
Abstract
Purpose
To evaluate the radiation dose reduction during endovascular aneurysm repair (EVAR) after the reconfiguration of a Philips AlluraXper FD20 X-ray system.
Methods
Between 2013 and 2015, we implemented a low-dose protocol (Eco dose) increasing the filtration with 1 mm of Al and 0.1 of Cu on both fluoroscopy and fluorography and halving the frames per second in fluoroscopy. The switch was complemented by hybrid operating room staff education and training in radiation protection. We compared two samples of 50 patients treated before the switch (normal dose) with 50 patients treated after the switch (Eco dose). Procedures were categorized into two different grades of complexity, standard and complex, intended as fenestrated/chimney/snorkel and EVAR plus additional embolization to prevent endoleak type II. We evaluated patient demographics, Air Kerma (AK), dose area product (DAP), and procedural data (fluoroscopy time, number of fluorographies, and iodinated contrast). Staff radiation dose was measured with film badge dosimeter on C-arm.
Results
The Eco-dose protocol witnessed a DAP reduction of 53% in standard EVARs and of 57% in complex EVARs and an AK reduction of 45% in standard and 57% in complex EVAR. The image quality in 2016 was perceived acceptable, as proven by the fact that fluoroscopy time, number of fluorographies, and contrast medium volumes did not have to be increased. We achieved a reduction in staff dose of 25.6%.
Conclusions
Optimized angiographic system setting significantly reduced the radiation dose both to the patients and to the staff assuring safe EVAR procedures.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Background
The endovascular management of occlusive and aneurysmal vascular diseases has significantly risen in the last few years [1, 2], with subsequently increased exposure of patients and staff to radiation. In particular, endovascular aortic procedures expose patients and staff to significant doses of ionizing radiation, with a potential risk of radiation-induced skin damage and subsequent malignancy [3]. Virtually, all patients undergoing abdominal aortic aneurysm repair (EVAR) need a preoperative CT scan, intraoperative fluoroscopic and fluorography imaging, and lifelong surveillance imaging.
The European Directive 2013/59/EURATOM of December 5, 2013 emphasized the need for justification of medical exposure and strengthened the requirements on the information to be provided to patients, the recording and reporting of doses from medical procedures, the use of diagnostic reference levels, and the availability of dose-indicating devices [4]. As of now, radiation exposure in patients who undergo medical imaging procedures is not typically monitored, but member states must transpose the directive into national legislation by February 6, 2018.
A lower radiation dose to the patient will result in a lower radiation dose also to the staff [5], dose that can be further lowered by taking protective measures, such as various forms of X-ray shielding and lead aprons, collars, and glasses. Recent technical innovation managed to reduce the entrance dose, while maintaining the image quality, by exploiting advanced real-time image-processing algorithms and hardware changes, such as thicker copper filtration, shorter pulse duration, smaller focal spot size, and a more sensitive detector [6]. In centers where this technology is not yet available, it is essential to work on the optimization of the existing angiography system for improving patients’ safety, as well as on the education of operators about the most appropriate use of the imaging equipment [7].
Well-known strategies to reduce radiation exposure during endovascular procedures are maximizing the distance between the X-ray source and the patient, minimizing the distance from the patient to the detector [8], applying low fluoroscopy settings and an appropriate field of view [9], and using road mapping functionalities [10]. Other useful tips have been proposed in the literature: The operator should not activate the fluoroscopy unit when not viewing the monitor and should make use of the last-image-hold feature [11], redundant views should be avoided, and the operator should note the number of 5-min fluoroscopic notifications alarms [12]. In addition, all forms of magnification, either decreasing the field of view (FOV) or increasing the distance between the patient and the detector, increase the radiation dose and should thus be minimized as much as possible [13]. A good collimation decreases scatter radiation, by eliminating the more divergent rays, upgrades image quality, and reduces radiation exposure by eliminating X-rays not converging on the area of interest and thus not useful to imaging. The change of projection can spare the skin from the harmful effects of radiation, but care must be exercised to use this method intelligently because steeply angled oblique images result in more tissues to be traversed by the X-ray beam and in compensation by the automatic brightness control system, resulting in an increased radiation dose [14]. In addition, radiation dose can be reduced by increasing awareness among personnel and implementing standardized X-ray exposure protocols [6].
