
Abstract
Purpose
Definition of the role of real-time elastography (RTE) in the evaluation of response to treatment of uterine fibroids using MRgFUS in symptomatic patients.
Materials and methods
28 women with 34 symptomatic fibroids, selected for MRgFUS, were enrolled. The patients were preliminarily studied with MRI and suprapubic and transvaginal ultrasound examination including RTE; the follow-up was performed immediately after treatment, at 3 months and 12 months with the same technique. Each lesion was evaluated by looking for ultrasound parameters (volume, resistance index) and RTE strain ratio (SR). Before and after treatment, all patients completed three questionnaires for symptom evaluation (e.g., uterine fibroids symptoms and quality of life).
Results
Of the 27 treated fibroids, only 14 had an effective treatment with non-perfused volume (NPV) >70 %. After 3 months of treatment, 17/21 patients presented significant decrease of uterine bleeding. A positive correlation between %NVP and percentage of fibroid volume decrease was seen. Reduction of SR value from t0 to t2 was found in 19/27 fibroids, particularly significant in fibroids with NPV > 70 %. A significant positive correlation between the percentage of symptom decrease and %SR decrease was found. At the time of statistical analysis, 12/21 patients reached the 12-month follow-up: they showed a further reduction of SR.
Conclusion
RTE is a valid method able to support standard ultrasound examination in the evaluation of uterine fibroids, since it allows demonstrating the decrease of rigidity, which can be quantified with the SR parameter. It could be included in a pre-treatment multiparametric evaluation of patients looking for MRgFUS eligibility and in follow-up when it could assess the response to treatment.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Uterine fibroids are the most frequent benign tumors of myometrial origin with an incidence ranging from 20 to 40 % in reproductive age women [1, 2]. They are composed of the same smooth muscle fibers as the uterine wall and fibrous connective tissue in various percentages.
Estrogens, growth hormone and progesterone influence their growth rates [3].
In 50–60 % of cases, fibroids are asymptomatic and their diagnosis is incidental. The most common symptoms are abnormal uterine bleeding [4], dysmenorrhea, bulk symptoms of pressure, pelvic pain and infertility.
The severity of symptoms plays a crucial role in the choice of the therapeutic approach, which can range from medical treatment (GnRH analogs, oral contraceptive and progestins) to surgery. Hysterectomy is a common option, but it represents an invasive chance [5]. Other uterine-sparing therapeutic options include myomectomy, uterine artery embolization (UAE) and magnetic resonance guided focused ultrasound surgery (MRgFUS) [6].
MRgFUS is a totally non-invasive thermal ablation procedure for treating symptomatic uterine fibroids [7].
MRgFUS is based on the use of high-intensity focused ultrasound waves delivered by an extracorporeal transducer to generate high temperatures within the target tissue (>56 °C) with consequent cell death and coagulative necrosis without damage to the surrounding area.
Careful selection of patients is crucial for the success of the treatment: potential candidates are screened with pelvic MRI to determine if they meet the patient selection guidelines outlined by Yoon et al. [8].
During the procedure, real-time images of the expected path of the US beam are obtained, and the induced temperature in the fibroid is measured by MR thermometry. The aim of the treatment is to ablate as much of the fibroid as possible, with multiple sonications targeting different portions [9].
According to other clinical experiences, the resulting “non-perfused volume” (NPV), as assessed at post-treatment magnetic resonance with gadolinium, at more than 70 % represents an effective treatment [10, 11].
Real-time elastography (RTE) is a US complementary technique that studies the elastic properties of the examined tissue, improving the characterization of lesions.
Real-time elastography is based on slight external tissue compression by the US probe on the examined structures; this compression produces displacement within the tissue, with subsequent calculation of the strain profile along the axis of compression.
Strain is the level of deformation and is inversely proportional to stiffness: soft tissues are more easily compressible, presenting a higher value of strain. Real-time strain ratio (SR) between healthy and pathological tissue is a useful quantitative parameter that is possible to calculate.
According to the “color map scale”, the stiffness of the tissue is represented in a range of colors from red (soft) to blue (hard).
Although uterine fibroids are composed of the same smooth muscle fibers as the myometrium, they are many times denser; this is the reason why they appear stiffer at RTE.
