
Abstract
Introduction
The majority of pancreatic resections for malignancy are performed in older patients with major comorbidities. The aim of this study was to develop a preoperative nomogram based on the presence of comorbidities to predict risk of perioperative mortality.
Materials and Methods
The National Inpatient Sample database was queried to identify patients that underwent pancreatectomy for malignancy. The preoperative comorbidities identified as predictors were used, and a nomogram was created. Sample A (2000–2004) was utilized to develop the model, and sample B (2005) was utilized to validate this model.
Results
The overall actual observed perioperative mortality rate for samples A and B was 6.3% and 5.2%, respectively. The mean total points calculated for sample A by the nomogram was 131.7 that translates to a nomogram-predicted mortality rate of 4.9%, which is similar to the actual mortality. The mean total points for sample B was 128.1, which translates to a nomogram-predicted mortality rate of 4.6%. The similarity of mortality rates as predicted by the nomogram and a concordance index of 0.76 shows good agreement between the data and the nomogram.
Conclusion
This preoperative nomogram has been shown to accurately predict the risk of perioperative mortality following pancreatectomy for malignancy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pancreatic cancer is the fourth leading cause of cancer-related death in the USA.1 In the year 2008, 37,680 new cases of pancreatic cancer were diagnosed that accounted for 34,290 deaths.2 Surgical resection is the only modality that may offer hope for prolonging survival with reported 5-year survival rates ranging from 18% to 41% in selected patients.3,4 The advancement of surgical techniques has led to a significant decrease in perioperative mortality over the decades.3–6
Pancreatic cancer is a disease that predominantly afflicts the elderly who are more likely to be infirm and suffer from multiple pre-existing comorbidities. The pros and cons of subjecting these patients to such major operations need to be carefully weighed. The preoperative counseling of these potentially operable and high-risk patients is critical to obtaining an adequately informed and shared consent. The majority of surgeons rely on the published literature to educate the individual patient on the likely rates of perioperative mortality associated with the proposed procedures. Although we have seen a decrease in the perioperative mortality overall, there is a difference in the reported perioperative morality rates published in the literature.3–6 The single-institution studies have reported a low perioperative mortality rate of 1–2%, which may not be possible to replicate at other institutions.3–5 In contrast, population-based studies have reported a higher perioperative mortality rate ranging from 7.8% to 4.6%.6 Although the population-based data are a more accurate estimate of the national perioperative mortality rates, it may be too generalized to be applicable to that particular patient.
There is currently no specific method available to estimate the risk of perioperative mortality for the individual patient scheduled to undergo pancreatectomy for malignancy. Nomograms are graphical devices or models that use algorithms or mathematical formulae to estimate the probability of an outcome and are optimized for predictive accuracy for each individual patient. The aims of this study were to (1) develop a nomogram consisting of easily available variables that can be utilized in the preoperative setting to counsel individual patients about the perioperative mortality associated with pancreatectomy for malignancy and (2) to validate the proposed nomogram.
Materials and Methods
Data Source
The Nationwide Inpatient Sample (NIS) database was used to look at inpatient mortality following pancreatectomy for pancreatic neoplasms. The data were obtained from the Nationwide Inpatient Sample, a database developed as part of the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality. The NIS is designed to approximate a 20% sample of US hospitals. In 2005, the NIS data contained discharge data from 1,054 hospitals located in 37 states (HCUP, Nationwide Inpatient Sample, Rockville, MD: Agency for Health Care Research and Quality; 2005). Additional information about “NIS Overview” can be found at http://www.hcup-us.ahrq.gov/nisoverview.jsp.
The data for this study were compiled from the 2000–2005 versions of the NIS. All patients discharged with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes for pancreatectomy (5251—proximal pancreatectomy, 5252—distal pancreatectomy, 5253—radical subtotal pancreatectomy, 5259—other partial pancreatectomy, 526—total pancreatectomy, and 527—radical pancreatectomy) and diagnosis codes for malignant neoplasms of the pancreas (157.0—head of pancreas, 157.1—body of pancreas, 157.2—tail of pancreas, 157.3—pancreatic duct, 157.8—other specified pancreas sites, and 157.9—pancreas, part unspecified) were included. Data on patient age and sex, admission type, hospital size and type, and pancreatectomy type were extracted from the database. Perioperative mortality in the NIS database is defined as any mortality following pancreatectomy during that same hospital admission. Preoperative comorbid conditions were identified using the taxonomy published by Elixhauser et al.7 A sample definition of some of the comorbidities is shown in Table 1. A detailed description of all the comorbidities used can be found in the taxonomy published by Elixhauser et al.7 The years 2000–2004 (sample A) were used to create a predictive model, and year 2005 (sample B) was used for validation of the model. The analysis was limited to adults (age ≥18 years).
