
Abstract
A retrospective chart review for the period between 1998 and 2006 was conducted to evaluate microneurolysis combined with a hypothenar fat pad flap (HTFPF) for patients at Mayo Clinic, Scottsdale, Arizona, who were being treated for recurrent carpal tunnel syndrome. After exclusion of patients with incomplete release of the transverse carpal ligament at the time of the original operation, 28 consecutive patients were identified. Their average age was 68.5 years (range 43–89 years). The average interval between the original carpal tunnel release and reexploration was 82 months (range 5–298 months). The average follow-up was 10.5 months (range 3–48.4 months). The preoperative two-point discrimination tests averaged 7 mm (range 5–12 mm). At surgery, all patients were found to have fibrosis surrounding the median nerve with adherence of the nerve to the radial leaf of the transverse carpal ligament. After surgery, the Tinel sign disappeared in 26 of 28 patients and two-point discrimination improved to an average of 6 mm (range 4–8 mm). Postoperative grip strength averaged 20 kg, compared with 11 kg preoperatively. Pain completely disappeared in 83% of patients (average improvement 93%, range 5–100%). Numbness completely disappeared in 42% of patients (average improvement 82.9%, range 5–100%). Tingling disappeared in 50% of patients (average improvement 84.7%, range 5–100%). No patient reported being worse after reoperation. These results suggest that the combination of microneurolysis and HTFPF can restore median nerve gliding and provide soft-tissue coverage, improving symptoms in patients with recurrent carpal tunnel syndrome.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The incidence of failure in the operative management of carpal tunnel syndrome (CTS) varies from 3% to 19% [1, 3, 10, 11, 13, 19]. Outcomes after reoperation are considerably worse, with reports of as many as 95% of patients with enduring symptoms [24] and 40% with poor results [17]. The most commonly cited causes for initial failure include incomplete release of the transverse carpal ligament, postoperative adhesions, tenosynovitis, and intraneural fascicular scarring [10, 12–14]. Previous reports have identified the most common finding at reexploration of the median nerve as incomplete release of the transverse carpal ligament [11]. Our experience is in agreement with that of Hunter [9] and Strickland et al [25], who found that recurrence is often caused by tethering of the median nerve within the carpal canal. Severe perineural fibrosis is consistently observed at reexploration; the median nerve may be pushed toward the palmar arch by the flexor tendons, or it may be trapped in fibrous scar tissue of the transverse carpal ligament itself.
Nonoperative treatment of recurrent CTS may provide symptomatic relief for a small number of patients but fail to benefit most patients in the long term. Unfortunately, revision decompression and simple neurolysis have been equally disappointing in relieving hand pain in most cases [4, 5, 11, 30]. Various soft-tissue flaps have been described to provide coverage of the nerve at reexploration to mitigate the residual compression and prevent adherence of the median nerve to the carpal canal [16, 21, 23]. The hypothenar fat pad flap (HTFPF), first described by Cramer [2], has been refined by Strickland et al. [25] to provide a barrier between the median nerve and the remaining radial leaf of the transverse carpal ligament. The fat pad serves to provide coverage of the nerve, to prevent readherence, and to restore a smooth gliding bed for the median nerve. In a series of 62 hands, Strickland et al. [25] demonstrated excellent results in relieving recalcitrant symptoms with use of the HTFPF at an average follow-up of 33 months.
Analyzing the results of many series of soft-tissue flap coverage at reexploration is difficult because of the small number of patients and the heterogeneity of the study group. Specifically, the patient population may include patients with incomplete release (as indicated by persistent symptoms after initial surgical decompression), patients with peripheral neuropathy, and patients with true recurrent CTS as defined by Wulle [32]. The purpose of our study was to evaluate the operative findings and outcomes of reexploration for patients with true recurrent CTS [32]; in other words, we studied a select population with improvement in pain, numbness, and tingling after surgical decompression and recurrence of those symptoms after a symptom-free period, usually months or years. Furthermore, we discuss our own modification of the Strickland technique for the HTFPF, which involves microneurolysis of the median nerve to the level of normal fascicular anatomy.
