
Abstract
Female sex workers are a structurally vulnerable population, including critical insecurity such as having access to food and shelter. This risk may be heightened among individuals who enter sex work as minors. However, the reasons for entering sex work as a minor and the long-term structural risk implications are poorly understood. Here, we investigated the reasons for and long-term impact of trading sex before the age of eighteen on women’s structural vulnerability among a cohort of 250 cisgender women involved in street-based sex work in Baltimore City, Maryland, USA. We used logistic regression to explore the role of age of entry on two structural vulnerability outcomes of interest (homelessness and recent food insecurity in the past 3 months). Overall, 73% of women entered the sex trade to get drugs, 36% of women entered to get basic necessities such as food or housing, and 17% of women entered to support their children or family. Of significance, 21% of those aged < 18 years at entry reported being either coerced, threatened, pressured, misled, tricked, or physically forced into trading sex compared to 5% in those who entered at an older age group (p value < 0.001). In adjusted analysis, women who first trade sex before the age of 18 had 4.54 increased odds of experiencing recent homelessness (95% CI 1.92–10.70) and had 3.14 times increased odds of experiencing recent food insecurity (95% CI 1.42–6.94). Those who entered as minors were also more likely to be HIV positive (11.3% vs 3.6%, p value = 0.02). This study highlights that those who trade sex at a younger age experience an ongoing cumulative vulnerability in comparison to those entering over the age of 18. These findings call for additional research into a more detailed understanding of young women’s entry into the sex trade and trajectory. A focus on the importance of policy changes and structural interventions that directly alleviate young people’s socio-economic disadvantage is needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Globally and in the US, cisgender women who engage in sex work, hereafter female sex workers (FSW) represent a high-risk group for the acquisition of sexually transmitted infections [1]. Additionally, FSW are frequently the victims of human rights abuses including both physical and sexual violence [2]. Increasingly ecological and risk environment models [3, 4] are being used to help better understand the role of a complex array of social and structural determinants in shaping FSWs’ health risks and outcomes. FSW are not a homogenous group as their behaviors (e.g., engagement in drug use, engagement in survival sex, sex for basic needs) and the settings in which they work (e.g., street-based, working in brothels or clubs) vary greatly. A particularly vulnerable group are women who trade sex before the age of 18. According to the Trafficking Victims Protection Act (TVPA) [5], any person under the age of 18 who is trading or selling sex is considered a victim of trafficking. The TVPA stipulates that minors meet criteria for trafficking solely based on age without presence of force, fraud, or coercion nor movement across state lines. Throughout this paper, the term “trade sex” will be used to account for girls under 18 and involved in sex work. This term recognizes the heterogeneity of this group of young people and their experiences [6]. Several individual and interpersonal factors associated with HIV risk have been found to be higher among FSW who trade sex prior to the age of 18. These include higher levels of HIV infection and sexual risk behaviors (e.g., less frequent condom use, recent anal sex), lower levels of HIV awareness, more sexual partners, and increased risk of experiencing violence [7,8,9].
Following a structural determinants approach to understanding health outcomes, a variety of dimensions contextualize FSWs’ HIV risk and acquisition. Consideration must be given to the complex interaction of individual (e.g., condom/drug use), interpersonal (e.g., experience of violence, number of clients), and structural-level factors (e.g., stigma, poverty, lack of social capital) [10]. Often, HIV-related structural vulnerabilities predate and may precipitate entry into the sex trade, for instance childhood sexual abuse, economic hardship, and drug use [11, 12]. Research has sought to explore the different motivations for entry into the sex trade with findings suggesting that age is an important organizing factor [13]. However, while the literature has identified several individual, interpersonal, and structural vulnerabilities influencing early initiation and explored the immediate impact of early entry on HIV risk, the long-term effects of entering the sex trade at a young age have received little attention. It remains unclear if these women are temporarily at increased risk of HIV during their younger years or whether entering at a young age is associated with long-term increases in risk, whereby they enter a subpopulation of extreme vulnerability without opportunities to exit. In support of the latter, a study of adult cisgender FSW in Chicago found an increased risk of health problems, including sexually transmitted diseases, among FSW who started trading sex prior to the age of eighteen [14]. Another study in Minneapolis found that women who had traded sex before age 18 and were still working as adults sold sex more frequently and reported more street-based work than those who started after the age of 18 [15]. While these two studies provide an evidence base of age of entry being a key marker of proximal factors linked to HIV risk, they have not considered the wider structural environment within which these women operate. Most fundamentally, we need to understand the extent to which these vulnerable populations can access basic necessities such as food and shelter. It is these broader structural factors that provide the context in which lower order interpersonal and individual HIV risk taking occurs [4].