Statistical Methods
SAS software (SAS Institute Inc., Cary, NC, USA) and SUDAAN®8 software were used for all statistical analysis to account for the complex sampling design of NIS. Weighted sample estimates, standard errors, and 95% confidence limits were calculated using the Taylor expansion method. All statistical tests were two-sided, and p values less than 0.05 were considered to be statistically significant.
Chi-square tests were used to compare perioperative mortality rates by patient and hospital characteristics. We developed a nomogram to estimate the probability of perioperative mortality following pancreatectomy for pancreatic neoplasm. We first identified potential predictors of perioperative mortality with a combination of clinical experience, significance from the univariate chi-square tests, and availability at the time of admission. Multivariate logistic regression was used to find a predictive model of perioperative mortality. A nomogram was built using the techniques described by Iasonos et al.9 and Brittain et al.10 using NIS data from 2000 to 2004 (sample A). This nomogram was validated using calibration plots and with a concordance index using data from NIS 2005 (sample B). Briefly, the concordance index is calculated by comparing the patients that had died to those that are alive in sample B. All possible pairs are constructed between those who died and those alive. For each pair, if the nomogram assigns a higher probability of death to the patient who died than the one alive, then the model matches the data, and the pair is said to be concordant. The concordance index is the probability of being concordant out of all possible dead/alive patient pairs. A 95% confidence interval is presented for the concordance index based on 10,000 bootstrapped samples. A calibration plot is constructed by plotting predicted probabilities from the nomogram versus the actual probabilities. For sample A, deciles (quartiles for sample B due to smaller sample size) of the predicted probabilities for the patients who died were found, and the observed mortality proportions were determined for the decile groups, along with 95% confidence intervals, and plotted. A perfectly predictive nomogram should result in the observed and expected probabilities falling along the 45° line.
Results
The total number of patients included in the study was 5,481 (weighted frequency of n = 26,958). The mean age of our sample was 64.9 (range, 18–98) with males accounting for 51% of the patients. The number of patients included in samples A and B were 4,482 (weighted n = 21,981) and 999 (weighted n = 4,977), respectively. The overall perioperative mortality rate for the entire cohort of patients was 6.1%. The perioperative mortality rate for samples A and B was 6.3% and 5.2%, respectively.
Tables 2 and 3 show the demographic, hospital, tumor characteristics, and preoperative comorbidity details for samples A and B as well as the estimated perioperative mortality rates. The distribution of patient characteristics is similar between samples A and B sets. There are some differences in the significance level of perioperative mortality comparisons between samples A and B, but the majority of these differences are probably due to smaller sample sizes in the 2005 dataset.
Table 4 shows the results of the multivariate models used to predict perioperative mortality using the 2000–2004 dataset (sample A). Variables selected for the multivariate model were chosen from a combination of clinical experience and statistical significance. If the variable was significant at the 0.05 level from the univariate chi-square tests presented in Tables 2 and 3, they were included in the model. If they were not significant at the 0.05 level but deemed important based on clinical experience, they were also included in the model. Due to the overlap in the ICD-9 codes, statistical requirements, and to keep the nomogram simple, we used the pancreatectomy codes for “distal,” “radical,” and “other” only for inclusion. Presented are adjusted odds ratios with 95% confidence intervals, the β coefficient and standard error, the Wald p value, and the total points for that variable estimated from the multivariate logistic model. These variables were used to construct a nomogram as shown in Fig. 1. For each patient, all the variables will be plotted in the nomogram to calculate the total number of points. The total points are now added to obtain an estimate of the likely perioperative mortality following pancreatectomy. For example, a patient seen in our clinic with the preoperative comorbidities as shown in Fig. 2 will be assigned a total of 208.2 points that translates to a nomogram-predicted perioperative mortality of approximately 18%.

The constructed nomogram.

An example of using the nomogram. This 68-year-old female patient seen in our clinic with multiple shown preoperative comorbidities has a total of assigned points of 208.2 that translates to a nomogram-predicted perioperative mortality rate of approximately 18%.