The impact of the more recent technical innovations in reducing the entrance dose was well demonstrated in a wide spectrum of procedures, like pacemaker and implantable cardioverter defibrillator (ICD) implantations [15], trans-catheter aortic valve implantations [16], aortoiliac endovascular procedures [6], lower extremity interventions [17], and endovascular aneurysm repair too [18]. To the best of our knowledge, however, there are no studies in the literature that used a reconfiguration of the angiographic system to reduce the radiation dose during endovascular procedures.
Aim of the study
The aim of our study was to evaluate the radiation dose reduction during EVAR after the reconfiguration of the Philips (Eindhoven, the Netherlands) AlluraXper FD20 X-ray system present in our hybrid room. The estimate was made by comparing data on a sample of patients treated before the reconfiguration (year 2012) with data on an equivalent sample of patients treated after the reconfiguration (year 2016).
The primary endpoint was confirming the patient’s dose reduction. The secondary endpoints were assessing the effect on the procedural data and evaluation of the staff radiation exposure.
Materials and methods
Procedure
Between 2013 and 2015, thanks to our medical physics staff and the cooperation of Philips’s technical support, we progressively introduced and optimized a low-dose protocol (Eco dose) on our angiographic system (AlluraXper FD20 X-ray, Philips. Eindhoven, the Netherlands) consisting mainly in an additional filtration (1 mm of Al and 0.1 mm of Cu) in fluorography.
We also implemented fluoroscopy with an additional “ultra-low dose mode,” halving the pulses per second (7.5 vs. 15 pps) while maintaining the filters previously set for the low-dose mode (4 mm Al + 0.9 mm Cu). The previous “normal” and “high” dose modalities were set, respectively, with the filters of the “low” (4 mm Al + 0.9 mm Cu) and “normal” dose (4 mm Al + 0.4 mm Cu) modalities. The details of the reconfiguration are summarized in Table 1.
The entire staff (doctors, radiographers, and nurses) were extensively trained in the use of the new protocol. Specific emphasis was placed on radiation protection awareness, from the common procedures for the reduction of the radiation dose to the safest and most proficient ways for adopting, whenever possible, the Eco mode and not going over the number of fluorographies necessary for the best outcome of EVAR.
Study design and samples
The aim of the study was to test whether the implementation of the Eco-dose protocol fostered a decrease in the dose received by the patients without unacceptable cuts in the image quality.
To this end, EVAR procedures were categorized into two different grades of complexity:
-
Standard EVARs;
-
Complex EVARs, including EVAR plus additional embolization to prevent endoleak type II and fenestrated/chimney/snorkel EVARs.
Two samples, each composed of 25 consecutive standard and 25 consecutive complex EVARs, were compared. The first sample included the last 50 procedures performed before the optimization (normal-dose sample), whereas the second one included the first 50 procedures performed after the optimization had been completed and had become the routine mode of operation (Eco-dose sample).
No exclusion criteria were applied to patients as to age, gender, and body mass index (BMI).
The patient radiation dose was obtained by evaluating the Air Kerma (AK) and the dose area product (DAP), as proposed in 2009 by the Society of Interventional Radiology [12]. The total AK is the procedure cumulative Air Kerma at the interventional reference point (defined at 15 cm on the tube side of the isocenter) and is measured in Gray (Gy). DAP is defined as the integral of AK across the entire X-ray beam emitted from the X-ray tube and is a surrogate measurement for the entire amount of energy delivered to the patient by the beam (Gy × cm2). AK and DAP were measured using ionization chambers mounted at the collimator system and elaborated by a dedicated software.
Fluoroscopy time, number of fluorographies, and volume of iodinated contrast (iopromide 370 mg/ml, Ultravist. Bayer AG. Deutschland) injected were considered as surrogate indicators of the clinical image quality, under the assumption that a lower image quality would lead to longer fluoroscopy times, use of larger volumes of contrast medium, and higher number of fluorographies.
The ambient dose equivalent, considered as an indirect index of the dose received by the staff, was measured with a film badge dosimeter on the C-arm. The staff radiation exposure was intended as environmental dose, not considering personal protective devices and suspended screens, lateral shields, and table curtains.