Materials and Methods
Twenty-eight consecutive patients with true recurrent CTS as defined by Wulle were reexplored at Mayo Clinic, Scottsdale, Arizona, between 1998 and 2006. Patients were excluded if they had incomplete release of the transverse carpal ligament or evidence of peripheral neuropathy. All operations were performed by A. S. or S. D. and consisted of microneurolysis of the median nerve combined with an HTFPF. In all cases, the patients presented with recurrent symptoms after an open (n = 27) or endoscopic (n = 1) surgical decompression. All patients failed an initial trial of nonoperative treatment before reexploration.
Median nerve hypersensitivity was present at the wrist and around the scar in all patients; none demonstrated evidence of injury to the palmar cutaneous branch. The initial surgery was performed at a different institution in all but six cases. The care of two patients was covered under worker’s compensation benefits.
Electrical studies consisting of nerve conduction and electromyogram were performed preoperatively. In all cases, the nerve conduction studies, both sensory and motor, were abnormal with prolonged latency and decreased velocity compared with the contralateral side. In more than 75% of cases, the electromyogram was also abnormal. These studies could not be compared to previous evaluations because most of them were performed elsewhere before the initial surgery.
Surgical Technique
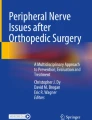
Reexploration of the median nerve with a HTFPF procedure was performed as described by Strickland et al. [25]. However, the procedure was modified to include use of an operative microscope for microneurolysis of the median nerve throughout the entire zone of scarred adhesions. The previous incision was used but extended both proximally and distally to facilitate complete exposure of the nerve proximal and distal to scar tissue. The median nerve was identified and consistently found to be adherent to the underside of the transverse carpal ligament within the carpal canal. Extensive fibrosis severely limited nerve mobility and gliding (Fig. 1A and B). Under microscope magnification, a 69-gauge Beaver blade was used to perform complete external neurolysis of the median nerve throughout the entire zone of scarring down to the level of normal fascicular architecture (Fig. 1C).

A and B, Operative findings consistently demonstrated adhesion of the nerve to the radial border and roof of the carpal tunnel. C, Under microscope magnification, a complete external microneurolysis was performed throughout the entire zone of scarring to the level of normal fascicular anatomy. (Used with permission of Mayo Foundation for Medical Education and Research).
Microneurolysis frees the nerve from any surrounding scar tissue to make it completely mobile (Fig. 2A and B). Normal nerve gliding should be established. We did not do internal neurolysis. An HTFPF procedure was performed (Fig. 3A and B), and the hand was placed in a thumb spica cast for 4 weeks.

A and B, Recurrent fibrosis prevented nerve mobility or gliding in all patients. After microneurolysis, the nerve should be mobile and free of tension during wrist range of motion.

A hypothenar fat pad flap procedure was performed by first identifying the ulnar nerve proximally and distally. A, The ulnar leaf was resected. (Used with permission of Mayo Foundation for Medical Education and Research.) B, The flap was then transferred onto the median nerve and attached with several stitches to the radial wall of the carpal canal at the level of the flexor pollicis longus tendon.
Patients were seen in follow-up visits at 2, 4, 8, and 12 weeks and at 6, 9, and 12 months and then yearly. At postoperative visits, the patients were routinely questioned about occurrence of pain, numbness, and tingling. Grip strengths were also obtained, and Tinel sign, Phalen maneuver, and Durkan compression tests were repeated.
Results
All 28 patients were available for follow-up at all scheduled visits. The average age of the 28 patients at reoperation was 68.5 years (range 43–89 years). The average interval between the original carpal tunnel release and reexploration was 82 months (range 5–298 months). Average follow-up was 10.5 months (range 3–48.4 months). Twenty-five of 28 procedures were on the right side and three were on the left side.