Structural vulnerability is an important explanatory framework that can help articulate how young persons’ positionality in a hierarchical social order characterized by intermediate factors of social and economic disadvantage (e.g., policies around affordable housing, local economic conditions related to employment opportunities) can translate into micro-level individual level hardship including homelessness and food insecurity, which in turn shape more proximal HIV-risk factors (e.g., unprotected sex, multiple high-risk partners) [16]. Although less is known about the food insecurity of young people who trade sex, studies show that adolescents who have reported trading sex are more likely to report histories of homelessness [17]. A nascent body of literature has directly investigated the relationship between food insecurity and homelessness among key vulnerable populations, including FSW and people who inject drugs (PWID). Two studies in Canada with PWID found that participants who reported food insecurity were at an increased odds of sharing injection equipment [18] and increased risk of engaging in unprotected sex [19]. The only study to have looked at food insecurity amongst FSW in a high-income setting (Canada) found that food insecurity was associated with both lifetime and recent experiences of physical/sexual violence [20]. Another study in Canada among FSW found that sexual violence was independently associated with sleeping on the street [21]. These studies reinforce the direct importance of overlapping indicators of structural vulnerability on marginalized groups more proximal HIV risk. However, how such structural vulnerability endures over time in the lives of marginalized women who trade sex at a young age is unexplored.
In this study, we looked at reasons for and long-term impact of trading sex before the age of eighteen among a cohort of 250 cisgender women involved in street-based sex work. The population was divided into those who entered the sex trade before the age of 18 versus over the age of 18. Adopting a life course perspective [22], our analysis focuses on how the interconnected structural conditions of specific structural factors, food insecurity, and homelessness manifest in the present day lives of those who traded sex under 18 years of age versus later in life, in addition to exploring the relationship of homelessness and food insecurity to FSWs’ current HIV-risk behaviors. A life course perspective provides a useful theory as it places individual behaviors and outcomes within a complex system that involves both their environment and time [23, 24]. The study is intended to direct policy and programming towards key socio-structural determinants in the lives of young women that may alleviate longer-term social and health-related vulnerability.
Methods
Study Population
Data were derived from the Sex Workers and Police Promoting Health in Risky Environments (SAPPHIRE) study, a prospective FSW cohort recruited in Baltimore City, Maryland, USA, that has been described in detail previously [25]. Briefly, street-based FSW were recruited through targeted sampling, with study staff approaching potential study participants in identified hotspots. Eligibility criteria were (1) age ≥ 15 years; (2) sold or traded oral, vaginal, or anal sex “for money or things like food, drugs or favors”; (3) picked up clients on the street or at public places ≥ 3 times in the past 3 months; and (4) willing to undergo HIV and STI testing. Exclusion criterion was identifying as male or a man. In addition to the baseline survey, shorter follow-up surveys and additional testing were conducted with participants during 4 field visits (3-, 6-, 9-, 12-month). The current analysis includes all baseline participants (n = 250), who were recruited between 04/2016 and 01/2017.
Participants completed a 50-min interviewer-led computer-assisted personal interview (CAPI) on topics covering demographics, history of sex work, including the age at which they first entered sex work, personal violence history, drug use and sexual behaviors, health services access, and mental health. In addition to the survey, biological specimens were collected for HIV and STI testing. HIV testing was completed using OraQuick© Advanced Rapid HIV-1/2 test kit (Orasure Technologies, Bethlehem, PA, USA). Results were given at the end of the interview along with the opportunity to receive referrals to a range of local health and social service organizations. For the STI testing, participants collected specimens using self-administered vaginal swabs (Aptima Multitest Swab Specimen Collection kit, Hologic, Inc., San Diego, CA, USA), which were tested for gonorrhea, chlamydia, and trichomoniasis. Positive results were sent to the Baltimore City Health Department for follow-up. Participants received a $70 prepaid VISA gift card for completion of the baseline visit. All procedures were approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
Measures
The two supporting structural factors we explored were homelessness and food insecurity experienced in the previous three months. These were chosen over other structural vulnerability factors measured due to their dual salience as independent health indicators as well as HIV-risk factors. Homelessness was self-reported and ascertained via the question, “have you been homeless in the past 3 months?” and for food insecurity, participants were asked how often they went to bed hungry because there was not enough food in the past 3 months, which we operationalized as going to bed hungry at least once per week.