MRgFUS on uterine fibroids determines the colliquative necrosis of the treated lesions and, as shown in the literature, reduction of symptoms without substantial reduction of volume. MRI with gadolinium shows reduction of vascularized tissue (NPV) in patients effectively treated, but the reason why symptoms reduce is still not clear.
We assume that fibroids become softer and less compressive on endometrial layers, leading to reduction of bleeding and pain and increase of fertility.
Ultrasound elastography could explore the elastic pattern of fibroids before and after treatment.
The objective of our study was to evaluate the usefulness of RTE in the characterization of uterine fibroids before and after treatment with MRI-focused ultrasound.
Materials and methods
Twenty-eight women, with a total of 34 uterine symptomatic fibroids (average age 38 years, range 30–48 years), had been selected for MRgFUS treatment (ExAblate 2000; InSightec, Haifa, Israele) in a time period of 1 year and were enrolled.
The research ethics committee approved this prospective study and all patients signed the informed consent form.
Inclusion criteria required at most three fibroids eligible for MRgFUS treatment (symptomatic patients, who had not undergone surgical approach before, with at least one fibroid bigger than 10 cm, hypointense on T2-weighted MRI, not exophytic or pedunculated) and good visualization of the fibroid with transvaginal scan. Exclusion criteria were: more than three treatable fibroids, MRI imaging indicative of leiomyosarcoma, hypointense lesion on T2W imaging, distance from the skin and the fibroid more than 12 cm, fibroids close to the lumbosacral plexus or to another bone surface, air-containing tissues or bone between transducer and fibroid, poor visualization of the fibroid with transvaginal US and no possibility to perform transvaginal examination.
The eligible patients were preliminarily studied with suprapubic US, with convex probe 2–5 MHz, then with transvaginal US, with intracavitary probe 3.3–8.8 MHz (Aplio 500, Toshiba Medical Systems Europe, Zoetermeer, The Netherlands). This preliminary US study (t0) included assessment of the lesions in B-mode (max diameter), color and power Doppler with measure of resistance index (RI), and elastographic study. The preliminary MRI study (Discovery MR750 3-Tesla machine General Electric, Milwaukee, WI, USA) was performed with T2-weighted and T1-fat suppression weighted sequences, before and after contrast media acquired in multiple planes and was useful for collecting volume and maximum diameter information (respectively, cm3 and cm).
After MRgFUS treatment, follow-up with Transvaginal RTE was planned immediately after treatment (within 2 h after treatment conclusion, t1) and at 3 months (t2). Patients who completed the 1-year follow-up were also evaluated at the 12 months follow-up (t3).
Patients also had pelvic MRI at t1, t2 and t3 with the same protocol as for t0 MRI.
Each lesion was evaluated by looking for US (maximum diameter, resistance index—RI) and RTE (color map and SR) parameters, which were evaluated by three operators in consensus, while MRI parameters at t0 included volume (cm3) and maximum diameter, at t1 only NPV and at t2 and t3 volume, maximum diameter and NPV.
Before the treatment (t0) and after 3 months (t2), all patients were asked to fill out three questionnaires evaluating clinical conditions and allowing evaluation of prevalent symptoms and improvement during follow-up: uterine fibroids symptoms and quality of life (UFS-QoL, for the degree of gynecological bleeding), King’s Health Questionnaire (KH, for urinary symptoms) and Female Sexual Function Index (FSFI, for sexual disorders).
During the study, three patients voluntarily quitted the t2 follow-up, while for four of them the transvaginal scan could not be performed (three patients had menometrorrhagia during the treatment and 1 patient presented voluminous posterior fibroid, located in the uterine body fundus with retroverted uterus).
Therefore, 21 patients with 27 fibroids represented the final study population (Table 1); 5/21 assumed GnRH therapies.
RTE has been performed by a sequence of mild compression/decompression of the uterine fibroid in the transvaginal approach, with subsequent evaluation of the elastogram using a dedicated software. The protocol consisted of two cycles of compressions; the correct pressure could be checked as a sinusoidal curve on a chart appearing in real time at the bottom of the elastogram.
