
Abstract
Background
When resecting hilar cholangiocarcinoma, the surgeon cannot visualize the hilar vessels through thick connective tissue known as the plate system. Little has been reported regarding the anatomical relationship between the plate system and the extrahepatic bile duct.
Methods
Twenty-five formalin-fixed cadaveric livers were dissected carefully and 7 were sectioned sagittally. The extent, composition, and distribution of the extrahepatic bile ducts within the system were investigated. The length between the confluence of the hepatic duct and the branch point of the segmental duct (level I) and the length between the branch point of the segmental duct and the segmental Glisson’s pedicle (level II) were measured.
Results
The plate system—composed of the hilar, cystic, Arantian, and umbilical regions—was easily separated from the hepatic parenchyma. Histologically, dense connective tissue with abundant capillaries, lymphatic vessels, and neural fibers were noted. Level I of B1pcp and B4a measured 13.0 and 14.7 mm, respectively. Level II measured 8.6 and 17.3 mm, respectively.
Conclusions
The bile ducts in the plate system correspond to the extrahepatic bile ducts and their lengths are variable for every segment. Knowing the lengths of the resectable extrahepatic bile ducts is useful for deciding which segment should be resected according to the cancerous invasion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is agreement in the literature for the hilar and upper bile duct carcinoma that whenever feasible, resection is the most appropriate treatment to allow for prolonged survival and a potential cure.1–5 Right and left hepatectomies were previously applied;6 however, postoperative hepatic failure caused by excessive liver resection is sometimes accompanied by poor hepatic function. One solution to this problem is to reduce the hepatic volume to be resected as much as possible. Complete resection of the caudate lobe is thought to be essential for a successful surgical strategy for treating hilar cholangiocarcinoma,1,7 and recent improvements in surgical techniques and discoveries in surgical anatomy of the hepatic hilum made it possible to perform a limited hepatectomy such as an isolated caudate lobectomy.8 On the other hand, the tumor-free margin is a common predictor of postoperative survival in multivariate analysis.2–5 Therefore, how to balance both the operative safety and the necessarily radical nature of the surgery is one of the most serious problems in patients with hilar cholangiocarcinoma and poor hepatic function. In such cases, knowledge of the delineation between resectable extrahepatic bile ducts and hepatic segments that need to be preserved is required. However, the surgeon cannot peer into the bile duct through the plate system, which is a fibrous connective tissue enveloping the hilar vessels. This article focuses on the surgical anatomy of the hepatic hilum with special attention to the relationship between the plate system and the extrahepatic bile duct.
Material and Methods
Thirty-two livers from adult cadavers were obtained from the Department of Anatomy, Yokohama City University School of Medicine. The agreements for the study had been obtained from all of the bereaved family members. These 25 livers were dissected carefully to visualize the plate system enveloping the hilar bile ducts and vessels, and 7 livers were sectioned sagittally. Fine dissection was performed using forceps by removing the hepatic parenchyma anteriorly. The hepatic veins, Glisson’s pedicles, the plate system, and all of Glisson’s pedicles of the caudate lobe (CL) were completely exposed. Seven livers were sectioned sagitally parallel to the inferior vena cava at serial 1 cm intervals. The hepatic hilum area of the three sectioned specimens was embedded in a paraffin block for H.E staining for histological examination. In addition, on the dissection samples, the branch point of each segmental (or subsegmental) bile duct was evaluated after opening them to periphery. The portal vein was also incised on its dorsal side to identify all of the portal branches of the caudate lobe from the inside. As indicated by Kumon et al.,9 the portal branches of the CL are defined as those originating from the main portal trunk, the right and left portal veins in this study. The caudate lobe was subdivided into the Spiegel lobe (SP) (occupying the left side of the ligamentum venosum), the paracaval portion (PCP) (surrounding the IVC), and the caudate process (CP) (the right inferior side of the right portal vein). The distance between the confluence of the hepatic duct and the branch-point of each segmental (subsegmental) bile duct was measured as level I, and the distance between the branch-point of each bile duct and that of each Glisson’s pedicle was measured as level II. The results were shown according to branching patterns of the posterior bile ducts, which were of the supraportal and infraportal types.
