
Abstract
Background
This study was designed to evaluate the survival outcomes of patients undergoing simple cholecystectomy and to investigate which patients would benefit from cholecystectomy alone in treating gallbladder carcinoma.
Methods
The available medical records of patients who underwent cholecystectomy alone for gallbladder carcinomas from August 1992 to February 2005 were retrospectively reviewed. Cancer stages were evaluated by clinical meaning based on the AJCC Cancer Staging Manual, 6th edition. “Clinical” R0, defined as gallbladder confined tumor (pT1-3 with negative resection margin) with cN0 and cM0, was tentatively established to evaluate the quality of simple cholecystectomy.
Results
Seventy-five patients underwent cholecystectomy alone for gallbladder carcinomas. Twenty-eight patients were male, and forty-seven patients were female, with their mean age 63.5 years (range, 29-80 years). Forty-one patients (54.7%) underwent laparoscopic cholecystectomy, and thirty-four patients (45.3%) underwent open cholecystectomy. T3 lesions were most common (26 patients), followed by T1 (24 patients), T2 (19 patients), and T4 (6 patients). “Clinical R0” could be defined in 48 patients (63%) after simple cholecystectomy. Multivariate analysis showed that incidental gallbladder carcinoma, T stage, and clinical R0 status were independent prognostic factors of long-term survival. When comparing survival outcomes of clinical R0 according to the T stage, no patients with Tis, T1a, and T1b had cancer-related mortality during follow-up. Especially, in patients with T2 gallbladder carcinomas, the mean survival rate was 68.9 months, and the 5-year survival rate was 77.8%. On the contrary, those with T3 lesions had poor prognoses.
Conclusion
Cholecystectomy alone could be proper management for well-selected patients with gallbladder carcinomas (incidental gallbladder carcinoma, gallbladder confined carcinoma, clinical R0). More experiences and a proper prospective study must be performed to confirm the meaning of clinical R0 in treating gallbladder carcinoma.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Gallbladder carcinomas were first described by Maxmillian de Stoll in 1777.1 Gallbladder carcinoma is the most frequent malignant neoplasm of the biliary tract and the fifth most common cancer of the gastrointestinal tract.2 There is still controversy about surgical treatment of gallbladder carcinomas. Generally, cholecystectomy alone is an adequate treatment for pathologic stage T1 (pT1) gallbladder carcinoma, providing that the resection margins are not violated by malignant cells.3–5 On the other hand, radical resection with regional lymph node dissection for T2 or more advanced gallbladder carcinoma is advocated.6 However, Shirai et al.7 reported that about 40.5% of patients with T2 gallbladder carcinomas survived more than 5 years after cholecystectomy alone, which implies that radical surgery is too much for patients with such favorable prognoses.
According to anecdotal experiences at our institution, simple cholecystectomy in certain patients is likely to provide an acceptable surgical outcome compared to radical surgery in treating gallbladder carcinoma. This observation prompted us to plan this study. This retrospective study was designed to evaluate the results of simple cholecystectomy in treating gallbladder carcinoma and to investigate which patients would benefit from simple cholecystectomy in treatment of gallbladder carcinoma.
Materials and Methods
The medical records of patients with gallbladder carcinomas who underwent surgical procedures at the Yonsei University Health System, in Seoul, Korea, between August 1992 and February 2005 were retrospectively reviewed. We selected patients who underwent simple cholecystectomies for gallbladder carcinomas. We investigated the survival results and clinical predictive factors for favorable survival outcomes after simple cholecystectomy in treating gallbladder carcinomas. Incidental gallbladder carcinoma was defined as carcinoma of the gallbladder first diagnosed at the histological examination of the resected gallbladder or gallbladder mass detected during a medical checkup without any symptoms. The clinical TNM (cTNM) stage was evaluated based on the AJCC Cancer Staging Manual; 6th edition.8 cTNM classification is based on evidence acquired before treatment, including physical examination, image study, endoscopy, biopsy, and surgical exploration. Nodal status was determined by preoperative image studies or histological examination of incidentally sampled lymph nodes during simple cholecystectomy. We tentatively developed an additional criterion, “clinical” R0, to evaluate the quality simple cholecystectomy cases, which was defined as no malignant cells on gallbladder resection margins in the pathologic report, no grossly residual tumors, no lymph node enlargement, and no distant metastasis based on image studies and operative findings [that is, gallbladder confined tumor (pT1-3 with negative resection margin), cN0 and cM0]. R1 was defined as the presence of a microscopic residual tumor (positive resection margin), and R2 as the presence of a macroscopic residual tumor. To delineate the characteristics of gallbladder carcinoma treated by cholecystectomy alone, we compared cases of patients who underwent radical cholecystectomies during the same period to those of patients who underwent simple cholecystectomies by T stage. The standard radical operation in our department is composed of at least wedge resection of the gallbladder bed including about 2 cm thickness of liver parenchyma, resection of soft tissue along the hepatoduodenal ligament with or without bile duct resection, and dissection of regional nodes from the hepatic artery to the extent of the right side of the celiac axis with retroperitoneal soft tissue clearance (16A2, 16B1). However, slight modifications of the extent of surgery according to the patient’s general conditions, tumor factors, and the surgeon’s preference were made. Statistical analysis was performed using SPSS software (Statistical Package for the Social Sciences, version 10.0). The categorical variables are expressed as frequencies (%), whereas continuous variables are presented as a mean with their range or ± standard deviation. Follow-up data were obtained from medical records and patient or family member telephone interviews. Survival was calculated from the date of diagnosis to the date of death or last follow-up. Cumulative survival rates and plots were estimated using the Kaplan-Meier method. The log-rank test was applied to check for statistical significance. Cox multivariate analyses were performed to determine the independent prognostic factors for survival. Differences in p value less than 0.05 were considered significant.
