
Abstract
Analysis of the frontal sinus is an important tool in personal identification. Cone beam-computed tomography (CBCT) is also progressively replacing conventional radiography and multi-slice computed tomography (MSCT) in human identification. The aim of this study is to develop a reproducible technique and measurements from 3D reconstructions obtained with CBCT, for use in human identification. CBCT from 150 patients (91 female, 59 male), aged between 15 and 78 years, was analysed with the specific software program MIMICS 11.11 (Materialise N.V., Leuven, Belgium). Corresponding 3D volumes were generated and maximal dimensions along 3 directions (x, y, z), X M, Y M, Z M (in mm), total volume area (in mm3), V t, and total surface (in mm2), S t, were calculated. Correlation analysis showed that sinus surfaces were strongly correlated with their volume (r = 0.976). Frontal sinuses were separate in 21 subjects (14 %), fused in 67 (44.6 %) and found on only one side (unilateral) in 9 (6 %). A Prominent Middle of Fused Sinus (PMS) was found in 53 subjects (35.3 %). The intra- (0.963–0.999) and inter-observer variability (0.973–0.999) showed a great agreement and a substantial homogeneity of evaluation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Radiographic comparison of the frontal sinus is a well-recognized approach for reliable personal identification [1–8]. It has proven particularly useful when antemortem (AM) dental records are not available, when teeth are missing postmortem (PM), or in cases in which soft tissues are decomposed or burned [7–9].
Some typical features of frontal sinus morphology make it a very reliable part of the human skeleton for human identification [10]. The frontal sinus remains stable throughout an individual’s life until old age, when progressive pneumatisation due to atrophic changes may occur [11–14]. The frontal sinus is also preserved intact as its internal bony structure protects it from injury [15–18]. Lastly, it is highly variable in nature and shows differences even between monozygotic twins [16], as demonstrated by several radiographs, among which researchers could not find two identical ones [19, 20].
AM and PM radiographs of the frontal sinuses can be compared by overlapping or coding systems [18, 21]. Overlapping is accepted as a reliable method but it does cause some problems which are overcome by coding systems [22–25].
In spite of the large number of publications relating to the uniqueness of frontal sinuses, there is a real need for more research aimed at quantification [25]. As Christensen stated [20, 25], although many claim that the frontal sinuses are unique to each individual, no empirical studies have ever rigorously tested this statement.
Some recent publications have stressed the possibility of studying frontal sinuses by computed tomography (CT) [26–29]. These techniques provide very good opportunities for studying these anatomical structures with a three-dimensional approach and great precision in all measurements [30]. They also present several advantages over conventional radiographs: superimposition of structures beyond the plane of interest can be avoided, allowing visualization of small differences in density [26, 27, 29]; internal points for evaluation can be easily shown by image segmentation; craniometric points can be precisely located and measurements more accurately performed than on conventional radiographs. Hence, volumes and areas can be determined [27, 28, 31].
Cone beam-computed tomography (CBCT) has recently begun to emerge as a potentially low-dose cross-sectional technique for visualizing bony structures in the head and neck [26, 30]. The technology involves a cone-shaped X-ray beam directed at a flat two-dimensional (2D) detector. As both rotate around the subject’s head, a series of 2D images are generated. The software can then apply a particular algorithm to reconstruct the images into a three-dimensional (3D) dataset [32].
Comparatively low dosing requirements, high-quality bony definition and the compact design afforded by CBCT scanners have made them attractive for office-based and intra-operative scanning of frontal sinuses [32]. Radiation dose is very important because in the field or non-specific location, such as a laboratory, shielding operators are essential [33]. Last but not least, its portability makes it ideally suited to field use. The machine can be transported and easily positioned in place like a cart, allowing its use on virtually any levelled temporary facility [33].
In this context, the most commonly used techniques are based on evaluation of both metric and non-metric characteristics of frontal sinus patterns. For example, in 1987, Yoshino et al. [19] proposed a system of classification based on the following morphological characteristics: area size, bilateral asymmetry, superiority of area size, outline of superior borders, partial septa and supra-orbital cells were collected and classified with code numbers. The authors state that the possibility of having the same code for two different individuals is one every 23,040 cases.