All procedures considered in the comparison were performed by the same team, composed of six interventional radiologists who, at the time of the implementation, had already accrued between 10 and 30 years of experience. The relative experience in standard and complex EVAR was the same for all the first operators involved. The first operator was allowed to change the angiographic system configuration depending on the need, even within the same procedure. All demographic and procedural data were recorded by the nursing staff in a dedicated electronic registry.
The study was retrospective without any study-related clinical intervention and conducted in good clinical practice according to the Helsinki Declaration of 1975 and subsequent modifications. All patients at the time of the procedure had been informed about the possible use of their data for study purposes and signed an informed consent form. Patients’ information was anonymized prior to the analysis.
Statistical analysis
Continuous variables were checked for normality with the Shapiro-Wilks test. Normality was accepted for age and BMI, which are expressed as mean ± standard deviation. Normality was rejected for all other variables, which are reported as median, first quartile Q1 (25th percentile) and third quartile Q3 (75th percentile). Data were compared with Mann–Whitney’s nonparametric test and displayed graphically by box plots, which allow visualizing sample mean, median, and the upper and lower (first and third) quartiles. Correlations between variables were expressed by Pearson’s linear correlation coefficient r.
Categorical variables, reported as counts and percentages were arranged in 2 × 2 contingency tables and studied with the Chi-square test with Yates’ correction.
Statistical significance was set at two-tail p < 0.05. Statistical tests were run on StatPlus:Mac v.6 (AnalysisSoft. Walnut. CA. USA).
Results
The comparison between normal-dose and Eco-dose protocol was carried out separately for standard and complex EVARs. The variables considered were: age, gender, BMI, AK, total DAP, fluoroscopy time, number of fluorographies, and volume of contrast medium injected.
To shield the possible confusing effect of the reduction of the number of performed fluorographies consequent to the staff’s training, we report for each EVAR the value of the fluorography-related DAP (DAPf) normalized to the number of performed fluorographies (Nf).
The outcome of the two comparisons is shown in Table 2 for standard EVARs and Table 3 for complex EVARs. For both standard and complex EVARs, the patients’ baseline showed no difference between the normal-dose samples and the Eco-dose samples.
Conversely, the dose-related variables DAP, DAPf/Nf, and AK showed statistically significant decrements after the switch to the Eco-dose protocol.
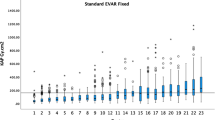
For AK, the reduction was about 45% for standard and 57% for complex EVARs (Fig. 1a); the DAP reduction was 53% for standard and 57% for complex EVARs (Figs. 1b, 3).

Box plot of AK (a) and DAP (b) for standard (normal and Eco protocol) and complex (normal and Eco protocol) EVAR procedures. The bottom and top hinges of the boxes are the first (Q1) and third (Q3) quartiles; the blue band inside the box is the second quartile (median), and the red line is the sample mean
The fluoroscopy time (Fig. 2a) and the number of fluorographies (Fig. 2b) did not show symptoms of having been increased by the reconfiguration: no increase in the fluoroscopy time (p = 0.90 for standard and 0.22 for complex EVARs) nor in the number of fluorographies, which actually significantly decreased for complex EVARS (p = 0.04), thanks to the training.

Box plot of the fluoroscopy time (a) and of the number of fluorographies (b) for standard (normal and Eco protocol) and complex (normal and Eco protocol) EVAR procedures. The bottom and top hinges of the boxes are the first (Q1) and third (Q3) quartiles; the blue band inside the box is the second quartile (median), and the red line is the sample mean
The volume of contrast medium injected decreased from 82.4 ± 42.1 ml for normal dose to 63.5 ± 35.6 ml for Eco dose in standard EVAR (p = 0.09) and from 162.5 ± 32.1 to 98.4 ± 36.1 ml for complex EVARs (p < 0.0001).
The ambient dose equivalent went from 333 mSv/1000 procedures to 248 mSv/1000 procedures with a reduction of 25%.

Box plot for the DAP/Nf. The bottom and top hinges of the boxes are the first (Q1) and third (Q3) quartiles; the blue band inside the box is the second quartile (median), and the red line is the sample mean
Discussion
EVAR procedures may be highly irradiating for patients, possibly leading to skin injuries, as well as to stochastic effects. Since their frequency and complexity significantly increased in the last few years, every effort should be made to decrease the patient’s exposure as much as possible [19].
