
Abstract
Background
Radio frequency ablation (RFA) of hepatocellular carcinoma has proved to be useful in local control of tumor. A few data on survival after treatment are available in literature. The aim of the study was to evaluate factors related to survival and to identify different classes of risk after radio frequency ablation.
Methods
Ninety-eight cirrhotic patients with 145 hepatocellular carcinomas were treated with radio frequency ablation from January 1998 to May 2004. In 55 patients, cirrhosis was in Child-Pugh class A, and in 43, in class B. Tumor was single in 60 and multiple in 38; mean tumor number was 1.5 (range 1–3). Tumor size ranged from 1.5 to 6.0 cm, mean 3.8 cm. Mean follow up period was 24.9 months. Radio frequency ablation was performed with expandable type needle with percutaneous approach under real-time ultrasound guidance. For statistical analysis, univariate and multivariate analysis were performed.
Results
Complete ablation of the tumor was achieved in 85.5% of lesions. Survival, 1 and 3 years, was 76.7 and 36.6%, respectively. Univariate analysis showed that Cancer of the Liver Italian Program (CLIP) score, tumor growth pattern, α-fetoprotein level, and complete tumor necrosis, were factors significantly related to poor survival. Multivariate analysis identified that factors related to poor survival were α-fetoprotein level >100 ng/ml, Child-Pugh class B, and incomplete tumor necrosis with a hazard ratio of 4.0, 2.7, and 3.8, respectively. After complete ablation, median survival was 38 months in patients with Child-Pugh class A cirrhosis and α-fetoprotein level ≤100 ng/ml, 22 months for patient with Child-Pugh class B cirrhosis and α-fetoprotein ≤100 ng/ml, and 9 months for patient with Child-Pugh class A cirrhosis and α-fetoprotein >100 ng/ml (P < 0.01).
Conclusions
Complete necrosis and absence of residual tumor positively affect survival after RFA. In patients with Child-Pugh A cirrhosis and α-fetoprotein level ≤100 radio frequency, ablation have results, 55% after 3 years, that are comparable to those of surgical resection. Patients with Child-Pugh B cirrhosis and/or α-fetoprotein >100 ng/ml showed less satisfactory results, and in these patients, multimodality treatment or other treatments should be considered.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common tumor in the world, with an estimated incidence of 500,000–1,000,000 new cases every year, and its incidence is still rising in Western Countries.1–3
HCC arise on cirrhosis in more than 80% of patients with a natural history that is extremely variable because is it strongly related to the severity of underling liver disease.4 Liver transplantation and liver resection offer the best results in terms of survival, but only 20–30 % of patients can be submitted to these treatments.5–7 Liver transplantation treats both cirrhosis and HCC, but it can be applied only in a small portion of patients because of organ shortage.
Liver resection in cirrhotic patients has good results for patients with Child-Pugh class A cirrhosis without portal hypertension and normal bilirubin level, but results are not satisfactory in patients with more severe cirrhosis. Moreover, recurrence rate after liver resection is high with an incidence greater than 70% after 5 years.8
During the last years, local ablation techniques (ethanol injection, microwave ablation, and radio frequency ablation) gained consent because of good results in local necrosis and low complication rates.
Many studies in literature reported efficacy of radio frequency ablation (RFA), but data about survival are limited to a small series with a short follow-up. Moreover, a few studies in literature analyze prognostic factor for survival after RFA in HCC.9–11
The aim of this study was to analyze prognostic factors for survival after RFA of HCC on cirrhosis and to identify different prognostic classes of patients.
Materials and Methods
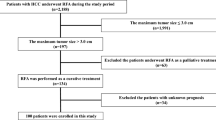
Between January 1998 and May 2004, 98 cirrhotic patients with 145 HCC were treated with percutaneous RFA at the 1st Department of General Surgery of University of Verona. Among these, 79 were male and 19 were female. Mean age of patients was 67 years (range 41–88). Patient characteristics are summarized in Table 1. Patients were classified according to Child-Pugh classification and CLIP (Cancer of The Liver Italian Program) score.12 , 13
Diagnosis of HCC were based on accordance of two imaging techniques [computed tomography (CT) and magnetic resonance imaging (MRI)] showing an arterial hypervascularization in a focal lesion ≥2 cm or with a combined criteria of an imaging technique and serum α-fetoprotein level greater than 400 ng/ml, according to The European Association for Study of the Liver (EASL) consensus conference criteria.14 In 25 patients with uncertain radiological findings, diagnosis was confirmed with fine needle biopsy. Exclusion criteria from the study were: Child-Pugh class C cirrhosis, severe ascites, tumor larger than 6 cm, more than four tumor nodules and extrahepatic disease.