In 2005, to improve the performance of the above method for individual identification, Cameriere et al. [34] proposed a new system of classification based on the following morphological characteristics: ratio between left frontal sinus area and left orbital area (SOR1) and ratio between right frontal sinus area and right orbital area (SOR2), instead of the area size and bilateral asymmetry of Yoshino’s method. Cameriere et al. [24] also attempted to estimate the probability of misclassification.
With the above methods, the probability of making a positive identification error (i.e. the probability of identifying two images of two different skulls as belonging to the same person) was found to be 1/20,000 by Yoshino et al. [19] and p < 10–6 by Cameriere et al. [24].
The aim of the present study was to develop a reproducible technique and measurements from 3D reconstructions obtained with CBCT, for human identification purposes.
Materials and methods
CBCT scans of 150 patients (91 female, 59 male), aged between 15 and 78 years, were selected from those treated at the Unit of Orthodontics and Pediatric Dentistry, University of Milan (Italy).
All these examinations were performed with the same CBCT unit: i-CAT (Imaging Sciences International, Hatfield, PA) and the same settings: 120 kV and 20 mA. The scanning protocol involved 0.4-mm slice thickness, 16 × 22 cm field of view, 20-second scan time and 0.4 mm voxel size.
Inclusion criteria were as follows: patients had at least one frontal sinus; they were at least 15-years old; they had had i-CAT (Imaging Sciences International, Hatfield, PA, USA) CBCT scans previously, for planned orthodontic treatment; and their sinuses were not inflamed and not involved in any systemic disease.
The raw data were saved in DICOM format and then imported into the specific software program MIMICS 11.11 (Materialise N.V., Leuven, Belgium). Reconstruction of the coronal (x–z), sagittal (y–z) and transversal (x–y) planes were analysed.
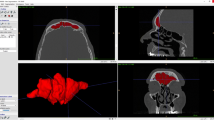
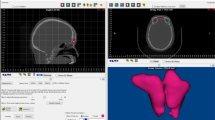
According to the minimal and maximal threshold values, one layer of the relevant structures (airways) was called the mask, and was defined and colour-coded. Air has the lowest values of HU (Hounsfield Unit) and while bone has the highest. Threshold levels for air were therefore determined for all CBCT datasets, in this case HU from −1024 to −20. Because of the connection of the air to the surroundings, pixel need to be erased with mask editing so the field of view can be excluded from the surroundings. When all the connections are broken, new pixels are added inside the volume for the whole volume to be measured. When the sinus is air filled, the only procedure needed is selecting the mask by thresholding air and then use the tool dilate for 2–3 pixels (Fig. 1a, b).

a, b Coronal (frontal) and mid-sagittal (lateral) views during the isolation of the frontal sinus (evidenced in yellow). The coronal section (a) is approximately at the premolar level. Mid-sagittal section (b) is best for the evaluation of the visible portion of the airway. This section can be generated with simple functions using the CBCT scanner’s software applications
Its corresponding 3D volume was then generated through the voxel size and number of voxels in the 3D object (Fig. 2). The contour interpolation algorithm is used to visualize the 3D model of the frontal sinus and the grey interpolation algorithm to calculate and measure the sinus volume.

3D volume rendering of the frontal sinus
On the basis of this reconstruction, maximal dimensions along 3 directions (x, y, z), X M, Y M, Z M (in mm), total volume area (in mm3), V t, and total surface (in mm2), S t, were calculated on the whole structure of the frontal sinuses.
The line drawn parallel to the Frankfort horizontal plane and passing through the tightest area of the sinus before its connection with the nose and the lower airway was chosen as the baseline of the sinus (Fig. 1) as a reference limit, in order to determine the whole volume of the sinuses which sometimes could not be significantly isolated if the baseline was drawn in an area above. All nonmetric characteristics and metric measurements were recorded after the frontal sinus was cut from the baseline. This choice is also one which may cause operators to make minor but statistically insignificant differences when volume sizes are measured.
Protocols to collect CBCT images for human subjects were approved by the Ethics Committee for Research Involving Human Subjects of the University of Milan (Italy), and the study was conducted in accordance with the ethical standards laid down by the Declaration of Helsinki (Finland). The World Medical Association (WMA) developed the Declaration of Helsinki as a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data.