The preoperative two-point discrimination tests averaged 7 mm (range 5–12 mm). All patients had a positive Tinel sign preoperatively. Moreover, all patients demonstrated cutaneous hypersensitivity of the surgical scar. At reoperation, all patients were found to have fibrosis surrounding the median nerve, which was attached to the radial leaf of the transverse carpal ligament. After surgery, the Tinel sign disappeared in 26 of 28 patients and two-point discrimination improved to an average of 6 mm (range 4–8 mm).
Preoperative grip strength averaged 11 kg and postoperative grip strength averaged 20 kg. Pain disappeared completely in 83% of patients, with improvement in sensation and strength. Patients reported an average subjective improvement in pain of 93% (range 5–100%). Numbness completely disappeared in 42% of patients. Average subjective improvement in numbness was 82.9% (range 5–100%). Tingling disappeared completely in 50% of patients. Average subjective improvement in tingling was 84.7% (range 5–100%). No patient reported being worse after reoperation.
Discussion
Paine [18] first reported reexploration for true recurrent CTS in 1963. Langloh and Linscheid [11] subsequently detailed 34 cases of recurrent and unrelieved CTS, of which seven were true recurrences. The outcomes of these early studies are difficult to interpret, because patients with incomplete division of the transverse carpal ligament were included with patients who had true recurrence. Our technique of microneurolysis of the median nerve combined with a hypothenar pedicle flap for coverage in cases of recalcitrant CTS is a simple, effective technique that improves symptoms. However, the success of this procedure depends on distinguishing patients with true recurrent CTS and intracanal fibrosis from those with an incomplete initial release or tenosynovitis. In cases of incomplete release, the preoperative symptoms are often the same as before the operation without an intervening symptom-free period. Conversely, in cases of true recurrent CTS, symptoms are initially improved and then recur with an exacerbation of scar hypersensitivity and a significantly positive Tinel sign at the level of previous surgery. In all our patients, electrodiagnostic studies confirmed continued compression of the median nerve at the level of the wrist.
Hunter [9] described epineural fibrous fixations, which induced median nerve traction and resulted in traction neuropathies associated with recurrent CTS. To improve outcomes, he advocated a simple surgical mobilization of the median nerve followed by early functional nerve-gliding therapy. Louis et al. [12] reported the results of simple neurolysis, which were disappointing in six of 26 cases with true recurrence. O’Malley et al. [17] reported mixed results for 20 cases of repeat surgery for CTS; nine of these were incomplete releases, whereas 11 had true recurrence with fibrosis. Most authors now agree that coverage of the median nerve must be performed after any type of neurolysis [4, 6, 20, 21, 23, 32]. Multiple local pedicle muscle flaps for coverage of the median nerve have been described in an attempt to prevent adherence to surrounding tissue. These include flaps from the abductor digiti minimi [21], the pronator quadratus [28], the lumbrical [28], and the palmaris brevis [22]. Tham et al. [27] described a reverse radial artery facial flap for treatment of recalcitrant CTS that had a satisfactory outcome in six patients. Varitimidis et al. [29] treated 15 patients with recurrent compressive neuropathy of the median nerve at the wrist with autogenous saphenous vein wrapping and found significant pain relief and improvement in sensation at a mean follow up of 43 months. However, these previous reports were limited to short-term follow-up of small series of patients or were presented as technique papers alone.
Strickland et al. [25] reported excellent results with the HTFPF in 62 hands at an average follow-up of 33 months. Mathoulin et al. [15] used a modified HTFPF in 45 patients with recurrent symptoms of CTS and reported excellent results in 49%, good results in 45%, and average results in 4.5%; the therapy failed in only 4.5% of the 45 patients at an average follow-up of 45 months. The HTFPF has come under criticism recently for its inability to be wrapped circumferentially and its limited extent of proximal and distal coverage [8]. Goitz and Steichen [8] proposed microvascular omental transfer to provide more extensive coverage of the lysed median nerve. They reported high patient satisfaction in a series of nine extremities with an average follow-up of 6.6 years. However, most of these patients had already had local flaps that failed and required a laparotomy for flap harvest.