All patients were submitted to RFA with percutaneous approach under real-time ultrasound guidance in the operating room with general anesthesia or conscious sedation. The expandable electrode was inserted into the tumor with ultrasonography guidance and prongs were deployed. During the study period, two different types of needle and RF generator were employed. From 1998 to June 2000, we utilized 15-gauge electrodes with four hooks connected to an RF generator with 50-W output (model 500, RITA Medical System, Mountain View, CA). From June 2000, a new expandable electrode (with seven to nine hooks) and a new RF generator with 150-W output was introduced (model 1500, RITA Medical System, Mountain View, CA). Real time monitoring of temperature of hooks was set to maintain mean temperature of 100°C for 12–20 min. For lesions larger than 5 cm, multiple overlapping ablations were applied.
After treatment, blood count and liver function tests were performed after 12 and 24 h. Patients were monitored in the hospital overnight and discharged the next day unless there was presence of complications. Evaluation of tumor response after RFA was based on World Health Organization (WHO) criteria in which complete tumor response is defined as the absence of arterial enhancement within or at the periphery of all treated tumors determined by two observations (CT or MRI) not less than 4 weeks apart.15
In our institution, we routinely perform dual phase contrast-enhanced CT scan. We utilize dynamic gadolinium enhanced MRI in patients with contraindications to CT (i.e., chronic renal failure, history of adverse reactions to iodine contrast agents). Patients with incomplete tumor response were evaluated for a new RFA treatment.
Local recurrence was defined as evidence of pathologic enhancement within or at the periphery of a tumor with previous complete response.
Distant intrahepatic recurrence was defined as appearance of new liver tumors in the liver distant from the ablated tumor.
Follow-up protocol consists of monitoring serum α-fetoprotein level every 3 months and evaluation of imaging, contrast CT, or MRI after 3 months, and every 6 months thereafter. Local recurrences or distant intrahepatic recurrences were reevaluated for new treatment in all patients with ethanol injection, RFA, or chemoembolization according to number and size of recurrence.
Statistical Analysis
Data were collected and analyzed by Stata version 8.2 (StataCorp, College Station, Texas).16 Comparison between categorical variables was carried out with Pearson chi-square test. For univariate survival analysis, Cox regression model was utilized with log-rank test evaluation of statistical significance. The univariate survival analysis was reported for each of the observed variables and uncorrected (crude) hazard ratios together with 95% confidence interval and P value of the log-rank tests.
For univariate analysis, the following variables were analyzed: gender, age, type of cirrhosis, CLIP score, Child-Pugh class, tumor size, number of tumors, tumor location, type of growth of tumor, α-fetoprotein level, complete ablation of tumor after treatment.
For multivariate analysis, the bootstrap variable selection method proposed by Austin and Tu was utilized to identify predictive variables. Cox models were estimated on a set of 5,000 bootstrap samples after stepwise (forward and backward) selection, and the candidate variables were ranked according to the proportion of bootstrap samples in which they were identified as independent predictors.17 Starting from the most frequently selected variables and sequentially adding variables until the predictive accuracy do not significantly increase, the final proportional hazard Cox models were estimated. The goodness-of-fit of the models was tested by the method proposed in May and Hosmer using 6, 8, and 10 quantiles of risk.18 Moreover, after model estimation, the analysis of deviance and efficient score residuals were performed, and the proportional hazard assumption was tested based on Schoenfeld residuals.
Results
During the study period, 98 patients with 145 tumors were treated with RFA. Median follow up for surviving patients was 22 months (range 3–76). A single tumor was present in 60 patients and multiple tumors in 38 patients; mean tumor number was 1.5 (range 1–3). Mean tumor size was 3.8 cm (range 1.5–6). In 14 patients, minor complications occurred, and major complications occurred in 8 patients. No treatment-related deaths were observed. Detailed description of complications are reported in Table 2.