We considered several demographic measures. Age and age first sold sex, street-based or otherwise, were retained as continuous covariates and were measured in years. Time since initiated sex work was generated from subtracting age first sold sex from current age and was analyzed as a continuous measure in years. Race/ethnicity is presented trichotomously as non-Hispanic White, non-Hispanic Black, or other race/ethnicity and was analyzed as dichotomously (White vs other) due to small sample size. We also explored relationship status (single vs married vs in a relationship) and childhood abuse, which was defined as ever being pressured or forced into sexual intercourse or sexual touching, or being hit, punched, slapped, or otherwise physically hurt by someone causing marks or physical injury under age 18. We considered other structural vulnerabilities: limited education (not graduating high school vs. graduating high school or obtaining GED), current unemployment, no monthly savings in the past 3 months, ever been arrested, and healthcare access measured by insurance status, no doctor visit in past 12 months, and visit to the emergency department in past 3 months.
We explored the reasons for entering the sex trade as well as reasons for current involvement. Women were asked how or why they entered the sex trade with 12 select-all-that-apply options including an open response category. Using a validated approach [26], we used these response options to create a category to include those who experienced being coerced, threatened, pressured, misled, tricked, or physically forced as one of the reasons for initially entering the sex trade. Women were also asked to select the option that best describes their relationship with the individual who introduced them to sex work with 11 choices including an open response choice. “Reasons for current engagement” were ascertained with 10 select-all-that-apply options including an open response option.
To explore whether homelessness and food insecurity are linked to more proximal drivers of HIV risk, we additionally measured STI infection in the past 3 months, inconsistent condom use in the past 3 months, > 30 clients in the past 3 months, and daily heroin use in the past 3 months. STI results were defined as positive or negative for each STI type, and indeterminate or inconclusive results were coded as missing. Inconsistent condom use was restricted to sex, either vaginal or anal, with clients in the past 3 months. Women were asked how often they used condoms with clients in the past 3 months with options always, most of the time, sometimes, rarely, and never, which we coded women as engaging in inconsistent condom use in the past 3 months if they reported using condoms with clients less often than always. Clients were defined as “people you’ve had vaginal, anal, or oral sex with for money, food, drugs, or favors.” Sexual violence was defined as being pressured or forced into sexual intercourse, and physical violence was defined as being hit, punched, slapped, or otherwise physically hurt, or being threatened or hurt with a weapon. We chose the cutoff of 30 clients as it was the median number of clients reported in the last 3 months at baseline.
Statistical Analysis
The attributes of women who traded sex before the age of 18 and after the age of 18 were compared across domains of demographics indicators, working conditions, drug use, and sexual risk behavior covariates using Pearson’s chi-square tests and t tests. Alongside age of entry, a priori list of variables were considered based on existing understanding of women’s risk environment, which included daily heroin use, race/ethnicity, and time since initiating sex work [27, 28]. We used logistic regression to explore the role of age of entry on of our two structural vulnerability outcomes of interest (recent homelessness and recent food insecurity). Initially a bivariate logistic regression model was used to evaluate the associations. We then developed multivariable logistic regressions that allowed us to adjust for possible measured confounders. Statistical analyses were conducted using Stata/SE 15.1 (StataCorp, College Station, TX, USA).
Results
The sample had a mean age of 35.7 years (range 18–61 years) (Table 1). Close to half (47.6%) of the women reported finishing high school or obtaining a GED. Substance use over the past 3 months was common with 70.8% reported injecting drugs in the past 3 months, 92.1% of whom had injected heroin in the past 3 months. 83.6% reported having smoked crack cocaine in the past 3 months. HIV prevalence was 5.2%. Trichomoniasis was highly prevalent with 48.8% of women testing positive at the baseline visit. Overall, 62.4% of the women reporting being homeless within the last 3 months and 61.2% reported going hungry over the same period. The mean age of entry into the sex trade was 24.7 (range 11–61). 21.2% of women entered < 18 years, 39.2% entered between 18 and 25, and 39.6% entered at older age groups. Half of the women had experienced childhood abuse, either physical or sexual. However, women that entered < 18 were more likely to report sexual childhood abuse than those 18+ years at entry (45.3% vs 29.4%, p value 0.02). Individuals who entered as minors were also much more likely to be HIV positive (11.3% vs 3.6%, p value 0.02) as well as have suffered from recent homelessness (79.2% vs 57.9%, p value < 0.01) or food insecurity (77.4% vs 56.9%, p value 0.01).