Results
General Characteristics of Patients
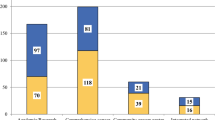
Between August 1992 and February 2005, a total of 217 patients with gallbladder carcinomas underwent surgical procedures at our institution. Among them, 75 patients underwent cholecystectomy alone for gallbladder carcinomas. Twenty-eight patients were male, and forty-seven patients were female. The mean age at time of surgery was 63.5 years (range, 29–80 years). Forty-six patients (62.2%) had incidental gallbladder carcinomas. Abdominal pain and discomfort were the most frequent symptoms, found in 48 patients (63.2%). Gallstone disease was associated in 34 patients (48.6%), and GB empyema was noted in 10 patients (14.5%). Forty-one patients (54.7%) underwent laparoscopic cholecystectomy, and thirty-four patients (45.3%) underwent conventional open cholecystectomy. Five operation-related complications (6.6%) occurred. Bile leak was found in three patients, bleeding in one, and wound infection in one patient; however, there were no mortalities (<30 days after cholecystectomy alone).
Characteristics of Gallbladder Carcinoma
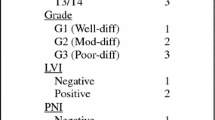
All gallbladder carcinomas were adenocarcinomas. Polypoid tumors were mainly located in the distal part of the gallbladder (fundus and body, more than 60%). T3 lesions were the most common (26 patients), followed by T1 (24 patients) and T2 (19 patients). Left supraclavicular lymph nodes (two patients), liver metastasis (three patients), and peritoneal seeding (positive rectal shelf, one patient) were present in six cases of distant metastasis at the time of surgery. Clinical R0 could be defined in 48 patients (63.2%) after simple cholecystectomy (Table 1).
Prognostic Factors for Favorable Survival Outcomes: Univariate Analysis
Overall survival of patients with gallbladder carcinomas who underwent simple cholecystectomy was mean 80.2 months with a 5-year survival rate of 47.9%. The survival differences according to T stage were statistically significant, as shown in Table 2 (p < 0.0001). The 5-year survival rate of patients with gallbladder carcinomas with Tis, T1b, and T2 lesions was 100, 75, and 56.2%, respectively. Residual tumor status after simple cholecystectomy alone significantly influenced survival differences. That is, considerable survival differences between clinical R0 and R1 or R2 were noted (clinical R0 vs R2, p < 0.0001, and clinical R0 vs R1 p = 0.0045). In addition, clinical lymph node metastasis and distant metastasis, tumor grade, tumor morphology, and incidental gallbladder carcinoma were all significant prognostic factors in univariate analysis (p < 0.05, Table 2).
Prognostic Factors for Favorable Survival Outcomes: Multivariate Analysis
When multivariate analysis (Cox regression) is performed using variables with significant survival differences in univariate analysis as covariates, incidental gallbladder carcinoma (p = 0.011), T-stage (p = 0.004), and R status (p = 0.041) were independent prognostic factors for good survival outcomes after simple cholecystectomy in patients with gallbladder carcinomas (Table 2).
Analysis of Clinical R0 Status
Forty-eight patients (61.2%) were defined as having clinical R0 after cholecystectomy alone. With the advancement of T stage, the frequency of R1 and R2 increases (Table 3). Almost all early gallbladder carcinomas (T1) were defined as clinical R0 after simple cholecystectomy alone; however, frequently, R1 and R2 resulted from simple cholecystectomy in patients with gallbladder carcinomas more advanced than T2 lesions.