Other authors have argued that restoration of normal nerve excursion is more important than soft-tissue coverage in the treatment of recurrent CTS. Wilgis and Murphy [31] demonstrated that nerves have longitudinal excursion, highlighting the importance of treating adherence in peripheral nerves to effectively treat the inciting lesion. Szabo et al. [26] subsequently quantified the normal excursion of the median nerve within the carpal tunnel. Duclos and Sokolow [7] described the treatment of 13 consecutive patients with true recurrent CTS. Their technique involved extensive neurolysis without the use of a vascularized flap. At an average follow-up of 27.5 months, 75% of their patients had complete relief of symptoms. Duclos and Sokolow suggested lack of normal nerve gliding as a major factor in symptom recurrence and recommended extensive neurolysis to help restore normal excursion.
Our approach combines many of the elements described above, namely restoration of nerve excursion and prevention of readherence, for a simple, effective treatment of recurrent CTS. The median nerve is first freed from the adherent radial leaf of the transverse ligament so that it can be brought into the operative field and inspected. This allows a determination of whether there is an hourglass deformity distorting the normal fascicular anatomy. Neurolysis is then performed under an operating microscope to remove the scarred epineurium to the level of normal fascicular alignment. Use of the microscope allows precise restoration of normal anatomy both proximally and distally to the area of scarring. Finally, use of the HTFPF through the same incision avoids a secondary donor site problem while simultaneously providing coverage to prevent readherance and create a suitable gliding bed for the nerve to restore normal excursion. Care should be taken to avoid internal neurolysis to prevent further fascicular scarring, which could be detrimental to outcome.
Our study reviewed the results of reoperation in a homogenous population of consecutive cases of true recurrent CTS treated with extensive microneurolysis and an HTFPF. Results were favorable for all patients. At latest follow-up, no patient who has undergone this procedure has had a recurrence, although recovery can average 6 to 9 months. The improvement in clinical symptoms in our patients compared with those reported previously can possibly be explained by the meticulous microneurolysis of the median nerve as well as the cushion effect of the fat flap. This technique appears to offer reliable improvement for patients with true recurrent CTS, possibly providing improved nerve gliding and increased soft-tissue coverage to protect the median nerve.
Abbreviations
- CTS:
-
Carpal tunnel syndrome
- HTFPF:
-
Hypothenar fat pad flap
References
Bloem JJ, Pradjarahardja MC, Vuursteen PJ. The post-carpal tunnel syndrome: causes and prevention. Neth J Surg 1986;38:52–5.
Cramer LM. Local fat coverage for the median nerve. ASSH Correspondence Newsletter 1985;35.
Cseuz KA, Thomas JE, Lambert EH, Love JG, Lipscomb PR. Long-term results of operation for carpal tunnel syndrome. Mayo Clin Proc 1966;41:232–41.
Das SK, Brown HG. In search of complications in carpal tunnel decompression. Hand 1976;8:243–9.
De Smet L. Recurrent carpal tunnel syndrome: clinical testing indicating incomplete section of the flexor retinaculum. J Hand Surg (Br) 1993;18:189.
Dellon AL, Mackinnon SE. The pronator quadratus muscle flap. J Hand Surg (Am) 1984;9:423–7.
Duclos L, Sokolow C. Management of true recurrent carpal tunnel syndrome: is it worthwhile to bring vascularized tissue? Chir Main 1998;17:113–7.
Goitz RJ, Steichen JB. Microvascular omental transfer for the treatment of severe recurrent median neuritis of the wrist: a long-term follow-up. Plast Reconstr Surg 2005;115:163–71.
Hunter JM. Recurrent carpal tunnel syndrome, epineural fibrous fixation, and traction neuropathy. Hand Clin 1991;7:491–504.
Kulick MI, Gordillo G, Javidi T, Kilgore ES Jr, Newmayer WL, III. Long-term analysis of patients having surgical treatment for carpal tunnel syndrome. J Hand Surg (Am) 1986;11:59–66.
Langloh ND, Linscheid RL. Recurrent and unrelieved carpal-tunnel syndrome. Clin Orthop Relat Res 1972;83:41–7.