The SR measurement was determined by comparing the strain in two manually selected regions of interest (ROI) on the best elastogram. The target ROI is centered on the leiomyoma (size 10–15 mm) and the reference ROI is placed on the surrounding myometrium at the same depth. Different sizes of target ROI were drawn: big target ROI, the same size as the fibroid, and small target ROI, of similar size to reference ROI, placed in five standard regions of the fibroid.
The SR is the ratio between the target ROI and reference ROI.
We selected five big target ROI and five small target ROI for each cycle of compression, and the strain ratio was automatically calculated for each ROI by Toshiba’s software.
At the end of the MRgFUS procedure, the non-perfused volume (NPV) was measured.
All patients were evaluated at t0, t1 and t2; only 12 patients reached the t3 follow-up at the time of the statistical analysis.
Statistical analysis
As of today, no previous experience in the literature regarding the elastographic evaluation of uterine fibroids treated with MRgFUS is available. Our experience does not present statistical references and is a preliminary study. The results are shown as median.
Wilcoxon sum-ranked test was used to compare the difference between the RI and SR values at t1, and volume, symptoms, RI and SR values at t2 with those at baseline (t0).
Linear regression analysis and Spearman correlation were used to evaluate the presence of correlation between NPV and ecographic and elastographic parameters at t1 and t2 to consider if the SR value could be an effective index to evaluate the effectiveness of treatment.
Same analyses were performed comparing all parameters examined, considering as outcome variables: NPV ≥70 %, volume reduction ≥50 % on t2 and symptoms reduction ≥50 %.
Statistical analysis was performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and all tests were two-tailed. p < 0.05 was considered to be statistically significant.
The same analyses were performed for the patients who underwent the 1-year follow-up (t3).
Results
At t0, before MRgFUS, the characteristics of the 27 fibroids analyzed were as follows: MRI volume average 82.2 cm3 (2.18–404.7, SD 98.2 cm3), MRI maximum diameter average 6.9 cm (range 3.3–9.5 cm SD 2 cm), US maximum diameter average 6.7 cm (range 3.5–9.4 cm, SD 1.8 cm), RI average 0.62 (range 0.32–0.90, SD 0.13) and SR average 5.73 (range 0.56–22.11, SD 5.96). For symptom analysis, only UFS questionnaire scores were collectable for statistical analysis, with a pre-treatment average score of 47.64 (range 3.13–100, SD 21.73; score reference from 0 to 100 with 100 representing the maximum grade of symptoms).
At t1, the volume was not re-assessed. The NPV ratio of the 27 treated fibroids was 69 % (range 16–99 %); 14/27 fibroids had an effective treatment with NPV >70 %, and the remaining had incomplete treatment (NPV < 70 %). RI at Doppler US study was not assessable in 8/27 fibroids (no vascular signal inside the lesion), while in the remaining 19 fibroids the RI average was 0.75 (range 0.42–0.93, SD 0.18). The SR average was 7.68 (range 0.29–31.3, SD 8.01). Questionnaires were not collected at the t1 follow-up.
At t2, the parameters changed as follows: MRI volume average 74.9 cm3 (range 1.2–322 cm3, SD 88.5 cm3); MRI maximum diameter average 6.3 cm (range 3.1–9.2 cm, SD 2 cm; NPV was not assessed; US maximum diameter 6 cm (range 2.9–9.9 cm, SD 2.2 cm); RI was not assessable in ten fibroids; in the remaining 17 fibroids, the RI average was 0.60 (range 0.43–0.82 SD 0.10). The SR average was 3.30 (range 0.83–17.35, SD 3.26). The UFS score was average 30.36 (range 6.25–90.62, SD 19.9).
Statistically significant differences between t0 and t1 were found only for US–RTE parameters (p < 0.05): RI was not found in 8/27 fibroids (29.6 %) and at an average of 0.75 in 19/27, with increase in average of 25 %; SR increase was 34 %.
The t0 versus t2 differences between all parameters was found as follows: between MRI volume and US/MRI, the maximum diameter difference was not statistically significant, and average reduction of volume in MRI was not statistically significant (8.9 %, p = 0.055). RI was not measurable in 10/27 fibroids; in the remaining 17 fibroids, RI was quite similar to t0 (p = 0.055). SR reduced to 42.4 % (statistically significant reduction with p < 0.05).