To test intra-observer reliability, a random sample of 30 CBCT scans were each re-examined twice, at two-week intervals. Assessment of inter-observer reliability was carried out by two observers, each of whom evaluated 30 randomly selected CBCT scans.
Randomly selected means that each scan among the analysed CBCT has an equal and independent chance of being selected to belong to the sample of 30 CBCT scans used to test reliability of the method. Effectively, the function “sample” of the statistical environment R has been used to take a sample of 30 scans from 150 numbered CBCT.
Intra- and inter-observer reliability was studied with the intra-class correlation coefficient (ICC) [35, 36].
Statistical analysis
In this preliminary study, only the quantitative variables characterizing 3D frontal sinus patterns were analysed. Descriptive statistics were performed for variables X M, Y M, Z M, V t and S t. In particular, correlation analysis was carried out among all these variables, to find the least correlated ones, i.e. those with correlation coefficient r such that |r| < 0.9.
Six quantitative variables (parameters) measured have been taken for each skull: maximal dimensions of sinuses along 3 directions (x, y, z), X M, Y M, Z M (in mm), total volume area (in mm3), V t, and total surface (in mm2), S t, of the whole structure of the frontal sinuses. If two of these variables were strongly correlated, the information acquired considering one of them should not differ from that acquired using both variables. For example, in this study, a simple linear regression between the logarithm of S t and the logarithm of V t points out that 97 % of the variability of S t can be explained by the variability of V t (Fig. 3). Consequently, it is not useful for the identification process to consider both variables. The choice to include V t and to remove S t is related to the variability among subjects of V t which is greater than the variability of S t.

Simple linear regression between the logarithm of S t and the logarithm of V t
Once the variables considered for individual identification by frontal sinus had been selected, the re-examined CBCT scans were used to assess the intra-observer variability of the chosen statistical variables. Within-subject variability was characterized by assuming that it was only due to errors on repeated measurements of the same scan, and that these errors were normally distributed.
The tolerance region at level 1−α for each individual was then evaluated. This region consists of measurement vectors x satisfying:
where x is a k-dimensional vector of measurements of a 3D frontal sinus pattern chosen for identification, μ is the known k-dimensional vector of measurements of a 3D frontal sinus pattern in the given individual and \( \sum \) is the estimated covariance matrix associated with within-subject variability due to inter-observer error measurement. Lastly, \( \chi_{k}^{2} (1 - \alpha ) \) indicates the quantile function for probability 1−α of the Chi squared distribution, with k degrees of freedom. That is, if a k-dimensional vector of measurement of a 3D frontal sinus pattern, x, is located out of the region of tolerance with centre μ, it does not refer to the same individual characterized by μ, with a probability of a false-negative error of less than α.
Calculation of probability of individual identification
In order to estimate the tolerance region at level (1−α) = 95 %, the re-examined observations (30 subjects) were used to determine inter-observer variability by assessing the covariance matrix:
Entering covariance matrix (2) in inequality (1) yielded the tolerance region at level 95 %. For example, if we know that a subject has X M = 49.89 mm, Y M = 25.74 mm, Z M = 33.60 mm and V t = 9011.95 mm3, then the centre of tolerance region for that subject is μ = (49.89, 25.74, 33.60, 9011.95).
Subsequently, another CBCT scan of the frontal sinuses of an unknown subject was compared with the following measures: X M = 50.89 mm, Y M = 26.74 mm, Z M = 34.60 mm and V t = 9111.95 mm3. The question for identification was “Does the second CBCT scan belong to the same subject?” According to inequality (1), since the first term \( (x - \mu )^{\prime } \sum^{ - 1} (x - \mu ) = 15.06 \) is not less than the second term \( \chi_{k}^{2} (1 - \alpha ) = 9.49 \), the second CBCT scan does not belong to the tolerance region of the same subject. This means that the second subject is different from the first one, with a probability α = 5 % of erroneously rejecting the hypothesis that the two scans belong to the same subject. The distribution of the logarithm of the Mahalanobis distance among the 150 scans is shown in Fig. 4.