Reasons for Entering the Sex Trade
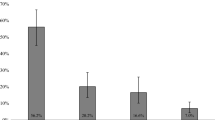
Overall, 73.2% of women entered the sex trade to get drugs, 35.6% of women entered to get basic necessities such as food or housing, and 17.2% of women entered to support their children or family (Table 2). Of significance, 20.8% of those aged < 18 years at entry reported being either coerced, threatened, pressured, misled, tricked, or physically forced into trading sex compared to 4.6% in those who entered at an older age group (p value < 0.001). Additionally, 28.3% of those aged < 18 years at age of entry reported earning extra spending money as a reason compared to 14.2% in those 18 years or older at entry (p value 0.02). The most cited relationship of the person that introduced them to the sex trade was a current sex worker that was not a family member (35.7%).
Current Working Environment and Reasons for Current Sex Trade
Overall, the mean time since initiating sex trade was 10.9 years (range 0–43 years) (Table 3). However, women who entered < 18 had been trading sex significantly longer than women that entered at 18 or older (18.2 years vs 9.0 years, p value 0.02). Most (66.0%) women reported daily sex trade, and in addition to having found clients on the street, women reported ever having found clients at a bar, restaurant, or club (37.1%); online (27.0%); and a strip club or exotic dance club (24.6%). The most common reasons for current sex work were to get drugs (86.0%), to get food (53.6%), and to get a place to stay (36.4%). There was no statistically significant difference between < 18 and those over 18 at entry for citing drugs as a reason for current sex work. However, women that entered < 18 were statistically significantly more likely to report “to get food” and “to get a place to stay” as reasons for current sex work (66.0% vs 50.3%, p value 0.04; 49.1% vs 33.0%, p value 0.03, respectively).
Structural-Level Outcomes—Food Insecurity and Experiencing Homelessness
We explored unadjusted and adjusted correlates of homelessness and separately for food insecurity by examining the relationship between the structural variable and age of entry into the sex trade. In unadjusted analyses, we found that those who entered < 18 had 2.78 times the odds of experiencing homelessness compared to those who entered later in life (95% CI 1.35–5.72) (Table 4). Drug use was also important; those who reported daily heroin use in the past 3 months had 3.86 (95% CI 2.19–6.80) times the odds of reporting recent homelessness compared to the rest of the cohort. Individuals who had been in the sex trade for longer reported less homelessness than those who more recently initiated trading sex, with each additional year associated with a 0.94 (95% CI 0.91–0.97) times change in odds. In adjusted logistic regression, these risk factors remained significant with age at entry (aOR 4.55, 95% CI 1.94–10.64), time since initiating trading sex (aOR 0.96, 95% CI 0.93–0.99), and daily heroin use (aOR 3.66, 95% CI 2.01–6.67) all independently associated with experiencing homelessness. In unadjusted analyses for experience of food insecurity in the past 3 months, women that entered the sex trade before the age of 18 had 2.59 times the odds of food insecurity than women that entered at or above age 18 (95% CI 1.28–5.23). Experiencing food insecurity was also correlated with current age (OR 0.97, 95% CI 0.94–0.99) and daily heroin use in the past 3 months (OR 1.87, 95% CI 1.08–3.23). In the adjusted analysis, age of entry remained significantly associated with food insecurity (aOR 3.32, 95% CI 1.52–7.28).
Structural Determinants Relationship to HIV-Risk Factors
We further explored how homelessness and food insecurity are related to contemporaneous HIV-risk factors. Individuals who reported recent homelessness had 1.83 times the odds of having an STI infection (95% CI 1.08–3.11) (Supplementary Table 1). This population also had an average of 43.5 more clients within the last 3 months (95% CI 8.0–72.7) compared to the rest of the FSW cohort population. The association of homelessness with client violence (OR 0.87, 95% CI 0.51–1.50) and reusing injection drug equipment (OR 1.79, 95% CI 0.94–3.41) was not significant. However, we found those who experienced recent food insecurity had 1.9 times the odds of experiencing client violence (95% CI 1.08–3.32). They also had an average of 21.7 more clients in the past 3 months, although this difference was not significant (95% CI − 11.4–54.7). In addition, those who experienced food insecurity had 2.44 times the odds of reusing injection drug equipment (95% CI 1.25–4.75). There was no association between food insecurity and STI infection (OR 1.25, 95% CI 0.74–2.10).