Result
Extent and Composition of the Plate System
The plate system is a fibrous connective tissue comprised of the hilar plate in the hepatic hilum, the umbilical plate enveloping the umbilical portion of the portal vein, the cystic plate in the gallbladder bed, and the Arantian plate covering the ligamentum venosum (Fig. 1). The hilar and the umbilical plate measured 30.8 ± 9.7 mm (mean±SD) on the right side and 41.8 ± 10.0 mm on the left side from the confluence of the hepatic duct (Fig. 2).

Anterior view of post dissection specimen. a The plate system was covering the hepatic hilum. The hilar plate was easily dissected from the hepatic parenchyma as a result of the absence of small branches arising from it, whereas Glisson’s pedicle was difficult to remove from the hepatic parenchyma as a result of the presence of small branches. RHV right hepatic vein, MHV middle hepatic vein, LHV left hepatic vein, FV fissure vein, GB gallbladder, CBD common bile duct, PV portal vein, GX Glisson’s of segment X, pcp paracaval portion. b Schema of the plate system. The plate system was composed of the hilar plate, the umbilical plate, the Arantian plate, and the cystic plate.

Diagram of the hepatic hilum. The bile ducts were running in the hilar and umbilical plates. They measured 30.8 ± 9.7 mm (mean±SD) on the right side and 41.8 ± 10.0 mm on the left side from the confluence of the hepatic duct. GB gallbladder, CBD common bile duct, PV portal vein, PHA proper hepatic artery, GX Glisson’s of segment X, pcp paracaval portion, cp caudate process, sp Spiegel lobe.
Glisson’s pedicle was continuous from the plate system, but the hilar plate was easily dissected from the hepatic parenchyma because of the absence of small branches arising from the hilar plate, whereas Glisson’s pedicle was difficult to remove from the hepatic parenchyma because of the presence of such small branches. Moreover, the portal vein, the hepatic arteries, and the bile ducts ran separately from each other in the plate system whereas they were gathered and bundled in Glisson’s pedicle.
The hilar plate was connected with the cystic plate at the right ventral edge, Glisson’s pedicles of the right lobe on the right side, Glisson’s pedicle of the CP at the right dorsal edge, and Glisson’s pedicle of the PCP on the cranial side. The umbilical plate was connected to the ligamentum teres hepatis on the ventral side and the Arantian plate on the dorsal side. Glisson’s pedicles of the medial and lateral segments branched from the umbilical plate, and in addition, Glisson’s pedicle of the SP, which had a very thin Glisson’s sheath compared to the others, just posterior to the point where the Arantian ligament was attached to the umbilical plate.
On the sagittal section of the posterior portion of the right portal vein (PP), the hilar and the cystic plates were enveloping the three vessels subtotally (Fig. 3). We identified three vessels running apart from each other in the hilar plate. At the confluence of the hepatic duct, the hilar plate formed a semicircular shape (Fig. 4). The anterior and posterior margins consisted the fusion line of the hepatic capsule and the hepatoduodenal ligament. The fusion line was thick in the ventral portion and thin in the dorsal portion. On the dorsal side of the hilar plate, there were small bile ducts of the CP and the SP. On the umbilical portion (UP), the umbilical plate was enveloping the portal vein and connected to the Arantian duct at the posterior aspect (Fig. 5). The presented case of the sagittal section had a variation of the infraportal bile duct of segment 3.

a Sagittal section of the posterior portion of the right portal vein. b The hilar and cystic plates were enveloping three vessels subtotally. RHV right hepatic vein, G7 Glisson’s of segment 7, BX bile duct of segment X, AX artery of segment X, RPV right portal vein.

a Sagittal section of the confluence of the hepatic duct. b The hilar plate formed a semicircular shape. The anterior and posterior margins consisted of a fusion line of the hepaic capsule and the hepatoduodenal ligament. White and black stars indicate orifices of the bile ducts of the posterior and anterior segments, respectively. IVC inferior vena cava, MHV middle hepatic vein, G1pcp Glisson’s of the paracaval portion, CL caudate lobe, CA cystic artery, CBD common bile duct, PV portal vein, CD cystic duct, RHA right hepatic artery.