Considering the symptoms t0–t2, investigated with the mentioned questionnaires, only the UFS questionnaire showed significant results (p < 0.008): in all patients, the reduction of symptoms was 36 %, while 17/21 patients presented, after 3 months, a decrease of 50 % of symptoms (average value). The scores from the other questionnaires were not statistically analyzed because of lack of data.
Considering the fibroids volume, difference between the volume (calculated on MRI T1-post Gd) at t0 and t2 was not statistically significant (p = 0.055).
Concerning the correlations between all parameters analyzed at t0, t1 and t2, we found some positive and statistically significant correlations (Spearman correlation, r = 0.41–0.75) between:
-
NPV and %volume decrease at t2 (p = 0.01);
-
SR values at t0 and t2 (p < 0.008); 19/27 fibroids showed a reduction of SR value (median of decrease: 42.4 %); in particular, significant decrease of SR was found in the patient group with NPV >70 (Figs. 1, 2; Table 2). Of the remaining fibroids, 5/27 had a significant increase of SR value (Figs. 3, 4; Table 3);
Fig. 1 
A 41-year-old female with an intramural fibroid of the anterior wall of the uterus. a T2 coronal MRI image shows hypointense fibroid at t0. b T1 post- gadolinium axial plane shows the highly perfused fibroid sufficiently distant from the sacral surface and with minimum distance from the skin. c At the end of the MRgFUS treatment, T1-weighted gadolinium-enhanced axial image is performed to demonstrate the effect of the ablation and to calculate the area of non-perfused volume corresponding to coagulative necrosis (NPV 71 %). Axial T1 post-contrast scan at 3 months (d) and 12 months follow-up (e) showing the fibroid volume reduction
Fig. 2 
Real-time elastosonography images of the fibroid shown in Fig. 1. The strain ratio is evaluated by comparing the mean strain in a region of interest centered on the myoma (big, light pink target Roi), with the mean strain in a region of interest in the surrounding myometrium (small, light yellow reference Roi), and by choosing the best curve in the elastogram. The strain ratio value was 4.47 at t0 (a), 22.1 at t1 (b), 3.56 at the 3 months follow-up (c) and 2.70 at t3 (d)
Table 2 Summary of volume, symptoms, resistance index and strain ratio changes in Case 1, Figs. 1 and 2 Fig. 3 
A 34-year-old female with a voluminous intramural fibroid localized at the top of the uterus. a At time 0, T2 coronal MRI image shows hypointense fibroid with hyperintense central area (hyaline degeneration), b highly perfused on T1 post-gadolinium axial plane. c After treatment, the T1 post-gadolinium axial image allows to calculate the NPV. The NPV was 48 %; therefore treatment was not technically efficient. Axial T1 post-contrast scan at 3 months (d) shows a size increase of the fibroid with a repopulation of the central necrotic portion. The patient underwent myomectomy 5 months after treatment
Fig. 4 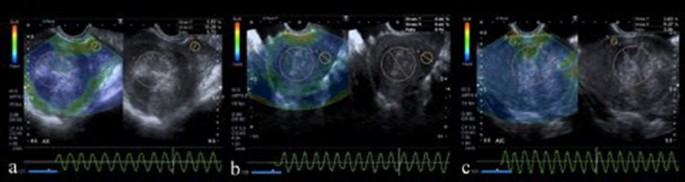
Real-time elastosonography images of the fibroid shown in Fig. 3. The strain ratio was 0.94 before treatment (a), 27.1 at t1 (b) and 1.81 at t2 (c). The myoma did not respond well to the treatment (NPV 48 %) and had an increase of the SR at the 3 months follow-up. Note how the B-mode ultrasound imaging at t0 showed a heterogeneous hyperechoic fibroid, as hyaline degeneration
-
NPV and SR on t1 (p < 0.05); SR on t1 and the %SR decrease at t2 (p = 0.005);
-
% symptoms decrease (SSS) and %SR decrease at t2 (p < 0.001);
-
NPV and %RI decrease on t2 (p < 0.05).




In the total of 21 patients, we had non-successful treatment in 5; during the 12-month follow-up, 2 patients became pregnant, 1 patient underwent a second MRgFUS treatment, 4 patients underwent myomectomy at the 5, 8, 8 and 11 months follow-up and 1 patient elected to withdraw from the study. One patient did not arrive at the 1-year follow-up.