Discussion
In this study, we have used data from a cohort of FSW from Baltimore City, USA, to explore how age of entry into the sex trade is linked to subsequent risk of structural-level HIV-related outcomes in adulthood. We found evidence that women who first trade sex before the age of 18 appear to be more likely to experience homelessness and food insecurity with implications for their HIV-related risk and broader health and wellbeing. Overall, we found that those who entered sex work under the age of 18 had nearly three times the prevalence of being HIV positive as those who entered as adults.
This study documents instigating factors for FSWs’ involvement in street-based sex trade and corroborates existing literature that a variety of factors influence women’s entry both < 18 or over. While avoiding a simplistic narrative of FSW who entered before the age of 18 being forced into trading sex, it was notable that a fifth of all FSW who started as < 18 also experienced conditions of force, fraud, coercion, or deception at entry compared to 4.6% of those older at entry. These criteria together comprise the TVPA definition of trafficked individuals as those, “induced by force, fraud, or coercion, or in which the person induced to perform [a sex] act has not attained 18 years of age.” [5]. It should however be emphasized that most women in this cohort did not meet the criteria for being trafficked.
In addition, although the broader literature gives rise to an inconsistent picture regarding the association between childhood abuse and younger involvement in the sex trade [29,30,31], this study’s findings point to almost half of those who entered before the age of 18 reporting childhood sexual abuse compared to only close to a third amongst participants who entered the sex trade later. Although it is important to draw attention to abuse that may enable a young person’s involvement in the sex trade, other survival-related factors can also feature among the more proximal drivers behind the decision to enter [6, 32]. When asked about reasons for entering the sex trade, 49.6% of women who entered below the age of 18 reported the need for basic necessities, such as food and housing. Although a similar number reported the same reason in the ≥ 18 group, it is worth highlighting this broader context of material adversity that underage girls face alongside precipitating factors for entry, such as sexual abuse.
Drug use remained independently associated with both homelessness and food insecurity. While the majority of FSW who entered before the age of 18 did so to support a drug habit, it was equally as important a reason in older age groups, consistent with previous studies [6, 13]. These findings are indicative of a setting in which street-based sex trade is deeply interconnected with the street drug economy and highlights the importance of broader structural context to understanding reasons for involvement in sex work in different settings.
Importantly, our findings highlight the previously unexplored impact of early entry into trading sex on FSW’s long-term structural vulnerability. Homelessness and food insecurity represent critical structural determinants of health and are shown to have significant consequences for the wellbeing of the most vulnerable groups in our society. Research has documented the consequences for increased mortality and morbidities including poorer outcomes for both chronic and infectious disease as well as mental health [33, 34]. Those experiencing increased economic hardship and social marginalization are at greatest risk. Among FSW populations, the implications of food insecurity on women’s sexual health and HIV risk have been linked to multiple partners and increased reliance on intimate partners and clients alongside reduced capacity to negotiate condom use [16, 20]. HIV has been shown to disproportionately impact those experiencing homelessness with additional risk of being the victim of physical or sexual violence [35]. Findings in this study highlight the enduring and disproportionate burden of these two important and mutually reinforcing structural health determinants on FSW who enter the sex trade before the age of 18. Among our cohort of 250 FSW, those who entered before the age of 18 continue to be structurally vulnerable, with over two and a half times the odds of experiencing food insecurity and current homelessness than those who entered as adults. This finding suggests that the documented socio-economic vulnerabilities that often precipitate a young person’s involvement in the sex trade persist in ways that have not previously been understood. FSW in this study reported similar reasons for present engagement in trading sex, including to support a drug habit and provide basic necessities. However, the fact that those women who entered at a younger age continued to experience homelessness and food insecurity as they become older highlights the existence of a subpopulation who are experiencing an amplified context of structural vulnerability over time with real implications for their HIV risk and broader health.