Louis DS, Greene TL, Noellert RC. Complications of carpal tunnel surgery. J Neurosurg 1985;62:352–56.
MacDonald RI, Lichtman DM, Hanlon JJ, Wilson JN. Complications of surgical release for carpal tunnel syndrome. J Hand Surg (Am) 1978;3:70–6.
Mackinnon SE. Secondary carpal tunnel surgery. Neurosurg Clin N Am 1991;2:75–91.
Mathoulin C, Bahm J, Roukoz S. Pedicled hypothenar fat flap for median nerve coverage in recalcitrant carpal tunnel syndrome. Hand Surg 2000;5:33–40.
McClinton MA. The use of dermal-fat grafts. Hand Clin 1996;12:357–64.
O’Malley MJ, Evanoff M, Terrono AL, Millender LH. Factors that determine reexploration treatment of carpal tunnel syndrome. J Hand Surg (Am) 1992;17:638–41.
Paine KW. The carpal tunnel syndrome. Can J Surg 1963;6:446–9.
Phalen GS. The carpal-tunnel syndrome: seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Jt Surg Am 1966;48:211–28.
Plancher KD, Idler RS, Lourie GM, Strickland JW. Recalcitrant carpal tunnel: the hypothenar fat pad flap. Hand Clin 1996;12:337–49.
Reisman NR, Dellon AL. The abductor digiti minimi muscle flap: a salvage technique for palmar wrist pain. Plast Reconstr Surg 1983;72:859–65.
Rose EH. The use of the palmaris brevis flap in recurrent carpal tunnel syndrome. Hand Clin 1996;12:389–95.
Rose EH, Norris MS, Kowalski TA, Lucas A, Flegler EJ. Palmaris brevis turnover flap as an adjunct to internal neurolysis of the chronically scarred median nerve in recurrent carpal tunnel syndrome. J Hand Surg (Am) 1991;16:191–201.
Strasberg SR, Novak CB, Mackinnon SE, Murray JF. Subjective and employment outcome following secondary carpal tunnel surgery. Ann Plast Surg 1994;32:485–9.
Strickland JW, Idler RS, Lourie GM, Plancher KD. The hypothenar fat pad flap for management of recalcitrant carpal tunnel syndrome. J Hand Surg (Am) 1996;21:840–8.
Szabo RM, Bay BK, Sharkey NA, Gaut C. Median nerve displacement through the carpal canal. J Hand Surg (Am) 1994;19:901–6.
Tham SK, Ireland DC, Riccio M, Morrison WA. Reverse radial artery fascial flap: a treatment for the chronically scarred median nerve in recurrent carpal tunnel syndrome. J Hand Surg (Am) 1996;21:849–54.
Urbaniak JR. Complications of treatment of carpal tunnel syndrome. In: Gelberman RH, editor. Operative nerve repair and reconstruction, Vol. 2. Philadelphia: JB Lippincott; 1991. p. 967–79.
Varitimidis SE, Riano F, Vardakas DG, Sotereanos DG. Recurrent compressive neuropathy of the median nerve at the wrist: treatment with autogenous saphenous vein wrapping. J Hand Surg (Br) 2000;25:271–5.
Wadstroem J, Nigst H. Reoperation for carpal tunnel syndrome: a retrospective analysis of forty cases. Ann Chir Main 1986;5:54–8.
Wilgis EF, Murphy R. The significance of longitudinal excursion in peripheral nerves. Hand Clin 1986;2:761–6.
Wulle C. Treatment of recurrence of the carpal tunnel syndrome. Ann Chir Main 1987;6:203–9.
Acknowledgment
Editing, proofreading, and reference verification were provided by the Section of Scientific Publications, Mayo Clinic.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Craft, R.O., Duncan, S.F.M. & Smith, A.A. Management of Recurrent Carpal Tunnel Syndrome with Microneurolysis and the Hypothenar Fat Pad Flap. HAND 2, 85–89 (2007). https://doi.org/10.1007/s11552-007-9025-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11552-007-9025-7