
Abstract
Patients with multiple endocrine neoplasia type-1 syndromes are known to have neuroendocrine tumors (NETs) involving the pituitary and gastroenteropancreatic region, in addition to the presence of parathyroid abnormalities. In rare instances adenomas in the ectopic pituitary gland have been reported. As pituitary gland and pituitary adenomas are known to express SSTRs, somatostatin receptor scintigraphy can be used for imaging. Somatostatin receptor-based PET/CT imaging using 68Ga-DOTANOC has become a popular noninvasive imaging modality for evaluation of patients with NETs. The application of 68Ga-DOTANOC PET/CT can be extended to multiple endocrine neoplasia type 1 patients, as is evident from this case study.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Patients with neuroendocrine tumors (NETs) of the gastroenteropancreatic tract are known to have associated neoplasms involving other organs. The inherited syndrome of multiple endocrine neoplasia type-1 (MEN1) encompasses one such entity with which patients present with multiple endocrine tumors of the gastroenteropancreatic tract (GEP) tract, multiple pituitary tumors, and parathyroid gland abnormalities [1]. Clinically they present either with symptoms arising from multiple gland effects, or involvement of any one organ may predominate with other manifestations being silent. Pituitary adenomas are seen in most patients with MEN-1 Syndrome. Ectopic pituitary adenoma (EPA) is a rare entity. Furthermore, EPA with an empty sella is extremely rare. Here we report a case that presented with NET involving the duodenum and was diagnosed to have occult pituitary tumor (macroadenoma) of an ectopic gland with empty sella on 68Ga-labeled (1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid)-1-NaI3-octreotide (68Ga-DOTANOC) positron emission tomography–computed tomography (PET/CT) study.
Case report
A 71 year old female presented with painless progressive obstructive jaundice of over 3 months duration. A preliminary ultrasound examination of the abdomen revealed a mass lesion arising from a small bowel loop. A contrast enhanced computed tomography (CECT) examination of the abdomen was performed and revealed the presence of a heterogeneous mass lesion arising from the duodenum. No other abdominal abnormalities were noted. A tissue biopsy from the duodenal tumor revealed features of a well differentiated neuroendocrine tumor. To rule out presence of metastatic disease, the patient was referred for somatostatin receptor scintigraphy (SRS) with 68Ga-DOTANOC PET/CT (Fig. 1). It showed intense tracer uptake in the primary duodenal tumor compatible with neuroendocrine histology (Fig. 2). No other obvious metastatic regions were discovered. However, abnormal uptake was noticed in a mass lesion arising in the region of sphenoid sinuses with no tracer uptake in the sella turcica corresponding to the pituitary gland (Fig. 3). To further characterize this lesion, magnetic resonance (MR) imaging was performed, which revealed presence of an empty sella with an ectopic pituitary gland presenting as mass lesion in the sphenoid sinuses (Fig. 4). Interestingly no clinical signs and symptoms suggestive of parathyroid abnormalities were present in this patient, but biochemical investigations did reveal the presence of mild asymptomatic hypercalcemia and elevated serum parathyroid hormone (PTH) levels.