Additionally, we found several recognized markers for sexual risk associated with recent homelessness—a higher number of clients in the last 3 months and increased risk of STI infection. Food insecurity was associated with recent client violence and reusing injection equipment. These findings are consistent with existing literature that highlights how both homelessness and food insecurity create a unique context of vulnerability that influences HIV-related risk taking and health outcomes amongst the most marginalized [21, 36]. Accordingly, our findings suggest that those who enter the sex trade at a young age remain disproportionately impacted by a physical and social context of homelessness and food insecurity with implications for their experience of violence, drug- and sexual-related risk taking alongside broader health and wellbeing. The fact that 11.3% (7 of 56) participants who entered sex work < 18 tested positive to HIV further indicates this group’s heightened HIV-risk context.
Research in other settings highlights homelessness can be a major driver for engagement in the sex trade is important in pushing the agenda on policies and programs that secure safe temporary and longer-term housing solutions for young people [6]. Our findings further support the urgency of this need given that these same youth go on to have amplified structural vulnerability as adults, both with respect to enduring housing instability and the introduction of food insecurity, which so often accompanies homelessness. Safer environment interventions at the macro-level must address women currently engaged in street-based sex trade. Interventions should include increasing the availability of and access to low-income housing and looking for systemic solutions to food insecurity that tackle the upstream drivers of urban poverty. At the micro-level, interventions that can more directly tackle FSWs’ immediate structural vulnerability and context of risk could include peer outreach strategies that link women to emergency and short-term housing options; food distribution hubs (including food pantries and kitchens); and mobile health and outreach services (including HIV testing, sterile syringes, free condoms, support for survivors of violence). These types of interventions are best supported by a macro-environment in which sex work is decriminalized. Decriminalization is particularly urgent considering current research highlighting the impact of criminalization on FSWs’ HIV risk including displacement from health outreach and HIV prevention services [37]. In addition to which, although the TVPA categorizes youth who trade sex as trafficking victims, in many states in the US, young people involved in the sex trade are still arrested and charged for prostitution, which is regulated at the state not federal level [6]. Criminalization can therefore have a very real impact on young persons involved in the sex trade, often funneling them into the criminal justice system that facilitates longer-term structural vulnerability. New Zealand decriminalized sex work in 2003 and is hailed as doing some of the most effective work on human trafficking [38], showing that decriminalization of sex work can offer protections to human rights and dignity in harmony with continued legal protections around human trafficking.
This study is not without its limitations. This analysis was cross-sectional, and as such, we are unable to establish temporality of events. Additionally, we lack understanding surrounding the participants’ first transactional sex encounter and the age at sexual debut. More information on both would better help elucidate the sequence of events leading to the first transactional sex encounter. Those that had been involved in the sex trade the longest could be susceptible to increased recall bias. Additionally, age when first sold sex may be subject to social desirability bias; participants may feel shame at reporting their sex work history. We attempted to lessen effects of responding based on social desirability by conducting interviews with only one trained study staff member in a private interview station. Participants were also reminded that their responses are confidential and not connected to their name. Although we treated food insecurity and homelessness as independent constructs, studies have shown a strong correlation between the two [39]; it would be useful to develop aggregate structural vulnerability measures to look at them in more detail. Finally, due to small sample size of women who entered as minors and unbalanced data, the CIs for homelessness and food insecurity are wide. However, despite this limitation, the lower end of the confidence intervals (1.92 and 1.42) represent a significant impact on homelessness and food insecurity, respectively, for women who enter sex work as a minor.
Conclusion
The failure to address many young women’s basic human rights, including housing, employment, access to education, and welfare, often catalyzes them into sex work and additional environments of risk and vulnerability [6]. This study highlights that those who trade sex at a younger age experience an ongoing cumulative vulnerability in comparison to those entering over the age of 18, with trading sex not alleviating young persons’ housing needs in the long-term and precipitating additional related structural vulnerabilities, namely food insecurity. These findings call for additional research into a more detailed understanding of why young women enter the sex trade and in particular, the individual-, interpersonal-, and structural-level factors that are present in their lives at that time. Research is also lacking on the trajectories of those who may enter the sex trade out of choice and the potentially cyclical nature of force/fraud/coercion in women’s longer-term involvement. Crucially, findings focus attention on the importance of policy changes and structural interventions that directly alleviate young people’s socio-economic disadvantage, which is so critical to the cessation of abiding long-term structural vulnerability and amplified HIV risk.
