
Abstract
Homelessness remains a societal problem. Compiled evidence of predictors for becoming homeless and exiting homelessness might be used to inform policy-makers and practitioners in their work to reduce homeless-related problems. We examined individual-level predictors for becoming homeless and exiting homelessness by searching PubMed, EMBASE, PsycINFO, and Web of Science up to January 2018. Becoming homeless and exiting homelessness were the outcomes. Observational studies with comparison groups from high-income countries were included. The Newcastle Ottawa Quality Assessment Scale was used for bias assessment. Random effects models were used to calculate pooled odds ratios (ORs) with 95% confidence intervals (CIs). We included 116 independent studies of risk factors for becoming homeless and 18 for exiting homelessness. We found evidence of adverse life events as risk factors for homelessness, e.g., physical abuse (OR 2.9, 95% CI 1.8–4.4) and foster care experiences (3.7, 1.9–7.3). History of incarceration (3.6, 1.3–10.4), suicide attempt (3.6, 2.1–6.3), and psychiatric problems, especially drug use problems (2.9, 1.5–5.1), were associated with increased risk of homelessness. The heterogeneity was substantial in most analyses (I2 > 90%). Female sex (1.5, 1.1–1.9; I2 = 69%) and having a partner (1.7, 1.3–2.1; I2 = 40%) predicted higher chances whereas relationship problems (0.6, 0.5–0.8), psychotic disorders (0.4, 0.2–0.8; I2 = 0%), and drug use problems (0.7, 0.6–0.9; I2 = 0%) reduced the chances for exiting homelessness. In conclusion, sociodemographic factors, adverse life events, criminal behaviour, and psychiatric problems were individual-level predictors for becoming homeless and/or exiting homelessness. Focus on individual-level vulnerabilities and early intervention is needed. PROSPERO registration number: CRD42014013119.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite substantial economic development and growth in the past three decades, homelessness remains an important societal problem in high-income countries which affects millions of people [1, 2]. Severe health problems, including high mortality risk, are associated with homelessness [1, 3,4,5,6,7]. Furthermore, parental homelessness has been linked to offspring’s risk of psychiatric disorders [8]. Thus, the public health burden related to homelessness is substantial and needs to be solved [2, 6, 7].
Currently, the awareness of how welfare reforms and the housing market have contributed to the rise in homelessness is high [2]. However, individual vulnerabilities are also regarded as important contributors to homelessness when structural factors, e.g., low-cost housing, jobs, and income support, become scarce [1]. Reviews of individual-level risk factors for becoming homeless are few and restricted to subgroups of homeless populations [9,10,11,12], and a broad, comprehensive systematic review is thus lacking. Poverty, adverse life experiences, psychiatric problems, and violence have been suggested as risk factors for homelessness [1]. While structural factors are acknowledged to be highly important in the plan for handling the problems of homelessness [13, 14], the literature on individual-level predictors for exiting homelessness is scarce. A study compiling the evidence across high-income countries within these areas of homeless research is lacking. Policy changes and interventions directed at the structural factors contributing to homelessness are important [13], and interventions providing housing and individual support generally have positive effects on obtaining stable housing [15]. However, a better understanding of the individual vulnerabilities related to the risk of becoming and remaining homeless is needed to improve future efforts aimed at reducing the public health problems and societal costs associated with homelessness. For instance, such knowledge is vital in being able to tailor interventions to the needs of different groups of individuals. We aimed to identify individual-related risk factors for becoming homeless and exiting homelessness in a systematic review and meta-analysis.
Methods
This systematic review and meta-analysis was registered at PROSPERO and reported according to MOOSE [16] (see Supplementary file 1). We systematically searched the electronic databases: PubMed, EMBASE, Web of Science, and PsycINFO in June 2016, with a further update in January 2018 using the following search strategy: (((((((((housing) OR correlat*) OR associat*) OR pathway*) OR cause*) OR predict*) OR determinant*) OR ‘risk factor*’)) AND homeless*. No restrictions regarding publication date or language were imposed. As we used a broad search strategy, we did not search reference lists manually, nor did we contact authors to obtain unpublished data.