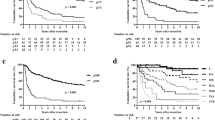
When comparing survival outcomes of clinical R0 according to T stage, significant differences were noted (Fig. 1). No patients with Tis, T1a, and T1b lesions had cancer-related mortality after simple cholecystectomy. Especially, patients with T2 gallbladder carcinomas showed acceptable survival outcomes after cholecystectomy alone. Their mean survival was 68.9 months, and the 5-year survival rate was 77.8%. To the contrary, those with T3 lesions had relatively poor prognoses. Their mean survival was 32.8 months with a 5-year survival rate of 14.6%, which were considerably different from patients with T1 and T2 gallbladder carcinomas with clinical R0 (Fig. 1).

Survival outcomes of clinical R0 according to T stage after simple cholecystectomy.
When comparing the survival outcomes according to R status after surgery in patients with T2 and T3 gallbladder carcinomas, no survival differences were noted between patients whose carcinomas were defined as clinical R0 and R0 resulting from radical cholecystectomy (Figs. 2 and 3).

Survival differences between clinical R0 and R0 in T2 gallbladder carcinoma.

Survival differences between clinical R0 and R0 in T3 gallbladder carcinoma.
Comparison of Simple Cholecystectomy and Radical Cholecystectomy at our Institution (Yonsei University Health System, Seoul, Korea)
One hundred and seven cases of radical cholecystectomy during the same period were compared with current simple cholecystectomized cases. A high incidence of cholecystitis including empyema, incidental diagnosis, shorter operative time, less bleeding, lower incidence of blood transfusion, and complications were noted in patients who underwent simple cholecystectomies compared to the patients who underwent radical cholecystectomies (Table 4).
Discussion
Gallbladder carcinoma is known as a highly fatal disease with a poor prognosis. The 5-year survival rate for patients with cancers of the gallbladder ranges from 0% to 10% in most reported series.9 The poor prognosis of this disease may be caused by the anatomical position of the gallbladder and the high proportion of tumors that are advanced at the time of presentation. Gallbladder carcinoma is difficult to diagnose clinically because the symptoms and signs are vague and nonspecific. However, early diagnosis of gallbladder carcinoma has increased because of the recent improvement of preoperative imaging10–12 and increased concerns about people’s own health status in accordance with improving personal economic status. In addition, clinical application of extensive radical surgery promises an improvement in survival.13, 14
Generally, simple cholecystectomy is accepted as the proper treatment for Tis and T1a gallbladder carcinomas. In the case of T1b lesions, despite the controversy, simple cholecystectomy is likely to be recommended. Wakai et al.3 recently suggested that cholecystectomy alone could be a standard treatment for T1b gallbladder carcinoma as cholecystectomy provides patients with a 10-year survival rate of more than 85%. Whereas on the other hand, radical cholecystectomy is strongly recommended for patients whose gallbladder carcinomas are staged as more severe than T2 lesions.15 Shirai et al.7 reported a 5-year survival rate of 90% after patients underwent radical resection for T2 and T3 tumors compared with a 5-year survival rate of only 40% for patients who underwent simple cholecystectomies. De Aretxabala et al.16 showed a 50% improved 5-year survival rate (70 vs 20%) for patients who underwent radical cholecystectomies versus patients who underwent simple cholecystectomies. Fong et al.17 reported a 5-year survival rate of 61% for patients with T2 tumors who underwent radical cholecystectomies compared with a 5-year survival rate of only 19% for patients with T2 tumors who underwent simple cholecystectomies. Furthermore, support for radical resection of locally advanced disease also has been accumulated during the past decade. Five-year survival rates of 15 to 63% and 7 to 25% have been reported for T3 and T4 gallbladder carcinomas, respectively.6
Although the number of patients with gallbladder carcinomas is limited and our clinical data are based on retrospective observation, which might have had unavoidable selection bias, the results of simple cholecystectomy were not disappointing and seemed to be comparable to previous reports. The 10-year survival rate of T1b tumors was 75%, and the 5-year survival rate of patients with T2 lesions was 56.2%. Especially, the result of patients with T2 lesions is superior to the results of patients who underwent simple cholecystectomies in the abovementioned literature.7,15,17 Then, we hypothesized that this selection bias could be, in other words, a sort of selection criterion for simple cholecystectomy in the treatment of gallbladder carcinoma. Therefore, the purpose of our clinical observation is to reveal possible selection criterion for simple cholecystectomy in gallbladder carcinoma. In fact, this study was performed to evaluate the results of simple cholecystectomies, and we would like to find which patients could benefit from simple cholecystectomy as a treatment for gallbladder carcinoma.