Distribution of the logarithm of the Mahalanobis distance among the 150 skulls
Results
Frontal sinuses were separate in 21 subjects (14 %), fused in 67 (44.6 %) and found on only one side (unilateral) in 9 (6 %). A prominent middle of fused sinus (PMS) was found in 53 subjects (35.3 %) (Table 1).
Correlation analysis (Table 2) showed that sinus surfaces were strongly correlated with their volume (r = 0.976). Consequently, S t was excluded from the variables used in the identification procedure, because it carried a very small amount of information with respect to that obtained from the other four variables. Hence, each subject was identified according to the four variables X M, Y M, Z M and V t.
As regards the intra-observer variability of X M, Y M, Z M and V t measurements, ICC ranged between 0.963 and 0.999. Regarding the inter-observer variability of the same measurements, ICC ranged from 0.973 to 0.999, and did not reveal significant intra- or inter-observer effects, indicating substantial homogeneity of evaluation.
Discussion
In recent years, the increase and improvements in 3D radiographic techniques (MRI and CT) have generated so many data that they can also be used for identification purposes. Compared with traditional 2D techniques, 3D images yield far more information. In addition to data from the coronal plane with traditional X-rays, CBCT scanning allows assessment of sinus depth, area and volume. In the last few years, self-shielded CBCT machines have also reduced radiation, compared with multi-slice CT (MSCT) scanning and conventional radiography; its relative low cost make acquisition more feasible; it can be also used in a wider range of subjects, and easily transported and operated for either office or mobile morgues [37, 38]. Lastly, the CBCT machines are user-friendly and limited training is necessary to use them. Although CBCT has not yet gained wide acceptance in forensic community, Sarment and Christensen encourage its use for many forensic applications [33].
In this study, frontal sinuses were separate in 21 subjects (14 %), fused in 67 (44.6 %) and found on only one side (unilateral) in 9 (6 % total, 2.6 % in females and 3.4 % in males). A PMS was found in 53 subjects (35.3 %, 11.3 in males and 24.6 in females). Because the left and right frontal sinuses develop independently, a significant asymmetry between these sinuses can arise in the same individual [39]. Occasionally, one or both sinuses may be absent. Yoshino et al. [19] reported the frequency of a unilateral sinus absence as 13.3 % for males and 16.9 % in females. The frequency of frontal sinus agenesis is variable between different populations [40].
The term fused sinus is used here to describe adjoining of the right and left sinuses [19]. Prominent middle sinus was defined as the attachment of both sinuses: one sinus overdeveloped, with the middle of the fused sinus protruding [19]. The fused and prominent middle sinuses were the highest types in this study. In Yoshino et al. [19], the frequency of the fused and prominent middle sinus was 53 % in males and 34 % in females. In Lee et al. [41], the frequency was 66.9 % in males and 60.2 % in females. Although the fused and prominent middle sinuses were not mentioned in previous studies, their importance should be taken into account when the frontal sinus is classified by morphology.
Concerning the intra- and inter-observer variability, ICC ranged between 0.963 and 0.999 and between 0.973 and 0.999, respectively. These results showed a strong agreement for the same reader and also between different operators with high accuracy. The high agreement renders frontal sinus identification system to be a simple method for establishing the identification of unknown persons for whom frontal sinus X-rays exist.
Of the variables considered for identification purposes, total surface (S t) was not used in this study because it is highly correlated with volume (r = 0.976) and therefore does not increase the quantity of identifying information.
Each CBCT scan corresponds to a point, P, in the four-dimensional space identified by X M, Y M, Z M and V t. Measured distances are quantitative characteristics and may vary, depending on manual reconstruction of the images, so it was concluded that one and the same skull always show an identical value for a certain measured parameter. Consequently, for identification purposes, the variability of CBCT measurements was considered and assessed in the frontal sinuses of the same subject. In this respect, one of the main aims of this paper was to evaluate, in each individual, the tolerance region, i.e. the 4D region T, where each point corresponds to the same subject. Conversely, a point which does not belong to this region represents a different subject, with a small fixed probability, α, of yielding a false-negative error.
As regards the probability of obtaining a positive identification error, i.e. two different subjects belong to the same tolerance region, none of the 150 individuals in this sample fell in the tolerance region of another individual.