We included articles meeting the following inclusion criteria: cohort, case-control, or cross-sectional study design including abstracts and theses; from high-income countries [17]; ‘homelessness’ or ‘stable housing’ defined by the study as outcome; a comparison group; and quantitative information on the level of individuals that could be used in the meta-analysis. We included both self-reported and objectively defined criteria for homelessness and stable housing, but people categorised as precariously housed or at risk of homelessness were not considered to be homeless. We excluded review articles, intervention studies, case studies, and discussion papers; studies using youths’ street involvement as outcome; and studies analysing self-perceived causes of the two outcomes.
Data Extraction and Analysis
All titles were screened for duplicates by SFN. Thereafter, two reviewers (SFN and CH) independently selected potentially relevant articles. If one reviewer found an article relevant based on the abstract it was included for full-text reading. Disagreement about inclusion of articles was resolved by discussion between the two reviewers. One author extracted pre-specified data: author name and year of publication, study period, study design, location, population/control group, participants and outcome numbers, outcome, individual-level predictors, and adjustment for sex and/or age. Categorisation of variables was performed based on what was reported in the individual studies. When we identified articles with overlapping population samples, we used information from the largest study, but supplementing with extra information from additional articles; current was preferred over lifetime homelessness; general population over other comparison groups; and adjusted data over unadjusted. We excluded information on income and poverty due to the collinearity with homelessness. All other identified predictors were analysed. For case-control studies, we excluded information of predictors if the temporality was unclear to decrease the risk of reverse causality. Thus, if homelessness was measured retrospectively for longer than 3 months, we only included information on independent factors, i.e., sex and ethnicity.
Risk of Bias Assessment
We assessed risk of bias using the Newcastle Ottawa Quality Assessment Scale (NOS) [18]. The scale ranges from zero to nine stars with a higher number of stars indicating lower risk of bias. Adjustment for sex and age yielded a star each, and so did response rates above 70%. The best rating for each study was used. Several studies were based on self-reported homeless status, and we expected this outcome measure to be as valid as the more objective administrative measures. Thus, we decided that the determination of homeless status by self-report should not be considered bias-prone, and consequently assigned such studies with a star; and defined studies with a bias assessment of seven to nine stars to have low risk of bias. Half of the included studies were bias-rated by two reviewers independently and results were compared to obtain the best possible agreement with the rating. Publication bias was assessed using funnel plots for analyses including at least ten studies. Trim and fill analysis was used to estimate the effect of potential publication bias on the estimates.
Random effects models were used to calculate the pooled odds ratios (ORs) with 95% confidence intervals (CIs) for all analyses. For data given as frequency or proportion, OR could directly be calculated. Variables reported as continuous data were converted from Cohen’s d to log OR and its variance using the two formulas: log OR = d × π/√3 and VlogOR = Vd × π2/3 [19]. Heterogeneity was measured using I2 [20]. In presentation of results, “k” refers to number of studies included in an analysis, and “n” refers to the pooled number of participants in these studies.
We conducted two sensitivity analyses. First, we did the pre-specified influential study analysis to check for the robustness of the results by examining whether any single study considerably changed the results when removed. Second, we restricted the analyses to studies with lowest risk of bias (seven to nine stars in NOS) to see if it changed the results. All analyses were done using Comprehensive Meta-Analysis version 3 [21].
Results
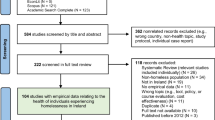
Of 23,576 references screened, 325 publications were selected for full-text review of which 152 publications and 134 independent studies were eligible to be included (Fig. 1).

Study selection of articles and independent study samples of predictors for becoming homeless and exiting homelessness
The systematic review and meta-analysis of risk factors for becoming homeless included 116 independent study samples (see the full list of references in the Supplementary file 2). The 22 cohort studies were published between 1999 and 2017, and 14 (64%) of these were published after 2010. Only one non–English language study was included. Follow-up ranged from 12 weeks to 10 years. Four countries were represented among the cohort studies: the USA (k = 16), the UK (k = 3), Canada (k = 2), and Denmark (k = 1). The study population included between 263 and 4,151,281 individuals. Data from 94 studies was of either case-control or cross-sectional design. These studies were published between 1982 and 2018, and 32 (34%) were published after 2010. Studies came from the USA (k = 74), Canada (k = 6), the UK (k = 5), Denmark (k = 2), Switzerland (k = 2), Australia (k = 2), and Germany, Spain, Ireland, and Portugal (k = 1 each); one of the studies represented the USA and Canada. Study populations included between 23 and 16,744,104 individuals.