In the end, only 12 fibroids in 12/21 patients were included for the 12 months follow-up (complete flowchart in Fig. 5). In these patients, we found a further decrease of SR (SR value at t0 6.08, range 0.56–22.11, SD 6.64; SR at t3 2.01, range 0.1–5.5, SD 1.48, p < 0.01), while volume and RI changes were not significant, in comparison with t2 (p > 0.05).

Flowchart of the study population
Concerning strain ratio evaluation, for all t0, t1, t2 and t3 follow-up, no statistically significant difference between big ROI and small ROI was found. Therefore, the statistical analysis was performed on big ROI data.
Discussion
It has been widely demonstrated in the literature that the clinical outcome of MRgFUS fibroid treatment primarily depends on the non-perfused volume (NPV) measured on contrast-enhanced T1-weighted imaging immediately post-treatment [12, 13].
The literature shows NPV from 30 to 80 %, with very variable volumetric decreases (from 15 to 40 %) [14].
Good selection of patients is the most important parameter able to predict treatment success: patients have to be symptomatic and symptoms must be correlated with uterine fibroids. This is the reason why optimal integration between the gynecologist, radiologist and patient is necessary.
Our results showed that in the majority of patients, there was a relatively small decrease of fibroid volume at the 3 months follow-up combined with good symptoms reduction.
RTE allowed to understand the reason of this event and to quantify elasticity changes of fibroids.
There are only a few reports in the literature on the in vivo use of real-time transvaginal elastography of gynecological interest.
Hobson et al. performed in vitro ultrasound strain imaging on 29 uteri removed via elective hysterectomy for irregular uterine bleeding. They showed that ultrasound strain imaging does provide differentiation between normal uterine muscle tissue and pathologies such as leiomyomas, and that a uterine leiomyoma may be better distinguished from the normal surrounding myometrium on strain images by the presence of a slipping artifact at the boundary of the leiomyoma [12].
In 2009, the French group of Ami performed real-time transvaginal elastography in ten patients with uterine fibroids to demonstrate the feasibility of the technique to map and characterize these lesions [13].
Our experience is the first in vivo study exploring the utility of elastography to evaluate the modifications of elasticity in uterine fibroids after MRgFUS treatment. The aim of MRgFUS treatment is not mainly to decrease the size of the treated fibroids, but mostly to reduce their dense texture, which is supposed to be the main cause of symptoms (for compressive effects).
The elastographic examination showed a significant variability between SR values of the fibroids before the treatment with an average value of 5.73 (range 0.56–22.11, SD 5.96). These results are concordant with those in the literature [13, 15].
Immediately after treatment, the evaluation of the same myomas showed a significant increase of SR, with a median of 7.68. We explained this response with a “reactive change”: the treated fibroids, especially the ones efficiently treated (NPV > 70 %), had an increase in their stiffness within 2 h after treatment, since coagulative necrosis and inflammatory fall from MRgFUS produce intralesional tension with increase of rigidity of the lesion itself. On these days, the inflammatory reaction is replaced with complete coagulative necrosis and granulation tissue, which will determine the decrease of stiffness and symptoms.
We showed that all patients with >70 % NPV at t1—technically efficient treatment—had significant increase of SR values (average increase of 50 %) immediately after treatment, demonstrating our hypothesis: RTE parameters can be used immediately after treatment to verify effective treatment, adding useful information to CE-MRI.
The percentage of SR decrease at 3 months follow-up is positively and significantly correlated with symptom reduction (p = 0.001): patients who responded well to the treatment had a decrease of SR, while patients who did not respond had an increase of SR already after 3 months.
Therefore we can state that in our cohort of patients, elastographic evaluation could predict the treatment efficacy and could have an important role during the follow-up of patients with uterine fibroids treated with MRgFUS.
Our experience needs to be confirmed with more data, which are necessary to consolidate these results and could draw attention to some pre-treatment characteristics.
In our study, we had some ineffective treatments. Almost 40 % of the treated fibroids presented an NPV < 70 %; this result gave us the chance to compare the two groups (NPV < 70 % to NPV > 70 %) and allowed us to look for the parameters that have to be strictly evaluated for a correct selection of patients to make the treatment efficient.