Our results, in terms of dose reduction, are substantially in line with those obtained by other studies using the most recent technical innovations, such as the Allura Clarity system (Philips Healthcare, Best, the Netherlands) (Table 4).
Van den Haak et al. [6] registered over all EVARs a 56% reduction in AK and 57% in DAP, after the implementation of the Allura Clarity FD20 system. This study did not distinguish between standard and complex EVAR, making difficult a direct comparison with our series, but the figures are consistent. De Ruiter and colleagues [18] evidenced a reduction in DAP of about 36% for not-complex EVARs and 32% for complex EVARs performed with a fixed C-arm equipped with Allura Clarity image-processing technology. In that study, a median DAP of 157.0 Gy cm2 and a median AK of 600 mGy in not-complex EVAR and a median DAP of 598.2 Gy cm2, with a median AK of 3700 mGy, in complex EVAR were, respectively, registered. Another study [17] showed a dose reduction of about 60% in complex endovascular procedures [CEP] after the implementation of the Allura Clarity image-processing system; the reduction was more effective in lower extremity interventions, up to 70% in fluorography and 47% in fluoroscopy, than in complex EVARs (up to 44% in fluorography and 37% in fluoroscopy). Absolute X-ray doses in simple EVAR procedures were 157 Gy cm2 (DAP) and 560 mGy (AK), while they were 372 Gy cm2 (DAP) and 2580 mGy (AK) in complex EVAR procedures. Both these studies, however, considered as complex only fenestrated EVAR and do not mention any embolization performed to prevent type II endoleaks.
It is important to remember that while the recent technical innovations attempt to maintain or enhance the image quality, the Eco dose achieves a lower dose irradiation at the expenses of some clinical image quality loss. Granted that the image quality is necessarily higher when using high radiation doses, the Eco-dose protocol has, however, been successfully optimized to obtain an acceptable image quality with the lowest possible dose according to the various procedures, as proven by the fact that fluoroscopy times, number of fluorographies, and contrast medium volumes did not have to be increased, with the latter two actually significantly decreasing. The normalized variable DAPf/Nf was introduced to enhance the effect of the Eco protocol, independently from the reduction in the number of fluorographies achieved thanks to the staff’s training; of course, it was the synergy between machine reconfiguration and staff training that allowed a reduction close to 60% for complex EVARs.
The exposure dose reduction for the patients was paralleled by a decrease in the staff exposure, quantified in − 26%. This result is consistent with what was achieved with the Allura Clarity technology by van den Haak (− 16%). It must be remembered that the operator is typically exposed to a dose rate approximately 0.1% the entrance skin exposure dose rate to the patient 1 m from the center of the fluoroscopic field [11].
This study has some limitations. First, it is a retrospective study on a limited number of patients. Second, while other studies considered as complex EVARs only chimney/fenestrated/branched EVAR, we classified as complex EVARs also the intraoperative embolizations to prevent endoleak type II, usually performed at our institution. Third, we evaluated the impact of the reconfiguration on the image quality only indirectly, through surrogate measurements as fluoroscopy time, number of fluorographies, and volume of iodinated contrast injected. Fourth, the staff dose was intended as environmental dose, not considering personal protective device and suspended screens, lateral shields, and table curtains.
Conclusions
The improvement of available resources, by optimizing the angiographic system settings and training in radiation protection the hybrid operating room staff, allowed to significantly reduce the radiation dose, thereby ensuring safer EVAR procedures both for patients and staff.