Out of the 116 study samples included, the study participants were recruited from psychiatric patient populations in 17 studies (15%); from populations with substance use problems in 12 studies (10%); from populations admitted to emergency departments in seven studies (6%); from low-income, impoverished, or vulnerably housed populations in 19 studies (16%); and from veteran populations in 13 studies (11%). In all, 19 studies (16%) only included women, whereas six studies (5%) only included men. The majority of study samples consisted of adults, but youths were also represented in several studies, and a single study included only children. Studies of the transition from foster care, psychiatric admission, or incarceration were limited. Only few studies were based on large population-based samples. Definitions of homelessness could be categorised in three groups: current homelessness (k = 74 (64%)), lifetime homelessness (k = 17 (15%)), and homelessness measured retrospectively for a period of more than past 3 months and up to past 5 years (k = 22 (19%)) (Supplementary file 2).
The meta-analysis of predictors for exiting homelessness included 18 independent study samples and exclusively cohort studies (follow-up from 2.5 months to 7 years) (see the full list of references in Supplementary file 3). The studies were published between 1996 and 2017, and eight studies (44%) were published after 2010. The studies represented the USA (k = 10), Canada (k = 4), and the UK (k = 2), and Australia and the Netherlands (k = 1 each). Out of the 18 study samples included, the study cohorts of homeless people covered different subgroups of the homeless population, e.g., individuals receiving psychiatric treatment in one study (6%), people with drug use problems in three studies (17%), and homeless veterans in two studies (11%). Four studies (22%) included first-time homeless people. Most studies were based on adults with a single study restricted to homeless elderly women. Six studies (33%) of homeless youths were identified. Three studies (17%) included homeless families. The outcome definitions varied according to criteria for length of stable housing. The majority of studies used stable housing at follow-up without requirement regarding duration (k = 13 (72%)). Others required at least 90 (k = 4) or 30 (k = 1) consecutive days of stable housing.
Risk Factors for Becoming Homeless
Figure 2 summarises the 41 independent meta-analyses for becoming homeless. Several risk factors were identified. Within the sociodemographic factors, male sex (OR 1.5; 95% CI 1.2–1.7, I2 = 99.7%), non-heterosexual identity (2.3; 1.3–4.1, I2 = 92.2%), low educational attainment (1.3; 1.1–1.6, I2 = 96.3%), and unemployment (2.6; 1.8–3.7, I2 = 96.5%) were associated with increased risk of becoming homeless. Veteran status (2.0; 1.3–2.9, I2 = 27.7%) and being single (2.0; 1.7–2.4, I2 = 96.7%) were identified as risk factors as well. Adverse life events from childhood to adulthood were associated with increased risk of becoming homeless. Foster care experiences (3.7; 1.9–7.3, I2 = 95.9%) and physical abuse in childhood (2.9; 1.8–4.4, I2 = 87.7%) were strong risk factors for becoming homeless, but also family problems other than abuse were associated with increased risk. Criminal behaviour and, especially, a history of incarceration (3.6; 1.3–10.4, I2 = 99.9%) were identified as strong risk factors for becoming homeless. Furthermore, people with experiences of runaway behaviour in youth had an OR of 3.3 (95% CI = 2.3–4.8, I2 = 72.8%). All psychiatric problems were associated with increased risk of becoming homeless, e.g., any drug use problem (2.9; 1.5–5.1, I2 = 99.7%), any psychotic disorder (2.1; 1.7–2.6, I2 = 37.2%), and any behaviour problem (1.9; 1.5–2.5, I2 = 96.6%) (Fig. 2). Furthermore, a history of suicide attempt (3.6; 2.1–6.3, I2 = 91.2%) was a strong risk factor for becoming homeless. However, several others of the analysed factors were not consistently associated with increased risk of becoming homeless, e.g., age, non-white ethnicity, social network, sex work, eviction, non-adherence to psychiatric medication, severe physical health problems, and traumatic brain injury. Forest plots for each meta-analysis can be found in online Supplementary file 4.