Validation of the Nomogram
The total number of points was calculated for each patient in sample A (2000–2004 dataset). The mean total points for the entire sample A is 131.7 (SE = 1.54) and ranges from 7.7 to 339.8. The mean total points for sample A of 131.7 correspond to approximately a 5% nomogram-predicted perioperative mortality rate which is similar to the actual observed perioperative mortality rate of 6.3%. The nomogram was validated using the NIS 2005 dataset (sample B). The mean total points for sample B is 128.1 (SE = 1.62) and ranges from 7.7 to 367.9. This approximates to a nomogram-predicted perioperative mortality rate of 4.6%, which is close to the actual observed perioperative mortality rate of 5.2%. The concordance index was found to be excellent at 0.76 with a 95% confidence interval of 0.69 to 0.83.
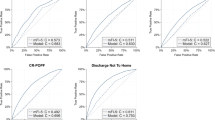
In addition to the concordance index, we performed validation of the nomogram by creating calibration plots. Calibration of the nomogram was examined by looking at the observed perioperative mortality versus the model-predicted perioperative mortality. First, we looked at the 2000–2004 data (sample A) that were used to build the nomogram (Fig. 3). The predicted probabilities extend from a minimum of 0.0054 to a maximum of 0.687. The observed perioperative mortality rates were calculated for the predicted probability deciles along with 95% confidence intervals and plotted against the predicted probabilities. There is excellent agreement between the observed and predicted probabilities. In the validation set, sample B (Fig. 4), the predicted probabilities extend from a minimum of 0.0054 to a maximum of 0.786. The observed perioperative mortality rates were calculated for the predicted probability quartiles along with 95% confidence intervals and plotted against the predicted probabilities. There is excellent agreement between the observed and predicted probabilities for the last three quartiles and a slight over estimate of the mortality rate in the first quartile.

Validation of sample A (2000–2004).

Validation of sample B (2005).
Discussion
The majority of patients that present with pancreatic malignancies are elderly with likely multiple pre-existing comorbidities. The preoperative counseling to obtain consent is vital before subjecting this group of high-risk patients to complex pancreatic resections. It is during this counseling that the risks and benefits of the procedure are explained to provide the platform upon which an informed consent is obtained. The published perioperative mortality rates following pancreatectomy are conflicting and range from 1–2% (single-institution data) to 7–8% (population-based data).3–6 Asiyanbola et al.11 noted a similar discrepancy in perioperative mortality rate for hepatic resections between single-institution and population-based studies.
Similarly, the data on the effect of several variables on the perioperative outcome following pancreatectomy for malignancy are also conflicting. Sohn et al.12 analyzed their single-institution database of 727 patients and noted that pancreaticoduodenectomy can be safely performed in octogenarians with outcomes similar to younger patients. In an update on the single-institution data, Makary et al.13 concluded that pancreaticoduodenectomy can be safely performed in nonagenarians. In contrast, a population-based study from Texas14 found that unadjusted in-hospital mortality increased with increasing age from 2.4% (<60 years) to 11.4% (>80 years of age).
The benefit of undergoing resection at high-volume centers has led to regionalization of care for patients with pancreatic malignancies.15,16 The data are confusing in defining what is high volume and also whether volume should be defined based on the physician or the hospital. In a study of the National Inpatient Sample database, Meguid et al.17 noted that volume alone accounted for less than 2% of data variance in perioperative mortality following pancreatic resection. This led them to suggest that volume alone is an imperfect surrogate of outcomes. Similarly, Riall et al.18 noted significant variability even among high-volume centers reiterating that volume is not a reliable single measure of quality or outcomes following pancreatic surgery.
The current data make it difficult to estimate the individual risk for each particular patient. The ability to estimate the individual risk of perioperative mortality following pancreatectomy for malignancy is important for the patient as well as the surgeon. Nomograms are graphical devices or models that use algorithms or mathematical formulae to estimate the probability of an outcome and are optimized for predictive accuracy for each individual patient.19,20 Nomograms allow physicians to tailor decisions to the individual patient rather than applying a “one-size fits all” approach to medical decision-making. Nomograms permit the use of all the important available parameters or risk factors so that an accurate prediction model can be constructed. Nomograms allow continuous variables to remain continuous to maximize the predictive power. More importantly, nomograms can be continuously updated based on available new clinical information thereby adding to the accuracy of the predictions.