71 year old female patient presented with features of obstructive jaundice and was diagnosed with duodenal neuroendocrine tumor. She was referred for staging 68Ga-DOTANOC PET/CT. Whole body maximum intensity projection (MIP) image shows the presence of abnormal radiotracer uptake in the abdomen (bold arrow). Increased radiotracer uptake is also seen in the region of the base of the skull (arrow). In contrast with normally seen mild uptake in the pituitary gland, this focus was large and very intense (SUVmax-32) and hence considered abnormal

Transaxial PET/CT images of the primary duodenal tumor. Nonenhanced CT image shows a large heterogeneously enhancing mass involving predominantly the second part of duodenum (a bold arrow). The mass caused near complete occlusion of the ampullary opening, as is evident from the presence of dilated intrahepatic biliary duct radicles (a arrow). Intense tracer uptake was seen in the mass on 68Ga-DOTANOC PET and PET/CT images (b, c SUVmax-28) suggestive of a somatostatin receptor-expressing neoplasm. No other area of abnormal tracer activity was seen within the abdomen

PET/CT images of the skull. Transaxial unenhanced CT image shows a soft tissue density mass involving the sphenoid sinuses (a bold arrow). Increased tracer uptake is noted on the axial PET image (b). PET/CT section reveals intense tracer uptake in the soft tissue mass with no erosion of adjacent bony structures (c). Cranial PET/CT section through the pituitary fossa was also inspected and no definite evidence of tracer uptake was seen in the pituitary fossa (not shown)

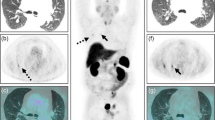
MR imaging was carried out to characterize the mass discovered on 68Ga-DOTANOC PET/CT imaging. Axial T1 weighted MR image through the region of sphenoid sinuses shows a relatively isointense soft tissue mass in the region of the sphenoid sinus (a bold arrow). Sagittal T1-weighted image reveals a large infrasellar soft tissue mass involving the sphenoid sinuses (b arrow), with the features of an empty sella. Pituitary stalk was central. Axial T2 weighted axial image shows the hyperintense mass (c arrow). CSF density is noted occupying the sellar region confirming the presence of an empty sella (d asterisk). Contrast enhanced axial (e) and sagittal (f) T1-weighted images are shown and reveal avid enhancement of the mass (arrow) described above
Discussion
Ectopic pituitary adenomas are rare lesions, and a high index of suspicion for EPA and familiarity with the imaging findings may help to diagnose this rare entity accurately [2]. Also uncommon is the association of such EPA with an empty sella [2]. Sphenoid sinus or infrasellar location has been shown to be the most common site for such EPA. Presence of a sphenoidal EPA has been hypothesized to be either purely ectopic in origin or arising from an invasive primary pituitary adenoma. Embryonic cells that give origin to the pituitary gland reside in the nasopharyngeal region and may develop hormonal stimulation leading to hypertrophy, leaving very few cells to constitute the normal pituitary gland, resulting in an empty sella. This gives rise to an ectopic pituitary adenoma in its true sense. Two plausible mechanisms have been hypothesized to explain an ectopic adenoma arising from invasive primary pituitary lesions. The first emphasizes the fact that an empty sella existed primarily, with subsequent development of a pituitary adenoma and herniation through the sellar floor. In the other scenario the macroadenoma first arose in the sella turcica and then migrated to the sphenoid sinus; in the course of tumor growth, the intrasellar component underwent necrosis giving rise to a secondary empty sella. This sporadic association of an adenoma arising in an ectopic pituitary gland has been described in the literature [2, 3]; their occurrence in the setting of a MEN1 syndrome has, however, not been described previously. A similar association of an empty sella has been found in association with MEN1 syndrome but no adenoma was present [4].
The differentials of skull base tumors that arise from such locations are primary malignant tumors of the sphenoidal sinus viz. squamous cell carcinoma, adenoid cystic carcinoma, and chondrosarcoma [5]. The avid enhancement on post contrast MRI images with high of tracer avidity to 68Ga-DOTANOC precludes the possibility of primary malignant tumors of the sphenoidal sinus. A high degree of tracer avidity to 68Ga-DOTANOC is also observed for meningiomas but the possibility of meningioma was excluded as the mass showed T2 hyperintensity on MRI along with the absence of adjacent dural enhancing tail. In view of MRI characterization of the subsellar mass a diagnosis of EPA was considered before meningioma.
In our case, no evidence of clinical features that would suggest the presence of a pituitary lesion or biochemical evidence of hormonal excess was found, which is common with pituitary adenomas, especially those associated with MEN1 syndrome [6]. Our patient presented with obstructive jaundice and was found to have a foregut neuroendocrine tumor involving the duodenum. In addition the patient had no signs or symptoms of hyperparathyroidism, which is very common in MEN1 syndrome patients [7], although she had asymptomatic mild elevations of serum PTH levels. Concurrent presence of an abdominal neuroendocrine tumor, pituitary macroadenoma, and subclinical hyperparathyroidism suggested a diagnosis of MEN1 syndrome in this patient.