a Sagittal section of the umbilical portion of the portal vein. b The umbilical plate was enveloping the portal vein connected to the Arantian duct in the posterior portion. The presented case had a variation of the infraportal bile duct of segment 3. White stars indicate orifices of the portal vein of segment 4. FV fissure vein, AD Arantian duct, Sp Spiegel lobe, UP umbilical portion, BX bile duct of segment X, AX artery of segment X.
Histological examination of the sagittal section of the porta hepatis revealed abundant connective tissue—including neural fibers, lymphatic vessels, small capillaries, and small bile ducts (Fig. 6). These structures were surrounding the portal triad and were clearly defined from the liver parenchyma by the fibrous tissue derived from the hepatic capsule. The connective tissue was dense in the hilar plate and gradually lessened toward the hepatoduodenal ligament.

Histological findings of sagittal section of the hilar plate (H.E. stain, original magnification ×40). There was abundant connective tissue including neural fibers (ne), lymphatic vessels (ly), small capillaries (c) and small bile ducts (b). The examined site is shown on the right upper schema.
Distribution of the Extrahepatic Bile Ducts in the Plate System
Among all of Glisson’s pedicles of the caudate lobe, segments 2 and 3 were examined, whereas only the major branches of the other segments were studied. Most of the second-order bile ducts and some of the third-order bile ducts were included in the plate system. Twenty cases of the posterior bile duct (Bp) were running on the cranial side of PP (=supraportal branch), whereas three cases of Bp and two cases of B6 were running on the caudal side of PP (=infraportal branch). The B4 drainage pattern was shown according to the Kawarada’s classification:10 type I (B4 joined the left hepatic duct [LHD] close to the hilar confluence), 5/25; type II (B4 joined the LHD far from the hilar confluence), 13/25; and type III (combined type), 7/25.
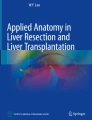
In the cases of supraportal posterior bile ducts, the distance between the confluence of the hepatic duct and each branch-point of the bile duct (level I) revealed bile ducts of the paracaval portion (B1pcp) as 13.0 mm, those of the posterior segment (Bp) as 13.2 mm, and those of segment 4a (B4a) as 14.7 mm (Fig. 7, Table 1). The distance between each branch-point of the bile duct and that of Glisson’s pedicle (level II) revealed B1pcp as 8.6 mm, which was the shortest, and B4a as 17.3 mm, which was the longest. The sum of level I and level II, which corresponds to the length between the confluence of the hepatic duct and the branch-point of the each Glisson’s pedicle revealed B1pcp as 21.6 mm, Bp as 29.6 mm, and B4b as 30.7 mm.

The length of the bile ducts in the plate system. Distance between the confluence of the hepatic duct and the branching point of each segmental (subsegmental) bile duct was measured as level I and distance between branching point of each bile duct and that of each Glisson’s pedicle was measured as level II.
In cases of infraportal posterior bile ducts, level II was longer than those of the supraportal cases, excluding B5a and B5b, and were statistically significant (p < 0.05) in the B1pcp, B4a and Bp (Table 2).
The length from the confluence of the hepatic duct to the right side of PP and the right side of UP, both of which were considered to be anatomical landmarks intraoperatively, measured about 25 and 30 mm, respectively.
Discussion
The plate system was originally mentioned by Walaneus et al. in 1620, but in relation to surgical anatomy, Couinaud et al. reported it precisely in 1957 and 1989.11,12 However, recent progress in surgical procedures for hilar cholangiocarcinoma requires more detailed anatomical knowledge of the plate system. Currently, there are many surgical procedures for hilar cholangiocarcinomas varying from local excisions to major hepatectomies, and the selection or indications of these procedures are difficult to determine, especially for patients with poor hepatic function. Therefore, we have to estimate the hepatic segments to be resected according to the cancerous invasion present in each case. In this paper, we focused on the relationship between the plate system and the bile duct, which is important for the selection of an appropriate operative procedure of hilar cholangiocarcinoma.