The benefit of post-operative nomograms in predicting long-term survival has been proven in patients with cancer of various organ systems.21–23 These nomograms obtained in the postoperative period consist of various known prognostic factors and are used to define and predict long-term outcome. Recently, we have seen the development of preoperative nomograms to predict the risk of complications associated with particular surgical procedures.24,25 Lin et al.24 developed a preoperative nomogram to predict complications associated with various types of breast reconstruction procedures following mastectomy. Lagarde et al.25 constructed a nomogram that can help predict the severity of complications in the preoperative setting for patients scheduled for esophagectomy. The aim of this study therefore was to develop and validate a nomogram consisting of easily available variables that can be utilized in the preoperative setting to counsel individual patients about the perioperative mortality associated with pancreatectomy for malignancy.
The results of our study revealed good correlation between the nomogram-predicted perioperative mortality rate and the actual observed perioperative mortality rate for both samples A and B. The concordance index was found to be 0.76 with a 95% confidence interval of 0.69 to 0.83 and is evident with the good agreement between the predicted and observed perioperative mortality rates. In addition, we found excellent agreement between the observed and nomogram-predicted perioperative mortality rates on the calibration plots for both samples A and B.
The variables selected for use in constructing the nomogram were based on statistical significance on multivariate analysis as well as clinical significance. The clinical variables included were the ones known to have a likely impact on clinical outcome. It is known that omitting clinically relevant variables can compromise predictive accuracy of the nomogram.9,26 Brennan et al.23 developed a prognostic nomogram for patients with adenocarcinoma of the pancreas that included several nonsignificant variables such as sex, margin status, number of negative nodes, and T stage. Although these included variables were not significant on multivariable analysis, the developed nomogram predictions discriminated better than the American Joint Commission on Cancer staging (0.64 vs 0.56, p < 0.001). Similarly, Wong et al.27 developed a prognostic nomogram for melanoma patients that included clinician-selected variables only based on their practical prognostic values.
There are several limitations to our study. The nomogram does not include some other known risk factors and perioperative variables such as ASA status, serum albumin, coronary artery disease, texture of gland, size of duct, and blood loss. Although these other variables are important determinants of outcome, some of this perioperative information is only available after the patient has already consented for the procedure. Similarly, the addition of more variables may increase the complexity and limit the universal applicability. The limitations of the utilized data source (NIS) allowed us to use the preoperative comorbidities as categorical variables rather than continuous variables. It is likely that a nomogram that incorporates them as continuous variables may be more beneficial. The purpose of this study was to develop a nomogram by using variables that are widely and easily available in the preoperative setting. This nomogram is not intended to substitute for experience of the surgeon or to replace the established process of obtaining an informed and shared consent. It is hoped that this nomogram will play an additional role in counseling these high-risk patients prior to surgery. The simplicity of using this nomogram in the preoperative clinic setting makes it easy for the individual patient to understand their individual estimated risk of the proposed procedure. In addition, this may also permit referring physicians without expertise in pancreatic surgery to counsel patients before referring to specialized institutions. The nomogram is currently available for use at the following website- http://www.unmc.edu/publichealth/pancreas_nomogram.html.
Conclusion
In summary, we have developed a preoperative nomogram to predict perioperative mortality following pancreatic resection for malignancy. The nomogram was developed by using variables that are easily and widely available in the preoperative setting. The ease of use of this nomogram will make it an additional tool in the preoperative counseling of these high-risk patients prior to obtaining an informed and shared consent. The value of this nomogram can be confirmed following external validation.
References
http://www.cancer.org/downloads/STT/Cancer_Statistics_2008.ppt—accessed March 2009.
http://www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf—accessed March 2009.
Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, Hodgin MB, Sauter PK, Hruban RH, Riall TS, Schulick RD, Choti MA, Lillemoe KD, Yeo CJ. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg 2006;10:1199–1210.
Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006;244:10–15.
Vin Y, Sima CS, Getrajdman GI, Brown KT, Covey A, Brennan MF, Allen PJ. Management and outcomes of postpancreatectomy fistula, leak and abscess: results of 908 patients resected at a single institution between 2000 and 2005. J Am Coll Surg 2008;207:490–498.
McPhee JT, Hill JS, Whalen GF, Zayaruzny M, Litwin DE, Sullivan ME, Anderson FA, Tseng JF. Perioperative mortality for pancreatectomy. A national perspective. Ann Surg 2007;246:246–253.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care 1998;36:8–27.
