann Vasc Surg 6 (1992), pp. 171–172
L. Benoit, J. Fraisse, J.P. Cercueil, A. Cornet and J. Cuisenier, Anévrysme de l’artère gastroduodénale et pancréatite chronique. Ann Chir 50 (1996), pp. 918–920
Triantopoulou C, Dervenis C, Giannakou N, Papailiou J, Prassopoulos P. Groove pancreatitis: a diagnostic challenge. Eur Radiol (2009) 19: 1736–1743
Blasbalg R, Baroni RH, Costa DN, Machado MC MRI features of groove pancreatitis..AJR 2007; 189:73–80.
Chatelain D, Vibert E, Yzet T, et al. Groove pancreatitis and pancreatic heterotopia in the minor duodenal papilla. Pancreas 2005; 30:e92–e95
Stolte M, Weiss W, Volkholz H, Rosch W. A special form of segmental pancreatitis: “groove pancreatitis.” Hepatogastroenterology 1982; 29:198–208
Adsay NV, Zamboni G. Paraduodenal pancreatitis: a clinico-pathologically distinct entity unifying “cystic dystrophy of heterotopic pancreas”, “para-duodenal wall cyst” and “groove pancreatitis”. Sem Diagn Pathol 21:247–254.
Tan CH, Chow PK, Thng CH, Chung AY, Wong WK. Pancreatic adenocarcinoma that mimics groove pancreatitis: case report of a diagnostic dilemma. Dig Dis Sci 51(7):1294–6, 2006.
Balakrishnan V, Chatni S, Radhakrishnan L, Narayanan VA, Nair P. Groove pancreatitis: a case report and review of literature. JOP 8(5):592–7, 2007.
Ahmad SA, Lowy AM, McIntyre BC, Mathew JB. Pancreaticoduodenectomy Journal of Gastrointestinal Surgery 9 (1):138–143, 2005.
Tan CH, Chow PKH, et al. Pancreatic adenocarcinoma that mimics groove pancreatitis: case report of a diagnostic dilemma. Digestive disease and sciences 2006; 51:1294–1296.
Kim J.H., Kim M.J., Chung J.J., et al. Differential diagnosis of periampullary carcinomas at MR imaging. Radiographics 2002; 1335–1352.
Jayaraman M, Mayo-Smith W, Movson JS, et al. CT of the duodenum: an overlooked segment gets its due. Radiographics 2001; 21:S147–S160.
Levy A.D., Remotti H.E., Thompson W.M., et al. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics 2003; 23:283–304.
Burkill G.J.C., BadranM., Al-Muddlres O., et al. Malignant gastrointestinal stromal tumor: distribution imaging features and pattern of metastasic spread. Radiology 2003; 226:527–532.
Buetow P.C., Miller D.L., Parrino T.V., et al.Islet-cell tumors of the pancreas: clinical, radiologic and pathologic correlation in diagnosis and localization. Radiographics 1997;17:453–472.
Bronstein YL, Loyer EM, Kaur H, et al. Detection of small tumors with multiphasic helical CT. AJR 2004;182:619–623.
Procacci C, Megibow AJ, Carbognin G, et al. Intraductalpapillary mucinous tumor of pancreas: a pictorial essay. Radiographics 1999; 19;1447–1463.
Lim HJ, Lee G, Oh YL. Radiologic spectrum of intraductal papillary mucinous tumor of the pancreas.Radiographics 2001; 21:323–340.).
Periampullary cancers: are there differences? Surg Clin North Am 2001;81:543–555.
Periampullary tumors: high-spatial resolution MR imaging and histopathologic findings in ampullary region specimens. Radiology 2004;231;767–774.
Pancreatic and peripancreatic diseases mimicking primary pancreatic neoplasia. To’o KJ, Raman SS.,Yu NC, et al. Radiographics 2005;25:949–965.
Tuberculosis: a radiologic review. Burrill j, Williams C, et al. Radiographics 2007;27:1255–1273.
SM Harun et al. What cyst is this?. Biomed Imaging Interv J 2007; 3(4):e44
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hernandez-Jover, D., Pernas, J.C., Gonzalez-Ceballos, S. et al. Pancreatoduodenal Junction: Review of Anatomy and Pathologic Conditions. J Gastrointest Surg 15, 1269–1281 (2011). https://doi.org/10.1007/s11605-011-1443-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-011-1443-8