Complete tumor response was achieved after the first treatment in 47 (88.6%) lesions smaller than 3 cm, in 54 (71%) lesion larger than 3 cm and smaller than 5 cm, and in 6 (37.5%) lesions larger than 5 cm (P < 0.001).
RFA treatment was repeated in 38 lesions with incomplete tumor response. After single or multiple RFA treatment, complete response was achieved in 98.1% (52 lesions) for HCCs smaller than 3 cm, in 81.5% (62 lesions) for HCCs larger than 3 cm and smaller than 5 cm, and in 62.5% (10 lesions) for lesions larger than 5 cm (P < 0.001).
We analyzed the following tumor-related variables to identify factors related to complete response: size, number, type of growth, subcapsular location, location near major vessels, and α-fetoprotein level. We identify that complete tumor response was higher in patients with tumor smaller or equal to 3 cm (98.1% versus 78.7%, P = 0.005), distant from major vessel (90.2% versus 73.3%, P = 0.02), and with α-fetoprotein level lower or equal to 100 ng/dl (89.2% versus 58.8%, P = 0.002). No patients with HCC smaller than 3 cm and α-fetoprotein level lower than 100 ng/dl had incomplete tumor response.
During follow-up, local recurrences were observed in 31 lesions (21.3%), whereas distant recurrences were detected in 36 patients (36.7%). During follow-up, 57 patients died. At the time of death, cause of death was related to tumor in 39 patients, whereas in 18 patients, no viable tumor was present and death was related to complications of cirrhosis (liver failure in 10, variceal bleeding in 7 and hepato-renal syndrome in 1).
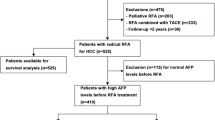
With univariate analysis, we identified that CLIP score, tumor growth type, α-fetoprotein level, and complete response after treatment were significantly related to survival (Table 3). We identified that the best cutoff level for α-fetoprotein level in our sample is 100 ng/dl. We estimated a Cox multiple regression model with the following explanatory variables: gender, age, tumor ablation, Child-Pugh class, and α-fetoprotein. Age was added to the model after standardization (mean 67.2, SD 8.7).
Table 4 shows the hazard ratio estimates (HRs) of the model, together with their 95% confidence interval and the P values of the corresponding HR = 1 hypothesis tests. The goodness-of-fit of the model was successfully tested within quantile z-scores, and P values showed that the estimated expected numbers of failures were not significantly different from the observed numbers of failures. Finally, the proportional hazard (PH) assumption was globally tested and cannot be rejected (χ 2 = 10.3, P value = 0.115).
Another multivariate model was estimated with the following explanatory variables: gender, age, CLIP score, and α-fetoprotein. A complete description of the model is reported in Table 4. The goodness-of-fit of the model was successfully tested. Finally, the proportional hazard (PH) assumption was globally tested and should be rejected (P value = 0.029).
Overall median survival after RFA was 26 months; 1- and 3-years survival was 76.7 and 36.6%, respectively. Survival for patients with Child-Pugh class A cirrhosis was 81.8 and 45.2% after 1 and 3 years, respectively, whereas it was 70.5 and 27% for patients with Child Pugh class B cirrhosis (P = 0.09), respectively. We did not observe differences in cause of death between patients with Child-Pugh class A and B; deaths were tumor related in 70.4% and in 62.1%, respectively (P = 0.5). Patients with complete tumor response after treatment had a significantly longer survival in comparison to patients with incomplete tumor necrosis: median survival of 27 months (95% CI 23–30) and 8 months (95% CI 5–11), respectively (P < 0.01) (Fig. 1).

Survival curves according to complete or partial necrosis after RFA treatment (P < 0.01).
After complete response of the tumor, median survival for patients with Child-Pugh class A cirrhosis and α-fetoprotein ≤100 ng/ml was 38 months (95% CI 23–53), 22 months (95% CI 12–31) for patients with Child-Pugh class B cirrhosis and α-fetoprotein ≤100 ng/ml, and 9 months (95% CI 7–11) for patients with Child-Pugh class A cirrhosis and α-fetoprotein >100 ng/ml (p < 0.01, Fig. 2). Survival for patients with Child-Pugh class B cirrhosis and α-fetoprotein >100 ng/ml was not analyzed because of small sample size.