Research Triangle Institute. SUDAAN Language Manual, Release 10.0 Research Triangle Park. 2008.
Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol 2008;26:1364–1370.
Brittain E. Probability of coronary heart disease developing. West J Med 1982;136:86–89.
Asiyanbola B, Chang D, Gleisner AL, Nathan H, Choti MA, Schulick RD, Pawlik TM. Operative mortality after hepatic resection: are literature-based rates broadly applicable? J Gastrointest Surg 2008;12:842–851.
Sohn TA, Yeo CJ, Cameron JL, Lillemoe KD, Talamini MA, Hruban RH, Sauter PK, Coleman J, Ord SE, Grochow LB, Abrams RA, Pitt HA. Should pancreaticoduodenectomy be performed in octogenarians? J Gastrointest Surg 1998;2:207–216.
Makary MA, Winter JM, Cameron JL, Campbell KA, Chang D, Cunningham SC, Riall TS, Yeo CJ. Pancreaticoduodenectomy in the very elderly. J Gastrointest Surg 2006;10:347–356.
Riall TS, Reddy DM, Nealon WH, Goodwin JS. The effect of age on short-term outcomes after pancreatic resection: a population-based study. Ann Surg 2008;248:459–467.
Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Relation of perioperative deaths to hospital volume among patients undergoing pancreatic resection for malignancy. Ann Surg 1995;222:638–645.
Fong Y, Gonen M, Rubin D, Radzyner M, Brennan MF. Long term survival is superior after resection for cancers in high-volume centers. Ann Surg 2005;242:540–544.
Meguid RA, Ahuja N, Chang DC. What constitutes a “high-volume” hospital for pancreatic resection? J Am Coll Surg 2008;206:622.
Riall TS, Nealon WH, Goodwin JS, Townsend CM Jr, Freeman JL. Outcomes following pancreatic resection: variability among high-volume providers. Surgery 2008;144:133–140.
Eastham JA, Kattan MW, Scardino PT. Nomograms as predictive models. Semin Urol Oncol 2002;20:108–115.
Kattan MW. Comparison of Cox regression with other methods for determining prediction models and nomograms. J Urol 2003;170:S6–S9.
Kattan MW, Leung DH, Brennan MF. Postoperative nomogram for 12-year sarcoma-specific death. J Clin Oncol 2002;20:791–796.
Kattan MW, Karpeh MS, Mazumdar M, Brennan MF. Postoperative nomogram for disease-specific survival after an R0 resection for gastric carcinoma. J Clin Oncol 2003;21:3647–3650.
Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg 2004;240:293–298.
Lin KY, Johns FR, Gibson J, Long M, Drake DB, Moore MM. An outcome study of breast reconstruction: presurgical identification of risk factors for complications. Ann Surg Oncol 2001;8:586–591.
Lagarde SM, Reitsma JB, Maris AD, van Berge Henegouwen MI, Busch OR, Obertop H, Zwinderman AH, van Lanschot JJ. Preoperative prediction of the occurrence and severity of complications after esophagectomy for cancer with use of a nomogram. Ann Thorac Surg 2008;85:1938–1946.
Harrell FE Jr, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med 1996;15:361–387.
Wong SL, Kattan MW, McMaster KM, Coit DG. A nomogram that predicts the presence of sentinel node metastasis in melanoma with better discrimination than the American Joint Committee on Cancer staging system. Ann Surg Onc 2005;12:282–288.
Acknowledgments
The authors would like to extend their sincere thanks to Dr. Murray F Brennan for his kind review of the manuscript and valuable suggestions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. Keith D. Lillemoe (Indianapolis): I’d like to congratulate you for a great presentation. Your style of presentation and knowledge of the data were great. It was an outstanding job by a medical student.
The authors have constructed a nomogram based upon preoperative risk factors to predict perioperative mortality following pancreatic resection. The product of their efforts has been validated using a second patient sample from the same database. This work seems like a natural extension from prior publications from Memorial Sloan Kettering, the institution where the senior author, Dr. Are did his fellowship. Dr. Brennan and others at Memorial have constructed nomograms to predict the long term survival for many common tumors. The logic behind those nomograms is that they can be used to guide adjuvant therapy for patients at the greatest risk for recurrent disease.