Conclusions
The technique described in this study could increase the usefulness of the frontal sinus identification method in new forms of 3D examinations such as CBCT. The comparison of frontal sinus images by CBCT can be used as an additional method in the identification process, providing the expert with greater reliability. Forensic researchers are expected to achieve more numerous identifications in the future by applying CBCT scanning.
References
David MP, Saxena R (2010) Use of frontal sinus and nasal septum patterns as an aid in personal identification: a digital radiographic pilot study. J Forensic Dent Sci 2:77–80
Kanchan T, Krishan K, Menezes RG, Suresh Kumar Shetty B, Lobo SW (2010) Frontal sinus radiographs-a useful means of identification. J Forensic Leg Med 17:223–224
Tatlisumak E, Asirdizer M, Sunay Yavuz M (2011) Usability of CT Images of frontal sinus in forensic personal identification. In: Homma N (ed) Theory and applications of CT imaging and analysis. InTech, Rijeka, pp 257–268
Abraham J, Champod C, Lennard C, Roux C (2013) Spatial analysis of corresponding fingerprint features from match and close non-match populations. Forensic Sci Int 230(1–3):87–98
Schuliar Y, Knudsen PJ (2012) Role of forensic pathologists in mass disasters. Forensic Sci Med Pathol 8:164–173
Schwark T, Heinrich A, Von Wurmb-Schwark N (2011) Genetic identification of highly putrefied bodies using DNA from soft tissues. Int J Legal Med 125:891–894
Rios L, García-Rubio A, Martínez B, Alonso A, Puente J (2012) Identification process in mass graves from the Spanish Civil War II. Forensic Sci Int 219:e4–e9
Ishii M, Yayama K, Motani H, Sakuma A, Yasjima D, Hayakawa M, Yamamoto S, Iwase H (2011) Application of superimposition-based personal identification using skull computed tomography images. J Forensic Sci 56:960–966
Berketa JW (2014) Maximizing postmortem oral-facial data to assist identification following severe incineration. Forensic Sci Med Path 10(2):208–216
Patil N, Karjodkar FR, Sontakke S, Sansare K, Salvi R (2012) Uniqueness of radiographic patterns of the frontal sinus for personal identification. Imaging Sci Den 42:213–217
McLaughlin RB Jr, Rehl RM, Lanza DC (2001) Clinically relevant frontal sinus anatomy and physiology. Otolaryng Clin N Am 34:1–22
Seiden AM (2005) Frontal headache. In: Kountakis SE, Senior BA, Draf W (eds) The frontal sinus. Springer, Berlin, pp 115–126
Allen BC (1961) Applied anatomy of paranasal sinuses. J Am Osteopath Assoc 60:978
Kirk NJ, Wood RE, Goldstein M (2002) Skeletal identification using the frontal sinus region: a retrospective study of 39 cases. J Forensic Sci 47:318–323
Cox M, Malcolm M, Fairgrieve SI (2009) A new digital method for the objective comparison of frontal sinuses for identification. J Forensic Sci 54:761–772
Nambiar P, Naidu MD, Subramaniam K (1999) Anatomical variability of the frontal sinuses and their application in forensic identification. Clin Anat 12:16–19
Wallis A, Donal PJ (1988) Frontal sinus fractures: a review of 72 cases. Laryngoscope 98:593–598
Quatrehomme G, Fronty P, Sapanet M, Grévin G, Bailet P, Ollier A (1996) Identification by frontal sinus pattern in forensic anthropology. Forensic Sci Int 83:147–153
Yoshino M, Miyasaka S, Sato H, Seta S (1987) Classification system of frontal sinus patterns by radiography. Its application to identification of unknown skeletal remains. Forensic Sci Int 34:289–299
Christensen AM (2004) The impact of Daubert: implications for testimony and research in forensic anthropology (and the use of frontal sinuses in personal identification). J Forensic Sci 49(3):1–4
Campobasso CP, Dell’erba AS, Belviso M, Di Vella G (2007) Craniofacial identification by comparison of antemortem and postmortem radiographs: two case reports dealing with burnt bodies. Am J Forensic Med Pathol 2:182–186