Forest plot of 41 independent meta-analyses of predictors for becoming homeless with summary estimates
Predictors of Exiting Homelessness
Figure 3 summarises the 21 independent meta-analyses for exiting homelessness. Female sex (1.5; 95% CI 1.1–1.9, I2 = 69.2%), educational attainment (1.4; 1.1–1.7, I2 = 58.8%), and being partnered (1.7; 1.3–2.1, I2 = 40.2%) were associated with increased odds for exiting homelessness. Of the analysed adverse life events, relationship problems were associated with reduced odds for exiting homelessness (0.6; 0.5–0.8, I2 = 0%). Specific psychiatric problems, i.e., drug use problem (0.7; 0.6–0.9, I2 = 0%) and any psychotic disorder (0.4; 0.2–0.8, I2 = 0%), reduced the odds for exiting homelessness. Alcohol use problems, affective disorders, and anxiety disorders were not identified as predictors for exiting homelessness. Neither was age, white ethnicity, employment, social network, a history of incarceration, and sex work. Forest plots for each meta-analysis can be found in Supplementary file 5.

Forest plot of 21 independent meta-analyses of predictors for exiting homelessness with summary estimates
Heterogeneity, Bias Assessment, and Publication Bias
In most analyses of risk factors for becoming homeless, the between-study heterogeneity was high (I2 > 90%) (Fig. 2). For the few factors with heterogeneity below 70%, the number of studies included in the analyses was below ten. For the majority of analyses of predictors for exiting homelessness, the heterogeneity was below 70% (Fig. 3). For most of these analyses, there were also fewer than ten studies included.
Risk of bias in studies of risk factors for becoming homeless ranged from high risk with only one star to the maximum score, and 24 (21%) studies were assessed to be of high quality with low risk of bias (see Supplementary file 2). The scores in bias assessment obtained for studies of predictors for exiting homelessness ranged from three to nine, and 13 (72%) had low risk of bias (see Supplementary file 3).
Some of the analyses showed funnel plots that were consistent with publication bias, i.e., with an overweight of high-standard error studies overestimating the effect rather than underestimating it (see funnel plots in Supplementary files 6–7). However, based on the trim and fill analyses, we found no indication of major changes in the results (data not shown).
Sensitivity Analyses
The one-study–removed sensitivity analyses did not change results considerably in relation to both outcomes (data not shown). However, analyses of eviction and sex work as risk factors for homelessness were characterised by few studies and high variation in results. For suicide attempt, all studies suggested an increased risk of homelessness, but removal of a single study of low-income families [22] resulted in a further increase (4.7; 3.3–6.6, I2 = 69.7%, p ≤ 0.0001). Non-adherence to psychiatric medication became a statistically significant risk factor when removing one study of females [23] (2.0; 1.3–3.2, I2 = 0%, p = 0.001). When removing one study of families using homeless shelters [24], having children became a predictor for exiting homelessness (2.5; 1.1–6.0, I2 = 32.7%, p = 0.035). Substantial variation was found between the three studies examining anxiety disorder according to the odds for exiting homelessness [25,26,27], but all analyses were statistically non-significant.
We did sensitivity analyses in which we only included studies assessed to have low risk of bias. Several factors remained risk factors for becoming homeless with almost unchanged estimates, e.g., foster care (3.9; 1.3–12, I2 = 97.8%) (Supplementary file 8). The estimate of risk for homelessness related to drug use problems increased (3.6; 1.4–9.5, I2 = 99.9%). For a few factors, the association with increased risk of homelessness was no longer significant, i.e., criminal behaviour (p = 0.35), incarceration (p = 0.42), low educational attainment (p = 0.11), and unemployment (p = 0.42). Conversely, young age became a risk factor with increased risk of homelessness (1.5; 1.1–1.9, I2 = 99%). Sensitivity analysis of studies of predictors for exiting homelessness assessed to have low risk of bias did not change results considerably, e.g., for psychotic disorders (0.5; 0.3–0.9, I2 = 0%) (Supplementary file 9). However, the association with drug use problems (p = 0.16) became statistically non-significant.
Discussion
Becoming Homeless
In this large systematic review and meta-analysis of observational studies, several individual-level factors were associated with increased risk of becoming homeless in high-income countries: male sex, non-heterosexual identity, low educational attainment, unemployment, veteran status, being single, adverse life events in childhood and adulthood, criminal behaviour and a history of incarceration, a runaway history, a history of higher number of moves, psychiatric problems, and a history of suicide attempt. Based on the existing evidence, we found no clear associations with the risk of homelessness for the following factors: age, ethnicity, having children, size of social network, dissatisfaction with social support, lack of supportive friends, sex work, eviction, non-adherence to psychiatric medication, severe physical health problems, and traumatic brain injury. However, some of these associations were only examined in few studies. Others displayed substantial heterogeneity, such as ethnicity, which may explain why we did not find as clear associations as previous studies on e.g. ethnicity [1].