I understand the reasons that you have provided us for this nomogram and how it might be useful, but, again, to bring up the point that was brought up on Saturday at the Pancreas Club, Karl Bilimoria from Northwestern has already demonstrated that we have a problem with people with resectable cancers of the pancreas being denied surgery, or even surgical consultation, because the opinions of either their primary care physicians or other physicians, that they are not surgical candidates.
This nomogram could provide ammunition for nonsurgeons to calculate their own predictions of mortality and potentially deny resectable patients the potential for surgery.
Is this really what we want, to take these decisions out of the hands of the surgeons and leave them in the hands of a non-surgeon who can evaluate a nomogram based on a series of risk factors that they can measure but without surgical judgment.
I know databases have limitations, but you’re missing a lot of important factors that might contribute to perioperative risk such as serum albumin, ASA class, weight loss, and coronary artery disease. You use size of hospital and teaching hospitals as a surrogate, but these factors do not necessarily reflect hospital volume or surgeon experience in pancreatic surgery. You also could have included Leap Frog criteria.
Finally, imitation is the highest form of flattery. At Saturday’s Pancreas Club meeting, Jennifer Tseng and her group presented an almost identical nomogram addressing the same points that you did, only with a different database.
Despite the fact that these are both very nice papers, I predict that I will never use them. Rather, I am going to sit down with the patient, going to look at all their comorbidities, at my own experience, and I am going to look at the tumor, and I am going to put all these points together, make the decision whether to offer the patient an operation. I am not going to make this decision based on a calculated nomogram, but surgical judgment and experience.
I have one final question. After using the nomogram to determine that the lady you described with an 18% mortality, Dr. Are, did you offer her an operation? And if you did, then I can’t believe you really are going to ever apply this nomogram.
Discussant
Dr. Sean Mulvihill (University of Utah, Salt Lake City, Utah): I think Dr. Lillemoe was a little hard on you. I think it actually would be useful to have a nomogram that you could use to sit down with a patient and predict mortality.
The problem with your study is that it’s not applicable to any individual hospital. So, for instance, in my own hospital, of the last 173 Whipple resections we have done there was one perioperative death, for a mortality rate of 0.7%. But in your inpatient sample, the mortality rate is far higher. So we couldn’t use your nomogram except to attribute an average mortality across the country. I think most of us would believe that the average results in the country are unacceptably poor right now.
The other weakness is that the inpatient sample is notoriously inaccurate at describing patient comorbidities. And if one looks, in contrast to your nomogram, at the model that we have previously published from the NSQIP program where the variables are more closely controlled, it’s quite different. And so I think your study is useful, but probably not the answer to this problem of prediction of outcome.
Closing discussant
Chantal Afuh: That is a good point. As Dr. Are mentioned, this is not a tool to replace experience. It is something that may be used to help discuss these risks with patients.
One may say to the patient, based on your health status, the comorbidities you have, you may have an increased risk, whether it be slightly increased risk to another patient who does not have these additional health concerns.
There definitely are some institutions that have better outcomes than the national average. It is possible that this is something you may not wish to use at your institution to replace what you all have done, but it may be useful to supplement the conversation you have with the patient so that they can better understand and provide informed consent.
Dr. Carlos Fernandez Del Castillo (Boston, MA): A quick comment as I rise and share Dr. Lillemoe’s concern that this study, as well as the one from the University of Massachusetts, could generate nihilism in terms of the applicability of pancreatic resection for patients with pancreatic cancer, and can be used as an argument against surgery.
Currently only 30% of pancreatic resections are done for pancreatic cancer. Many others are done for benign disease, like cystic tumors, where the risk profile could be very different, including a higher risk of fistula, which in turn can be a cause of death. So, I’m not really sure this is really generalizable.
Closing discussant
Chantal Afuh: That is a very good comment as well. The purpose of our nomogram, however, is to be used when patients do have a primary adenocarcinoma.
So this isn’t necessarily something that can be applicable at large to different disease conditions of the pancreas or periampullary conditions. It’s something to be used in this particular situation, which is perioperative mortality following pancreatectomy for pancreatic malignancy.
Rights and permissions
About this article
Cite this article
Are, C., Afuh, C., Ravipati, L. et al. Preoperative Nomogram to Predict Risk of Perioperative Mortality Following Pancreatic Resections for Malignancy. J Gastrointest Surg 13, 2152–2162 (2009). https://doi.org/10.1007/s11605-009-1051-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-009-1051-z