Ribeiro Fde A (2000) Standardized measurements of radiographic films of the frontal sinuses: an aid to identifying unknown persons. Ear Nose Throat J 79:26–33
Tatlisumak E, Ovali GY, Aslan A, Asirdizer M, Zeyfeoglu Y, Tarhan S (2007) Identification of unknown bodies by using CT images of frontal sinus. Forensic Sci Int 166:42–48
Cameriere R, Ferrante L, Molleson T, Brown B (2008) Frontal sinus accuracy in identification as measured by false positives in kin groups. J Forensic Sci 53:1280–1282
Christensen AM (2005) Assessing the variation in individual frontal sinus outlines. Am J Phys Anthropol 127:291–295
Kim DI, Lee UY, Park SO, Kwak DS, Han SH (2012) Identification using frontal sinus by three-dimensional reconstruction from computed tomography. J Forensic Sci 58(19):5–12
Jackowski C, Wyss M, Persson A, Classens M, Thali MJ, Lussi A (2008) Ultra-high-resolution dual-source CT for forensic dental visualization-discrimination of ceramic and composite fillings. Int J Legal Med 122(43):301–307
Carvalho SPM, Alves da Silva RH, Lopes-Júnior C, Peres AS (2009) Use of images for human identification in forensic dentistry. Radiol Bras 42(2):125–130
Uthman AT, Al-Rawi NH, Al-Naaimi AS, Tawfeeq AS, Suhail EH (2010) Evaluation of frontal sinus and skull measurements using spiral CT scanning: an aid in unknown person identification. Forensic Sci Int 197(124):e1–e7
Cappabianca S, Perillo L, Esposito V, Iaselli F, Tufano G, Thanassoulas TG et al (2013) A computed tomography-based comparative cephalometric analysis of the Italian craniofacial pattern through 2,700 years. Radiol Med 118(2):276–290
Reichs KJ (1993) Quantified comparison of frontal sinus patterns by means of computed tomography. Forensic Sci Int 61:141–168
Miracle AC, Mukherji SK (2009) Cone-beam CT of the head and neck, Part 2: clinical applications. Am J Neuroradiol 30:1285–1292
Sarment D, Christensen AM (2014) The use of cone beam computed tomography in forensic radiology. J Forensic Rad Imag 2(4):173–181
Cameriere R, Ferrante L, Mirtella D, Rollo FU, Cingolani M (2005) Frontal sinuses for identification: quality of classifications, possible error and potential corrections. J Forensic Sci 50(4):770–773
Ferrante L, Cameriere R (2009) Statistical methods to assess the reliability of measurements in the procedures for forensic age estimation. Int J Legal Med 123:277–283
Shrout PE, Fleiss JL (1979) Intra-class correlations: uses in assessing rater reliability. Psychol Bull 2:420–428
Kapila S, Conley RS, Harrell WE Jr (2011) The current status of cone beam computed tomography imaging in orthodontics. Dentomaxillofac Rad 40:24–34
Besana JL, Rogers TL (2010) Personal identification using the frontal sinus. J Forensic Sci 55:584–589
Levine HL, Clemente MP (2003) Surgical anatomy of the paranasal sinus. In: Clemente MP (ed) Sinus surgery: endoscopic and microscopic approaches. Thierne, Stuttgart, pp 1–55
Shah RK, Dhingra JK, Carter BL, Rebeiz EE (2003) Paranasal sinus development: a radiographic study. Laryngoscope 113:205–209
Lee HK, Kwon KH, Kim KJ, Kang SM, Moon GJ (1985) A study on the classification of frontal sinuses and distributions using simple AP skull radiographies. J Soonchunhyang Univ 8(4):481–485
Acknowledgments
The authors would like to thank the staff of the Unit of Orthodontics and Pediatric Dentistry, University of Milan (Italy) for their assistance on this project, and also Ms. Gabriel Walton for editing the English text. Thanks also to the editor and the reviewers for helpful comments that have improved this paper.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cossellu, G., De Luca, S., Biagi, R. et al. Reliability of frontal sinus by cone beam-computed tomography (CBCT) for individual identification. Radiol med 120, 1130–1136 (2015). https://doi.org/10.1007/s11547-015-0552-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-015-0552-y