68Ga-DOTANOC PET/CT is increasingly being used for SRS of NETs [8]. It has the advantages of better resolution and ability to quantify, as compared with single photon emission tomography (SPECT) [9]. Pituitary gland expresses somatostatin receptors and is visualized on 68Ga-DOTANOC PET/CT. Somatostatin receptors expression in pituitary adenomas is reported to be highly variable within and between tumor subtypes [10]. Somatostatin receptors have been demonstrated in vitro in most cases of growth hormone (GH)-secreting adenomas and in some cases of thyroid stimulating hormone (TSH)-secreting adenomas and prolactinomas. Controversial results have been reported in other types of pituitary adenoma, for example non-secreting adenomas [10]. Utility of SRS with 111In-octreotide has been demonstrated for imaging primary and recurrent pituitary adenomas [10]. However, no study is available demonstrating the utility of 68Ga-DOTANOC PET/CT for such tumors. In this case the EPA showed increased 68Ga-DOTANOC uptake which was confirmed on MRI.
This case is thus an unusual combination of an empty sella with EPA demonstrated with 68Ga-DOTANOC PET/CT and MRI, and a clinical scenario consistent with MEN 1 syndrome. Such combination has not been described previously to the best of our knowledge. This case also highlights the importance of 68Ga-DOTANOC PET/CT for staging of patients with syndromic NETs.
References
Gibril F, Schumann M, Pace A, Jensen RT. Multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome: a prospective study of 107 cases and comparison with 1009 cases from the literature. Medicine (Baltimore). 2004;83:43–83.
Yang BT, Chong VF, Wang ZC, Xian JF, Chen QH. Sphenoid sinus ectopic pituitary adenomas: CT and MRI findings. Br J Radiol. 2010;83:218–24.
Kusano Y, Horiuchi T, Oya F, Miyaoka Y, Oguchi K, Takemae T, et al. Ectopic pituitary adenoma associated with an empty sella: a case report and review of the literature. J Neuroimaging. 2011;XX:1–2. doi:10.1111/j.1552-6569.2011.00620.
Muhr C, Ljunhhall S, Akerstrom G, Palmer M, Bergstrom K, Enoksson P, et al. Screening for multiple endocrine neoplasia syndrome (type 1) in patients with primary hyperparathyroidism. Clin Endocrinol. 1984;20:153–62.
DeMonte F, Ginsberg LE, Clayman GL. Primary malignant tumors of the sphenoidal sinus. Neurosurgery. 2000;46:1084–91.
O’Brien T, O’Riordan DS, Gharib H, Scheithauer BW, Ebersold MJ, van Heerden JA. Results of treatment of pituitary disease in multiple endocrine neoplasia, type 1. Neurosurgery. 1996;39:273–9.
Garber JE, Kenneth O. Hereditary cancer predisposition syndromes. Clin Oncol. 2005;23:276–92.
Ambrosini V, Campana D, Bodei L, Nanni C, Castellucci P, Allegri V, et al. 68Ga-DOTANOC PET/CT clinical impact in patients with neuroendocrine tumours. J Nucl Med. 2010;51:669–73.
Arman R, Habib Z. PET versus SPECT: strengths, limitations and challenges. Nucl Med Commun. 2008;29:193–220.
Hofland LJ, Lamberts SW. Somatostatin receptors in pituitary function, diagnosis and therapy. Front Horm Res. 2004;32:235–52.
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Naswa, N., Das, C.J., Sharma, P. et al. Ectopic pituitary adenoma with empty sella in the setting of MEN-1 syndrome: detection with 68Ga-DOTANOC PET/CT. Jpn J Radiol 30, 783–786 (2012). https://doi.org/10.1007/s11604-012-0117-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-012-0117-0