No significant differences in the efficacy of treatment were observed in the patient group which had GnRh therapies performed (p > 0.05).
A multiparametric evaluation, including symptoms, MR signal, localization, size and echo-elastographic pattern, could be useful for a better selection of fibroids for MRgFUS treatment.
In our cohort, the efficacy of the treatment by NPV corresponded with the data presented in other studies and showed a positive and significant correlation with size decrease at the 3 months follow-up.
Only 12 patients completed the 12 months follow-up and the majority of them (83 %)had a further decrease of SR, reduction of symptoms and reduction of fibroid volume. They had efficient treatment with NPV > 70 %. Two patients presented an increase of volume, a worsening of symptoms and increase of SR as compared to t0: these patients had an ineffective treatment with an NPV of 30 and 16 %.
Multiparametric US–RTE could be useful to complete the evaluation of patients treated with MRgFUS and support MRI examinations during follow-up, as it is able to measure the volume and residual vascularization of the fibroid as well as stiffness changes. If the results are confirmed in a much larger study population, US–RTE could even substitute MRI at the 3 months follow-up.
Significant symptom reduction was found already at the 3 months follow-up, with a median decrease of 36 %. We observed a variable response to the treatment in patients with partial ablation, not completely reasonable, varying from the significant symptom increase in patients with an NPV of 40 % to a remarkable and not-justified symptom reduction (up to 60 %) in incomplete treatments (NPV 32 %).
These results led us to some observations. First of all, the questionnaires to evaluate the symptoms are tentative to quantify a complex symptomatology and this leads to discordant results compared to the real modification of symptoms. This is the reason why the FSFI and KH-QoL questionnaires, first included in the protocol, were then excluded from statistical evaluations, since patients showed difficulties in the interpretation of questions, with consequent lack of data.
One more observation concerns the menometrorrhagic symptoms, which could be caused by other gynecologic pathologies, leading to wrong interpretation. This could represent a bias of the study. That is why we found both, communication with the patient and good selection, crucial for treatment success.
Some limitations of the present study are found: small cohort of patients and lack of previous experience in literature for elastographic examinations are the main.
Our cohort of patients was small because of the long-term follow-up, the difficulties about the organization of the examinations and the exclusion of some patients for various reasons (e.g., menstrual bleeding during treatment, transvaginal examination not being possible, etc.).
One of the major difficulties of RTE is the choice of reference ROI on normal myometrium, especially in case of big fibroids. Moreover, it was not always possible to place both ROIs at the same distance from the probe. In few occasion the trans-vaginal ultrasonographic anatomy and the location of the fibroid compared with the myometrium imposed us to draw the target ROI deeper than the reference ROI, with consequent possible bias.
The introduction of recent techniques—as new elastographic software with the automatic positioning of the ROI and the possibility to control the cycles of compression with a reference box—seems to be a good method to improve the reliability.
However, this preliminary study permitted to gain experience in endocavitary elastography and opened the door to future studies.
Conclusions
MRgFUS is a method for treating uterine fibroids in symptomatic patients who want to preserve fertility. The follow-up of patients shows that while the size has a slight decrease, the symptoms present a substantial reduction. This event can be explained by the reduction of the stiffness of the fibroids, due to the substitution of the solid tissue with coagulative tissue.
RTE allowed us to demonstrate that after treatment, the fibroids show a decrease of their rigidity, which can be quantified with the SR parameter. With pre-treatment and post-treatment study, it has been possible to show that fibroids with a high SR before treatment presented a better response than others with lower SR and reached an NPV > 70 %.
At the same time, successfully treated fibroids (NPV > 70 %) presented a significant increase of their SR immediately after treatment: coagulative necrosis and inflammation produce intralesional tension and increase the rigidity of the lesion itself.
At the 3 months follow-up, patients with NPV > 70 % had a good reduction of symptoms, a little decrease of size and a significant decrease of SR, compared with not efficiently treated patients.
In conclusion, real-time elastography could be a valid method, able to support standard ultrasound examination in the evaluation of uterine fibroids. Especially in symptomatic patients, it may be included in a pre-treatment multiparametric evaluation to allow a better selection of patients for the most suitable treatment.