Survival curves after complete necrosis of tumor according to Child-Pugh class and α-fetoprotein level (P < 0.01).
After complete ablation of the tumor, median survival for patients with Clip score equal to 0 and α-fetoprotein ≤100 ng/ml was 38 months (95% CI: 24–51), 26 months (95% CI: 20–32) for patients Clip score greater than 0 and α-fetoprotein ≤100 ng/ml and 9 months (95% CI 3–15) for patients Clip score greater than 0 and α-fetoprotein >100 ng/ml (P < 0.01). Survival for patients with Clip score equal to 0 and α-fetoprotein >100 ng/ml was not analyzed because no patient belonged to this group.
Discussion
RFA was recently introduced in clinical practice and is widely used in Europe and East countries to treat primary liver tumors with greater efficacy than ethanol injection in terms of tumor necrosis and number of sessions for complete response.19 , 20 Studies on ablation efficacy showed that complete necrosis of the tumor can be achieved in more than 90% of HCCs smaller than 3 cm, in 60–93% for lesions between 3 and 5 cm, and in 24–93% for lesion between 5 and 8 cm.21–23
Data about survival after RFA of HCCs are limited to small series and short follow-up. However, survival for small HCCs are good and are comparable to those of surgical resection with a 3-year survival of 45–68%.21 , 24 Few studies in literature analyze prognostic factors for survival after RFA, and they identify that factors related to survival are tumor size, α-fetoprotein level, complete tumor response after RFA, and albumin level.9 , 10 Our study confirms data of literature, and we identified that factors related to survival were: Child-Pugh class, α-fetoprotein level, and complete tumor response after RFA.
We confirm, in multivariate analysis, the importance of severity of liver disease for survival of patients after treatment. Child-Pugh class B patients have a relative risk equal to 2.7 in comparison to Child-Pugh A patients. Survival after 1 and 3 years for Child-Pugh class A patients was 81.8 and 45.2%, respectively, whereas survival for Child-Pugh class B patients was 70.5 and 27% (P = 0.09), respectively.
Our study confirms data of literature about the importance of complete response of the tumor.9 , 25 Patients with incomplete tumor necrosis after single or multiple treatment have hazard risk for death of 3.8 (95% CI 1.5–9.7). Moreover, our study shows that complete response can be achieved with both single or multiple treatment without differences in terms of survival, with a relative risk of 0.7 (95% CI 0.3–1.3).
In our results, high α-fetoprotein level was the strongest prognostic factor for survival with a hazard ratio for death of 4.0 (95% CI 1.6–9.8). As reported in previous studies, α-fetoprotein reflect the biological behavior of a tumor, and higher levels of this marker are related to size, to number of neoplastic nodules, and to poor prognosis.26
Utilizing the multivariate model, we identify a group of patients with best prognosis (Child-Pugh class A cirrhosis and with α-fetoprotein level ≤100 ng/ml and complete response after RFA) that has a median survival of 38 months with a 3-year survival rate of 55% and that are comparable with surgical series.27 The other group of patients (incomplete necrosis to treatment and α-fetoprotein level greater than 100 ng/ml) has worse prognosis with a median survival of 6 months (95% CI 6–7 months) and with no survivors after 3 years.
Staging system of HCC have a great importance in prognostic evaluation after surgical and nonsurgical interventions. Many staging systems were proposed, but complex relationship between cirrhosis, stage of tumor, and different types of treatment does not allow accurate stratification of different prognostic classes. Among different staging systems, results of those that consider only the severity of liver damage (Child-Pugh) or only the extension of tumor [International Union Against Cancer (UICC) TNM staging] does not allow a precise classification of risk.28 More recently, other staging systems that combine evaluation of cirrhosis and extension of tumor were introduced [CLIP, Chinese University Prognostic Index (CUPI), Barcelona Clinic Liver Cancer (BCLC)].28 The CLIP score, developed from a group of patients submitted to various types of treatment, showed good performances in surgical and nonsurgical patients in validation studies.29–31
With multivariate analysis, we identify that a combination of CLIP score and α-fetoprotein threshold level of 100 ng/ml have greater goodness-of-fit in comparison to CLIP score. This should be associated to α-fetoprotein threshold level (400 ng/ml) included in CLIP score that is observed in a few patients in our series (only 12 patients). In our opinion, a threshold level of 100 ng/ml better describe our study population.