References
Baral S, Beyrer C, Muessig K, et al. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(7):538–49.
Decker MR, Crago A-L, Chu SKH, et al. Human rights violations against sex workers: burden and effect on HIV. Lancet. 2015;385(9963):186–99.
Rhodes T, Wagner K, Strathdee SA, Shannon K, Davidson P, Bourgois P. Structural violence and structural vulnerability within the risk environment: theoretical and methodological perspectives for a social epidemiology of HIV risk among injection drug users and sex workers. In: O’Campo P, Dunn JR, eds. Rethinking Social Epidemiology Springer Netherlands. 2012:205–30.
Shannon K, Strathdee SA, Goldenberg SM, et al. Global epidemiology of HIV among female sex workers: influence of structural determinants. Lancet. 2015;385(9962):55–71.
United States. Victims of Trafficking and Violence Protection Act of 2000.; (Public Law 106-386/HR 3244/114 Stat. 1482, October 2000).
Lutnick A. Domestic minor sex trafficking: beyond victims and villains. Columbia University Press; 2016. New York, Chichester West Sussex
Silverman JG, Servin A, Goldenberg SM, et al. Sexual violence and HIV infection associated with adolescent vs adult entry into the sex trade in Mexico. JAMA. 2015;314(5):516. https://doi.org/10.1001/jama.2015.7376.
Goldenberg SM, Chettiar J, Simo A, et al. Early sex work initiation independently elevates odds of HIV infection and police arrest among adult sex workers in a Canadian setting. J Acquir Immune Defic Syndr. 2014;65(1):122–8.
Salazar M, Brouwer KC, Rocha-Jimenez T, Boyce SC, Staines-Orozco H, Silverman JG. Substance use among female sex workers in two US-Mexico border cities: associations with age of entry. Subst Use Misuse. 2018:1–4.
Shannon K, Goldenberg SM, Deering KN, Strathdee SA. HIV infection among female sex workers in concentrated and high prevalence epidemics: why a structural determinants framework is needed. Curr Opin HIV AIDS. 2014;9(2):174–82.
Loza O, Strathdee SA, Lozada R, et al. Correlates of early versus later initiation into sex work in two Mexico–US border cities. J Adolesc Health Care. 2010;46(1):37–44.
Kramer LA, Berg EC. A survival analysis of timing of entry into prostitution: the differential impact of race, educational level, and childhood/adolescent risk factors. Sociol Inq. 2003;73(4):511–28.
Cobbina JE, Oselin SS. It’s not only for the money: an analysis of adolescent versus adult entry into street prostitution. Sociol Inq. 2011;81(3):310–32.
Raphael J, Shapiro D. Sisters speak out: the lives and needs of prostituted women in Chicago: research study. Center for Impact Research; 2002. Chicago, IL
Martin L, Hearst MO, Widome R. Meaningful differences: comparison of adult women who first traded sex as a juvenile versus as an adult. Violence Against Women. 2010;16(11):1252–69.
Vogenthaler NS, Kushel MB, Hadley C, et al. Food insecurity and risky sexual behaviors among homeless and marginally housed HIV-infected individuals in San Francisco. AIDS Behav. 2013;17(5):1688–93.
Yates GL, Mackenzie RG, Pennbridge J, Swofford A. A risk profile comparison of homeless youth involved in prostitution and homeless youth not involved. J Adolesc Health. 1991;12(7):545–8.
Strike C, Rudzinski K, Patterson J, Millson M. Frequent food insecurity among injection drug users: correlates and concerns. BMC Public Health. 2012;12:1058.
Shannon K, Kerr T, Milloy M-J, et al. Severe food insecurity is associated with elevated unprotected sex among HIV-seropositive injection drug users independent of HAART use. AIDS. 2011;25(16):2037–42.
Barreto D, Shoveller J, Braschel M, Duff P, Shannon K. The effect of violence and intersecting structural inequities on high rates of food insecurity among marginalized sex workers in a Canadian setting. J Urban Health. 2018; https://doi.org/10.1007/s11524-018-0281-3.
Duff P, Deering K, Gibson K, Tyndall M, Shannon K. Homelessness among a cohort of women in street-based sex work: the need for safer environment interventions. BMC Public Health. 2011;11:643.