Real-time elastography could also be important during follow-up: immediately after treatment (when the multiparametric evaluation could predict the response to treatment) and at 3 months follow-up (when it has the potential to substitute MRI), since it is able to evaluate the decrease of size and vascularization, as well as changes in stiffness.
References
Ryan GL, Syrop CH, Van Voorhis BJ (2005) Role, epidemiology, and natural history of benign uterine mass lesions. Clin Obstet Gynecol 48(2):312–324
Wallach EE, Vlahos NF (2004) Uterine myomas: an overview of development, clinical features, and management. Obstet Gynecol 104(2):393–406
Stovall DW (2001) Clinical symptomatology of uterine leiomyomas. Clin Obstet Gynecol 44(2):364–371
Rein MS, Barbieri RL, Friedman AJ (1995) Progesterone: a critical role in the pathogenesis of uterine myomas. Am J Obstet Gynecol 172:14–18
Fernandez H, Sefrioui O, Virelizier O, Gervaise A, Gomel Frydman R (2001) Hysteroscopic resection of submucosal myomas in patients with infertility. Hum Reprod 16:1489–1492
Khan AT, Shehmar M, Gupta JK (2014) Uterine fibroids: current perspectives. Int J Womens Health 6:95–114
Napoli A, Anzidei M, Ciolina F, Marotta E, Marincola BC, Brachetti G, Di Mare L, Cartocci G, Boni F, Noce V, Bertaccini L, Catalano C (2013) MR-guided high-intensity focused ultrasound: current status of an emerging technology. Cardiovasc Intervent Radiol 36(5):1190–1203
Yoon SW, Lee C, Cha SH, Yu JS, Na YJ, Kim KA, Jung SG, Kim SJ (2008) Patient selection guidelines in MR-guided focused ultrasound surgery of uterine fibroids: a pictorial guide to relevant findings in screening pelvic MRI. Eur Radiol 18(12):2997–3006
Morita Y, Ito N, Hikida H, Takeuchi S, Nakamura K, Ohashi H (2008) Non-invasive magnetic resonance imaging-guided focused ultrasound treatment for uterine fibroids—early experience. Eur J Obstet Gynecol Reprod Biol 139(2):199–203
Park MJ, Kim Y-S, Rhim H, Lim HK (2014) Safety and therapeutic efficacy of complete or near- complete ablation of symptomatic uterine fibroid tumors by MR imaging-guided high-intensity focused US therapy. J Vasc Interv Radiol 25(2):231–239
Stewart EA, Gostout B, Rabinovici J, Kim HS, Regan L, Tempany CMC (2007) Sustained relief of leiomyoma symptoms by using focused ultrasound surgery. Obstet Gynecol 110(2):279–287
Hobson MA, Kiss MZ, Varghese T, Sommer AM, Kliewer MA, Zagzebski JA, Hall TJ, Harter J, Hartenbach EM, Madsen EL (2007) In vitro uterine strain imaging: preliminary results. J Ultrasound Med 26(7):899–908
Ami O, Lamazou F, Mabille M, Levaillant JM, Deffieux X, Frydman R, Musset D (2009) Real-time transvaginal elastosonography of uterine fibroids. Ultrasound Obstet Gynecol 34(4):486–488
Pron G (2015) Magnetic resonance-guided high-intensity focused ultrasound (MRgHIFU) treatment of symptomatic uterine fibroids: an evidence-based analysis. Ont Health Technol Assess Ser 15(4):1–86 (eCollection 2015)
Hall TJ (2003) AAPM/RSNA physics tutorial for residents: topics in US: beyond the basics: elasticity imaging with US. Radiographics 23(6):1657–1671
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Chiara Marigliano declares that she has no conflict of interest. Giovanna Panzironi declares that she has no conflict of interest. Luisa Molisso declares that she has no conflict of interest. Alessandra Pizzuto declares that she has no conflict of interest. Federica Ciolina declares that she has no conflict of interest. Alessandro Napoli declares that he has no conflict of interest. Paolo Ricci declares that he has no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Marigliano, C., Panzironi, G., Molisso, L. et al. First experience of real-time elastography with transvaginal approach in assessing response to MRgFUS treatment of uterine fibroids. Radiol med 121, 926–934 (2016). https://doi.org/10.1007/s11547-016-0679-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-016-0679-5