Numerous anatomical investigations about hepatic vessels using cast and radiological studies made remarkable progress in liver surgery and, in this decade, the surgical anatomy of the hepatic hilum (including the caudate lobe) was also clarified.12–17 However, the plate system’s contribution to the complexity of the hepatic hilum was difficult to investigate by such indirect methods. The dissection method used in this study was useful to identify the plate system as it would have been seen during actual operative procedures. Moreover, by adding the incision of bile ducts and portal vein, even small branches of the CL could be identified. The bile ducts of the CP and the SP are very small in diameter and run on the dorsal side of the hilar plate. Sagittal section examinations provided the three-dimensional information about the relationship between the plate system and the hilar vessels.
The edge of the plate system consists of the fusion line of the hepatoduodenal ligament and the hepatic capsule, based upon the findings of sagittal section examinations. Although there was not much connective tissue behind the portal vein compared to in front of it, it is reasonable to believe that it is part of the plate system because of the continuity from the anterior plate and the existence of small bile ducts draining from CP and SP. The plate system was continuous to Glisson’s pedicle intrahepatically, and Couinaud represented, in the schema of his literature, that the branch point of Glisson’s pedicles is the boundary of the plate system. We also defined the boundary of the plate system the same way, for the following two reasons.
First, the hepatic parenchyma was stuck to Glisson’s pedicle, but not to the plate system. Second, the arteries, the portal veins, and the bile ducts ran separately within the plate system, although close together in Glisson’s pedicle. Although cancer cells affect the bile duct in the plate system, the invaded bile duct can be resected without hepatic parenchymal resection for oncological reasons;18 however, if the cells involve Glisson’s pedicle, it is very difficult to resect the invaded bile duct alone. For resecting hilar cholangiocarcinoma, it is important to estimate whether cancerous invasion along the bile duct is within the plate system or not. Consequently, the bile ducts in the plate system correspond to the actual extrahepatic bile ducts. If cancerous invasion is beyond the plate system at a certain segment, the segment has to be removed with radical surgery.
In terms of the surgical aspects, the limits of the resectable extrahepatic bile ducts are considered to be approximately at the right edge of PP and right edge of UP, and the length from the confluence of the hepatic duct measured 25 and 30 mm, respectively. Most of the second-order bile duct branches and some of third-order branches are all included in the plate system.
In the operation of hilar cholangiocarcinoma, the plate system is the key anatomical structure in the hepatic hilum because extrahepatic bile ducts cannot be dissected from the plate system and the decision as to whether a certain hepatic segment should be removed or not depends on the relationship between cancerous invasion and the extension of the plate system. How much plate system we are able to preserve depends in part upon the selected surgical procedure. For example, in cases of supraportal posterior bile ducts, if cancer cells invade into the root of B1pcp and 10 mm of cancer-free length are necessary for surgical margin, the liver parenchyma of B1pcp has to be resected because its level II length is less than 10 mm. However, for segment B4a, the liver parenchyma of segment 4a possibly can be preserved because its level II length is over 15 mm. Between the supraportal and infraportal type level II lengths, the infraportal type were longer (excluding B5a and B5b). Therefore, in the infraportal type left lobe, the paracaval portions and posterior segments were relatively preservable segments. Thus, understanding the relationship between the plate system and the bile duct is useful for determining the degree of possible hepatic parenchymal preservation. The result of level I+II of B1pcp shows a length of 21.6 mm, which is remarkably short compared to other bile ducts. It is consistent with the fact that the CL is the most frequently involved segment in the liver, and it is also proof of the necessity of caudate lobe resection for hilar cholangiocarcinomas.
Our results provide new information about the surgical anatomy of the hepatic hilum with special attention to the plate system. Furthermore, this information is useful for appropriate selection of an operative procedure in patients with hilar cholangiocarcinoma and poor hepatic function.