According to our results (Table 4), an overall comparison of patients who underwent simple cholecystectomies and radical cholecystectomies according to T stage shows that less substantial morbidity, shorter operative times, smaller bleeding amount, and lower incidence of transfusion were noted in patients who underwent simple cholecystectomies, which means that limited surgery in patients with gallbladder carcinomas is beneficial. If the oncologic outcomes were comparable in patients who underwent simple cholecystectomies in well-selected cases of patients with gallbladder carcinomas, more extended surgery, which always brings a risk of postoperative morbidity and mortality, could be avoided in the selected population.
The highlight of this study might determine the validity of clinical R0 as a selection criterion for the choice of simple cholecystectomy. To some extent, clinical R0 apparently seems to reflect the status of the TNM stage. As mentioned above, we defined clinical R0 as when the resected gallbladder showed a negative margin on histopathologic examination, preoperative radiologic images revealed neither distant metastasis nor metastatic lymph node, and intraoperative findings showed no evidence of grossly residual tumors. From the viewpoint of this definition, advanced cases of T3, T4, N1, and M1 tumors have a high possibility of being excluded from clinical R0. On the other hand, not only early lesions, T1, but also some portions of T2 tumors have a high chance of being included as clinical R0. As a matter of fact, our results show that most gallbladder carcinomas actually fall into clinical R0 in cases of early lesions, Tis, T1a, and T1b. In the case of T2 lesions, about 74% of these lesions (14 out of 19 patients) fall into clinical R0. However, no T4 lesions could be considered clinical R0, and 48% of the T3 lesions (12 out of 25 patients) fall into clinical R0 (Table 3).
The survival outcomes of patients with clinical R0 gallbladder carcinomas were acceptable for patients with T1 and T2 tumors (Fig. 1). No cancer-related mortality was observed in any patients with Tis, T1a, and T1b tumors with clinical R0. Especially, with respect to 14 patients with T2 gallbladder carcinomas with clinical R0 (73.7%), the 5-year survival rate was 77.8%. Interestingly, this result is definitively superior to recent survival outcomes of patients who underwent simple cholecystectomies. Fong et al.17 reported that patients with radiographically resectable disease but not subjected to repeat resection after undergoing simple cholecystectomies had a 5-year survival rate of 19%, whereas those treated with radical resection had a 5-year survival rate of 61%, which emphasizes that radical resection is not only safe but reasonable cancer therapy for those with T2 gallbladder cancers. Suzuki et al.18 reported an overall 5-year survival rate in those 20 patients with T2 gallbladder carcinomas of 77% and also concluded that a radical second operation enhanced the chance for cure in patients with T2 gallbladder carcinomas. However, according to the present results of survival comparison in T2 gallbladder carcinomas, clinical R0 and R0 from radical surgery have no considerable survival differences (Fig. 2). To the contrary, the prognosis for patients with T3 lesions with clinical R0 was relatively poor, compared to patients with either T1 or T2 lesions with clinical R0. According to our results, the 5-year survival rate of patients with pT3 gallbladder carcinomas with clinical R0 was 14.6%, which is significantly different from that of patients with pT2 lesions (Fig. 1, p = 0.011). In addition, when comparing the survival rates according to R status after surgery in patients with T3 lesions, the survival outcome of patients with clinical R0 was apparently inferior to that of patients with R0 from radical surgery (Fig. 3). Although the differences between the two groups have no statistic meaning, the statistical power seems to be too weak to support the survival comparativeness (p = 0.0655). Consequently, we would like to emphasize that, unlike gallbladder carcinoma with T2 lesions, the value of clinical R0 in T3 gallbladder carcinoma cannot be guaranteed; therefore, additional or initial radical surgery should be considered for patients with T3 lesions to secure the negative resection margin and to control microscopic extension to the soft tissues, which could not be detected by macroscopic and radiological findings.
The concept of clinical R0 was tentatively used in this study to evaluate the surgical results after simple cholecystectomy. The critical drawback of this concept is that we cannot truly evaluate the microscopic lymph node metastasis, which could be definitively investigated in extended radical surgery. For example, about 30 to 40% of patients with T2 gallbladder carcinomas are known to have lymph node metastasis. In turn, these patients can lose the chance for long-term survival provided by radical surgery. Therefore, for the purposes of clinical application of this concept, we might need to design another clinical study that compares preoperatively predictive clinical R0 and pathologically provided residual tumor status in the same patients with gallbladder carcinomas.