This study confirms good results of RFA in a selected group of patients. Complete necrosis of the tumor after treatment have great value and is one of the most important prognostic factor. The best results were observed in patients with Child-Pugh class A cirrhosis and a low level of α-fetoprotein. In patients with Child B or with AFP level greater than 100 ng/ml, RFA treatment showed less satisfactory results, and in these patients, multimodality treatment or other treatments should be considered.
Abbreviations
- (HCC):
-
Hepatocellular carcinoma
- (RFA):
-
Radio frequency ablation
- (WHO):
-
World Health Organization
- (HRs):
-
Hazard ratio estimates
- (PH):
-
Proportional hazard
- (UICC):
-
International Union Against Cancer
References
Bosch, F. X., Ribes, J., & Borras, J. (1999). Epidemiology of primary liver cancer. Seminars in Liver Disease, 19, 271–285.
Bosch, F. X., Ribes, J., Diaz, M., & Cleries, R. (2004). Primary liver cancer: Worldwide incidence and trends. Gastroenterology, 127(5 Suppl 1), S5–S16, Nov.
Yanaga, K. (2004). Current status of hepatic resection for hepatocellular carcinoma. Journal of Gastroenterology, 39(10), 919–926, Oct.
Carr, B. I. (2004). Hepatocellular carcinoma: Current management and future trends. Gastroenterology, 127(5 Suppl 1), S218–S224, Nov.
Fong, Y., Sun, R. L., Jarnagin, W., & Blumgart, L. H. (1999). An analysis of 412 cases of hepatocellular carcinoma at a Western center. Annals of Surgery, 229, 790–799.
Llovet, J. M., Fuster, J., & Bruix, J. (1999). Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: Resection versus transplantation. Hepatology, 30, 1434–1440.
Poon, R. T., Fan, S. T., Lo, C. M., Ng, I. O., Liu, C. L., Lam, C. M., et al. (2001). Improving survival results after resection of hepatocellular carcinoma: A prospective study of 377 patients over 10 years. Annals of Surgery, 234, 63–70.
Bruix, J., & Llovet, J. M. (2002). Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology, 35(3), 519–524, Mar.
Camma, C., Di Marco, V., Orlando, A., Sandonato L., Casaril A., Parisi P., et al. (2005). Treatment of hepatocellular carcinoma in compensated cirrhosis with radio-frequency thermal ablation (RFTA): A prospective study. Journal of Hepatology, 42(4), 535–540, Apr.
Montorsi, M., Santambrogio, R., Bianchi, P., Donadon, M., Moroni, E., Spinelli, A., et al. (2005). Survival and recurrences after hepatic resection or radiofrequency for hepatocellular carcinoma in cirrhotic patients: A multivariate analysis. Journal of Gastrointestinal Surgery, 9(1), 62–67, Jan.
Vivarelli, M., Guglielmi, A., Ruzzenente, A., Cucchetti, A., Bellusci, R., Cordiano, C., et al. (2004). Surgical resection versus percutaneous radiofrequency ablation in the treatment of hepatocellular carcinoma on cirrhotic liver. Annals of Surgery, 240(1), 102–107, Jul.
Pugh, R. N. H., Murray-Lyon, I. M., & Dawson, J. L. (1973). Transection of oesophagus for bleeding oesophageal varices. British Journal of Surgery, 60, 646–664.
The Cancer of the Liver Italian Program (CLIP) Investigators. (1998). A new prognostic system for hepatocellular carcinoma: A retrospective study of 435 patients. Hepatology, 28, 751–755.
Bruix, J., Sherman, M., Llovet, J. M., Beaugrand, M., Lencioni, R., Burroughs, A. K., et al. (2001). EASL Panel of Experts on HCC. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. Journal of Hepatology, 35 (3), 421–430, Sep.
Miller, A. B., Hoogstraten, B., Staquet, M., & Winkler, A. (1981). Reporting results of cancer treatment. Cancer, 47, 207–214.
Rabe-Hesketh, S., & Everitt, B. S. A. (2003). Handbook of Statistical Analyses Using Stata (3rd ed.). Boca Raton, FL: Chapman & Hall/CRC.