Abbreviations
- CL:
-
caudate lobe
- H.E.:
-
hematoxylin eosin
- SP:
-
Spiegel lobe
- PCP:
-
paracaval portion
- IVC:
-
inferior vena cava
- CP:
-
caudate process
- PP:
-
posterior portion of the right portal vein
- UP:
-
umbilical portion of the left portal vein
- LHD:
-
left hepatic duct
- RHV:
-
right hepatic vein
- MHV:
-
middle hepatic vein
- LHV:
-
left hepatic vein
- FV:
-
fissure vein
- GB:
-
gallbladder
- CBD:
-
common bile duct
- PV:
-
portal vein
- GX:
-
Glisson’s of segment X
- BX:
-
bile duct of segment X
- AX:
-
artery of segment X
- pcp:
-
paracaval portion
- PHA:
-
proper hepatic artery
- cp:
-
caudate process
- sp:
-
Spiegel lobe
- RPV:
-
right portal vein
- CA:
-
cystic artery
- CD:
-
cystic duct
- AD:
-
Arantian duct
- ne:
-
neural fibers
- ly:
-
lymphatic vessels
- c:
-
small capillaries
- b:
-
small bile ducts
References
Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma. Ann Surg 1992;215:31–38.
Neuhaus P, Jonas S, Bechstein WO, Lohmann R, Radke C, Kling N, et al. Extended resections for hilar cholangiocarcinoma. Ann Surg 1999;230:808–819.
Klempnauer J, Ridder GJ, von Wasielewski R, Werner M, Weimann A, Pichlmayr R. Resectional surgery of hilar cholangiocarcinoma: a multivariate analysis of prognostic factors. J Clin Oncol 1997;15:947–954.
Su CH, Tsay SH, Wu CC, Shyr YM, King KL, Lee CH, et al. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann Surg 1996;223:384–394.
Pichimayr R, Weinmann A, Klempnauer J, Oldhafer KJ, Maschek H, Tusch G, et al. Surgical treatment in proximal bile duct cancer. Ann Surg 1996;224:628–638.
Boerma EJ, Bronkhorst FB, van Haelst UJGM, de Boer HHM. An anatomic invastigation of radical resection of tumor in the hepatic duct confluence. Surg Gynecol Obstet 1985;161:223–228.
Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg 1990;14:535–544.
Bartlett D, Fong Y, Blumgart LH. Complete resection of the caudate lobe of the liver: technique and results. Br J Surg 1996;83:1076–1081.
Kumon M. Anatomy of the caudate lobe with special reference to portal vein and bile duct. Acta Hepatol Jpn 1985;26:1193–1199.
Kawarada Y, Das BC, Onishi H, Taoka H, Gadzijev EM, Ravnik D, et al. Surgical anatomy of the bile duct branches of the medial segment (B4) of the liver in relation to hilar carcinoma. J Hepatobiliary Pancreat Surg 2000;7:480–485.
Couinaud C. Le Foie: Etudes Anatomiques et Chiruricales. Paris: Masson, 1957.
Couinaud C. Surgical Anatomy of the Liver Revisited. Paris: C. Couinaud, 1989.
Kogure K, Kuwano H, Fujimaki N, Makuuti M. Relation among portal segmentation, proper hepatic vein, and external notch of the caudate lobe in the human liver. Ann Surg 2000;231:223–228.
Kumon M. Anatomy of the caudate lobe with special reference to portal vein and bile duct. Acta Hepatol Jpn 1985;26:1193–1199.
Couinaud C. The paracaval segments of the liver. J Hepatobiliary Pancreat Surg 1994;2:145–151.
Mizumoto R, Suzuki H. Surgical anatomy of the hepatic hilium with special reference to the caudate lobe. World J Surg 1988;12:2–10.
Togo S, Shizawa R, Kanemura E, Tanaka K, Masunari H, Endo I, et al. Usefulness of 3-dimentional computed tomography for caudate lobectomy by transhepatic anterior approach. Hepatogastroenterology 2002;49:461–466.
Shimada H, Endo I, Fujii Y, Kunihiro O, Tanaka K, Misuta K, et al. Procedure of extended hilar bile duct resection and its application for hilar cholangiocarcinoma. Hepatogastroenterology 2002;49:300–305.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Masunari, H., Shimada, H., Endo, I. et al. Surgical Anatomy of Hepatic Hilum with Special Reference of the Plate System and Extrahepatic Duct. J Gastrointest Surg 12, 1047–1053 (2008). https://doi.org/10.1007/s11605-007-0358-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0358-x