The current study has unavoidable weak points in the analysis of the data. First, this study is based on retrospective available medical records, which means it is difficult to find the proper reasons why surgeons did not perform additional surgery with curative intent after simple cholecystectomies in patients with T2 and T3 lesions. Second, more than four surgeons were involved in treating gallbladder carcinomas according to the history of our department. We must take surgeon factors into account when comparing the results of radical surgery and simple cholecystectomy. Different extents of lymph node dissection and liver resection must also be considered in data analysis. However, our retrospective observations suggest that the survival results of patients who underwent simple cholecystectomies were acceptable for patients with T1 and T2 lesions with “clinical” R0 and provoke the possible role of simple cholecystectomy in well-selected patients with T2 lesions.
Conclusion
We carefully concluded that patients with incidentally detected gallbladder carcinomas could be expected to have good prognoses after undergoing simple cholecystectomy alone without additional radical surgery, as long as clinical R0 is ensured. However, we could not guarantee the validity of clinical R0 in patients with T3 lesions; therefore, radical cholecystectomy is warranted in such cases. More experiences and proper prospective study must be performed to validate surgical meaning of clinical R0 in treating gallbladder carcinomas.
References
Destoll M. Rationis mendendi. In Batavorum L, Haak ET Socios A et J Honkoop, ed. Nosocomio practico vendobonensi, Part I, 1788.
DeRegato JA, Spjut HJ. Digestive tract/accessory organo-gallbladder. In Ackerman LV, DeRegato JA, (eds). Cancer-Diagnosis, Treatment and Prognosis, 5th ed. St Louis: CV Mosby, 1977, pp 599–604.
Wakai T, Shirai Y, Yokoyama N, Nagajura S, Watanabe H. Early carcinoma of the gallbladder. Eur J Surg 1992;158:545–548.
Togoroki T, Kawamoto T, Takahashi H, et al. Treatment of gallbladder cancer by radical resection. Br J Surg 1999;86:622–627.
Bartlett DL, Fong Y, Fortner JG, Brennan MF, Blumgart LH. Long-term results after resection for gallbladder cancer: implications for staging and management. Ann Surg 1955;142:6–16.
Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol 2003;4:167–176.
Shirai Y, Yoshida K, Tsukada K, Muto T. Inapparent carcinoma of the gallbladder: an appraisal of a radical second operation after simple cholecystectomy. Ann Surg 1992;2155:326–331.
Frederick LG, David LP, Irvin DF, et al. AJCC Cancer Staging Manual, 6th ed. Philadelphia: Lippincott-Raven; 2002.
Piehler JM, Crichlow RW. Primary carcinoma of the gallbladder. Surg Gynecol Obstet 1978;929–942.
Chijiwa K, Sumiyoshi K, Nakayama F. Impact of recent advances in hepatobiliary imaging techniques on the preoperative diagnosis of carcinoma of the gallbladder. World J Surg 1991;15:323–337.
Ueno N, Tomiyama T, Tano S, et al. Diagnosis of gallbladder carcinoma with color Doppler ultrasonography. Am J Gastroenterol 1996;91:1647–1649.
Azuma T, Yoshikawa T, Araida T, Takasaki K. Differential diagnosis of polypoid lesions of the gallbladder by endoscopic ultrasonography. Am J Surg 2001;181:65–70.
Shoup M, Fong Y. Surgical indications and extent of resection in gallbladder cancer. Surg Oncol Clin N Am 2002;11:285–294.
Sasaki R, Itabashi H, Fujita T, et al. Significance of extensive surgery including resection of the pancreas head for the treatment of gallbladder cancer-from the perspective of mode of lymph node involvement and surgical outcome. World J Surg 2006;30:36–42.
Fong Y. Treatment of T2 gallbladder carcinoma. Ann Surg Oncol 2003;10:490.
De Aretxabala X, Roa IS, Burgos LA, et al. Curative resection in potentially respectable tumors of the gallbladder. Eur J Surg 1997;163:419–426.
Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention. Ann Surg 2000;232:557–569.
Suzuki S, Yokoi Y, Kurachi K, et al. Appraisal of surgical treatment for pT2 gallbladder carcinomas. World J Surg 2004;28:160–165.
Acknowledgement
We give special thanks to Seo Won. Youl (Biostatistical Supporting Laboratory Yonsei University College of Medicine) for so much advice in analyzing biostatics data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kang, C.M., Lee, W.J., Choi, G.H. et al. Does “Clinical” R0 Have Validity in the Choice of Simple Cholecystectomy for Gallbladder Carcinoma?. J Gastrointest Surg 11, 1309–1316 (2007). https://doi.org/10.1007/s11605-007-0225-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0225-9