References
Dua A, Kuy S, Lee CJ et al (2014) Epidemiology of aortic aneurysm repair in the United States from 2000 to 2010. J Vasc Surg 59:1512–1517. https://doi.org/10.1016/j.jvs.2014.01.007
Santosa F, Moysidis T, Nowak T et al (2012) Endovascular abdominal aneurysm repair: trends in Germany. VASA Z Gefasskrankheiten 41:268–274. https://doi.org/10.1024/0301-1526/a000202
Weerakkody RA, Walsh SR, Cousins C et al (2008) Radiation exposure during endovascular aneurysm repair. Br J Surg 95:699–702. https://doi.org/10.1002/bjs.6229
European Society of Radiology (ESR) (2015) Summary of the European Directive 2013/59/Euratom: essentials for health professionals in radiology. Insights Imaging 6:411–417. https://doi.org/10.1007/s13244-015-0410-4
Valentin J (2000) Avoidance of radiation injuries from medical interventional procedures. Ann ICRP 30:7–67. https://doi.org/10.1016/S0146-6453(01)00004-5
van den Haak RFF, Hamans BC, Zuurmond K et al (2015) Significant radiation dose reduction in the hybrid operating room using a novel X-ray imaging technology. Eur J Vasc Endovasc Surg Off J Eur Soc Vasc Surg 50:480–486. https://doi.org/10.1016/j.ejvs.2015.06.025
Kirkwood ML, Arbique GM, Guild JB et al (2013) Surgeon education decreases radiation dose in complex endovascular procedures and improves patient safety. J Vasc Surg 58:715–721. https://doi.org/10.1016/j.jvs.2013.04.004
Haqqani OP, Agarwal PK, Halin NM, Iafrati MD (2012) Minimizing radiation exposure to the vascular surgeon. J Vasc Surg 55:799–805. https://doi.org/10.1016/j.jvs.2011.08.055
Fetterly KA, Mathew V, Lennon R et al (2012) Radiation dose reduction in the invasive cardiovascular laboratory: implementing a culture and philosophy of radiation safety. JACC Cardiovasc Interv 5:866–873. https://doi.org/10.1016/j.jcin.2012.05.003
Peach G, Sinha S, Black SA et al (2012) Operator-controlled imaging significantly reduces radiation exposure during EVAR. Eur J Vasc Endovasc Surg 44:395–398. https://doi.org/10.1016/j.ejvs.2012.08.001
Mitchell EL, Furey P (2011) Prevention of radiation injury from medical imaging. J Vasc Surg 53:22S–27S. https://doi.org/10.1016/j.jvs.2010.05.139
Stecker MS, Balter S, Towbin RB et al (2009) Guidelines for patient radiation dose management. J Vasc Interv Radiol JVIR 20:S263–S273. https://doi.org/10.1016/j.jvir.2009.04.037
Walker TG, Kalva SP, Ganguli S et al (2012) Image optimization during endovascular aneurysm repair. AJR Am J Roentgenol 198:200–206. https://doi.org/10.2214/AJR.11.6608
Miller DL, Balter S, Noonan PT, Georgia JD (2002) Minimizing radiation-induced skin injury in interventional radiology procedures. Radiology 225:329–336. https://doi.org/10.1148/radiol.2252011414
van Dijk JD, Ottervanger JP, Delnoy PPHM et al (2017) Impact of new X-ray technology on patient dose in pacemaker and implantable cardioverter defibrillator (ICD) implantations. J Interv Card Electrophysiol 48:105–110. https://doi.org/10.1007/s10840-016-0200-z
Gislason-Lee AJ, Keeble C, Malkin CJ et al (2016) Impact of latest generation cardiac interventional X-ray equipment on patient image quality and radiation dose for trans-catheter aortic valve implantations. Br J Radiol 89:20160269. https://doi.org/10.1259/bjr.20160269
Kirkwood ML, Guild JB, Arbique GM et al (2016) New image-processing and noise-reduction software reduces radiation dose during complex endovascular procedures. J Vasc Surg 64:1357–1365. https://doi.org/10.1016/j.jvs.2016.04.062
de Ruiter QMB, Moll FL, Gijsberts CM, van Herwaarden JA (2016) Allura Clarity radiation dose-reduction technology in the hybrid operating room during endovascular aneurysm repair. J Endovasc Ther Off J Int Soc Endovasc Spec 23:130–138. https://doi.org/10.1177/1526602815622433
Ryckx N, Sans-Merce M, Meuli R et al (2016) System upgrade on philips allura FD20 angiography systems: effects on patient skin dose and static image quality. Radiat Prot Dosim 169:313–318. https://doi.org/10.1093/rpd/ncv484
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
All procedures were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Ruffino, M.A., Fronda, M., Discalzi, A. et al. Radiation dose during endovascular aneurysm repair (EVAR): upgrade of an angiographic system from standard to Eco mode. Radiol med 123, 966–972 (2018). https://doi.org/10.1007/s11547-018-0924-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-018-0924-1