Elder GH. Time, human agency, and social change: perspectives on the life course. Soc Psychol Q. 1994;57(1):4–15.
Campbell R, Dworkin E, Cabral G. An ecological model of the impact of sexual assault on women’s mental health. Trauma Violence Abuse. 2009;10(3):225–46.
Bronfenbrenner U. The ecology of human development. Harvard University Press; 1979. Cambridge, MA
Allen ST, Footer KHA, Galai N, Park JN, Silberzahn B, Sherman SG. Implementing targeted sampling: lessons learned from recruiting female sex workers in Baltimore, MD. J Urban Health. 2018; https://doi.org/10.1007/s11524-018-0292-0.
Decker MR, McCauley HL, Phuengsamran D, Janyam S, Silverman JG. Sex trafficking, sexual risk, sexually transmitted infection and reproductive health among female sex workers in Thailand. J Epidemiol Community Health. 2011;65(4):334–9.
Sherman SG, Park JN, Galai N, et al. Drivers of HIV infection among cisgender and transgender female sex worker populations in Baltimore city: results from the SAPPHIRE study. J Acquir Immune Defic Syndr. 2019; https://doi.org/10.1097/QAI.0000000000001959.
Brantley ML, Footer KHA, Lim S, Kerrigan D, Sherman SG. Experiences of structural vulnerability among exotic dancers in Baltimore, Maryland: co-occurring social and economic antecedents of HIV/STI risk. Int J Drug Policy. 2017;50:74–81.
Brawn KM, Roe-Sepowitz D. Female juvenile prostitutes: exploring the relationship to substance use. Child Youth Serv Rev. 2008;30(12):1395–402.
Estes RJ, Weiner NA. The commercial sexual exploitation of children in the US, Canada and Mexico. University of Pennsylvania, School of Social Work, Center for the Study of Youth Policy; 2001. Philadelphia, PA
Lutnick A, Harris J, Lorvick J, et al. Examining the associations between sex trade involvement, rape, and symptomatology of sexual abuse trauma. J Interpers Violence. 2015;30(11):1847–63.
Reed SM, Kennedy MA, Decker MR, Cimino AN. Friends, family, and boyfriends: an analysis of relationship pathways into commercial sexual exploitation. Child Abuse Negl. 2019;90:1–12.
Arenas DJ, Thomas A, Wang J, DeLisser HM. A Systematic Review and Meta-Analysis of Depression, Anxiety, and Sleep Disorders in US Adults with Food Insecurity. JGIM 2019;34(12):2874–82.
Aldridge, RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, Tweed EJ, Lewer D, Katikireddi SV, Hayward AC. Morbidity and Mortality in Homeless Individuals, Prisoners, Sex Workers, and Individuals with Substance Use Disorders in High-Income Countries: A Systematic Review and Meta-Analysis. The Lancet 2018;391(10117):241–50.
Lyons T, Shannon K, Richardson L, Simo A, Wood E, Kerr T. Women who use drugs and have sex with women in a Canadian setting: barriers to treatment enrollment and exposure to violence and homelessness. Arch Sex Behav. 2016;45(6):1403–10.
Surratt HL, Inciardi JA. HIV risk, seropositivity and predictors of infection among homeless and non-homeless women sex workers in Miami, Florida, USA. AIDS Care. 2004;16(5):594–604.
Platt L, Grenfell P, Meiksin R, et al. Associations between sex work laws and sex workers’ health: a systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med. 2018;15(12):e1002680.
Bales K, Lize S. Trafficking in persons in the United States: final Report. PsycEXTRA Dataset. 2005; https://doi.org/10.1037/e536242006-001.
Herault N, Ribar DC. Food insecurity and homelessness in the Journeys Home survey. J Hous Econ. 2017;37:52–66.
Acknowledgements
This research was supported by the National Institute on Drug Abuse (R01DA038499). We thank the Sex Workers and Police Promoting Health in Risky Environments (SAPPHIRE) research staff, community advisory board, and the sex workers who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 13 kb)
Rights and permissions
About this article

Cite this article
Footer, K.H.A., White, R.H., Park, J.N. et al. Entry to Sex Trade and Long-Term Vulnerabilities of Female Sex Workers Who Enter the Sex Trade Before the Age of Eighteen. J Urban Health 97, 406–417 (2020). https://doi.org/10.1007/s11524-019-00410-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-019-00410-z