Austin, P. C., & Tu, J. V. (2004). Bootstrap methods for developing predictive models. The American Statistician, 58(2), 131–137.
May, S., & Hosmer, D. W. (1998). A simplified method of calculating an overall goodness-of-fit test for the Cox proportional hazards model. Lifetime Data Analysis, 4, 109–120.
Lencioni, R. A., Allgaier, H. P., Cioni, D., Olschewski, M., Deibert, P., Crocetti L., et al. (2003). Small hepatocellular carcinoma in cirrhosis: Randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology, 228, 235–240.
Livraghi, T., Goldberg, S. N., Lazzaroni, S., Meloni, F., Solbiati, L., & Gazelle, G. S. (1999). Small hepatocellular carcinoma: Treatment with radiofrequency ablation versus ethanol injection. Radiology, 210, 655–661.
Guglielmi, A., Ruzzenente, A., Battocchia, A., Tonon, A., Fracastoro, G., & Cordiano, C. (2003). Radiofrequency ablation of hepatocellular carcinoma in cirrhotic patients. Hepatogastroenterology, 50, 480–484.
Livraghi, T., Goldberg, S. N., Lazzaroni, S., Meloni F., Ierace T., Solbiati L., et al. (2000). Hepatocellular carcinoma: Radio-frequency ablation of medium and large lesions. Radiology, 214(3), 761–768, Mar.
Poon, R. T., Ng, K. K., Lam, C. M., Ai, V., Yuen, J., & Fan, S. T. (2004). Effectiveness of radiofrequency ablation for hepatocellular carcinomas larger than 3 cm in diameter. Archives of Surgery, 139(3), 281–287, Mar.
Rossi, S., Di Stasi, M., Buscarini, E., Quaretti P., Garbagnati F., Squassante L., et al. (1996). Percutaneous RF interstitial thermal ablation in the treatment of hepatic cancer. American Journal of Roentgenology, 167, 759–768.
Sala, M., Llovet, J. M., Vilana, R., Bianchi L., Sole M., Ayuso C., et al. (2004). Initial response to percutaneous ablation predicts survival in patients with hepatocellular carcinoma. Hepatology, 40(6), 1352–1360, Dec.
Tangkijvanich, P., Anukulkarnkusol, N., Suwangool, P., Lertmaharit S., Hanvivatvong O., Kullavanijaya P., et al. (2000). Clinical characteristics and prognosis of hepatocellular carcinoma: Analysis based on serum alpha-fetoprotein levels. Journal of Gastrointestinal Surgery, 31, 302–308.
Wayne, J. D., Lauwers, G. Y., Ikai, I., Doherty, D. A., Belghiti, J., Yamaoka Y., et al. (2002). Preoperative predictors of survival after resection of small hepatocellular carcinomas. Annals of Surgery, 235(5), 722–730, May.
Wildi, S., Pestalozzi, B. C., McCormack, L., & Clavien, P. A. (2004). Critical evaluation of the different staging systems for hepatocellular carcinoma. British Journal of Surgery, 91(4), 400–408, Apr.
The Cancer of the Liver Italian Program (CLIP) Investigators. (2000). Prospective validation of the CLIP score: A new prognostic system for patients with cirrhosis and hepatocellular carcinoma. Hepatology, 31, 840–845.
Ueno, S., Tanabe, G., Sako, K., Hiwaki T., Hokotate H., Fukukura Y., et al. (2001). Discrimination value of the new western prognostic system (CLIP score) for hepatocellular carcinoma in 662 Japanese patients. Cancer of the Liver Italian Program. Hepatology, 34, 529–534.
Zhao, W. H., Ma, Z. M., Zhou, X. R., Feng, Y. Z., & Fang, B. S. (2002). Prediction of recurrence and prognosis in patients with hepatocellular carcinoma after resection by use of CLIP score. World Journal of Gastroenterology, 8, 237–242.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guglielmi, A., Ruzzenente, A., Sandri, M. et al. Radio Frequency Ablation for Hepatocellular Carcinoma in Cirrhotic Patients: Prognostic Factors for Survival. J Gastrointest Surg 11, 143–149 (2007). https://doi.org/10.1007/s11605-006-0082-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-006-0082-y