Exiting Homelessness
Rather few studies of individual-level predictors for exiting homelessness were identified, but we found female sex, educational attainment, and having a partner to be associated with increased odds of exiting homelessness. Relationship problems, any psychiatric problem, any substance use problem, any drug use problem, and any psychotic disorder were associated with reduced odds for exiting homelessness. Although several analyses were characterised by high heterogeneity or a low number of studies included, we identified several strong associations across high-income countries.
Overall, our findings confirmed previous knowledge [1, 12], but our study provided updated and elaborated evidence with summary estimates, and was not limited to the USA as most of the previous reviews [9, 10, 12]. Family problems and abuse were previously found to be among the most frequent self-reported reasons for street involvement among children and youths [11]. In accordance with this finding, we found foster care experience, childhood abuse, and runaway behaviour to be among the strongest risk factors for becoming homeless. Besides, our findings confirmed a strong link between psychiatric risk factors and homelessness. It also highlighted the association between the risk of homelessness and specific psychiatric problems, e.g., suicide attempt, behaviour problems, affective disorders, and psychotic disorders. Generally, few studies included information on veteran status, sexual identity, emotional abuse, eviction, offspring-related adversity, sex work, history of suicide attempt, non-adherence to psychiatric medication, and traumatic brain injury and other severe physical health problems.
Evidence of associations between social support, adverse life events, criminal behaviour, and specific psychiatric problems according to the chances of exiting homelessness was scarce. We speculate that this might be explained by a general acknowledgement that there is a need for structural support for exiting homelessness and that the individual factors become less important. Previous studies have suggested the importance of employment to homeless people [28,29,30]. We did not find convincing evidence for employment and education to be strong predictors for exiting homelessness, but our study showed that having a partner was a strong contributor.
Prospective and large population-based studies are lacking, especially outside the USA, and could support future interventions addressing problems with homelessness. More research of the link between transitional periods and the risk of homelessness, for instance following foster care, prison, and psychiatric admission, would be useful to document the need for structural changes according to vulnerable periods with high risk of homelessness. Furthermore, research into predictors for exiting homelessness based on large unselected homeless samples could also be useful in guiding future interventions aimed at reducing homelessness.
Strengths and Limitations
This study has important strengths. As far as we know, this is the most comprehensive systematic review and meta-analysis of individual-level predictors for becoming homeless and exiting homelessness to date. A broad search strategy was used with no restrictions. Two reviewers selected the studies for inclusion, and sensitivity analyses were conducted to check the robustness of our findings and consider risk of bias in our interpretation of the high number of suggested predictors. Information from studies in which the temporality was unclear was excluded to decrease the risk of reverse causality.
This study also has several limitations. First, the heterogeneity was very high in most analyses of risk factors for becoming homeless partly because of broad inclusion criteria and substantial methodological differences between the included studies, e.g., outcome definitions, study designs, methods used for data collection, adjustments, and strategy for study sampling. Also, the differences in comparison groups, e.g., veterans, drug users, foster care youths, and psychiatric patients, probably contribute to this. Thus, the pooled ORs should be seen as indicators of increased risk rather than precise estimates of the overall risk for the specific factors. Besides, most studies were from the USA and whether the findings of all risk factors are generalisable to high-income countries in general is unknown. However, we do think that the factors for which a clear tendency towards an increased or a reduced risk was identified can be used as guidance according to whether the individual-level factors analysed in this study are important risk factors of the outcome. Additionally, some predictors were only examined in very few studies, and thus, the analyses of these factors lacked statistical power resulting in less valid estimates. Also, poverty and income were not analysed due to their collinearity with homelessness and, thus, we cannot interpret on the influence of these factors. While poverty is a well-established correlate of homelessness, our aim was to establish risk factors besides the obvious ones of not being able to afford housing [1]. Furthermore, we were not able to study the influence of experiencing more than one risk factor at a time, which could definitely influence the risk. Although we took the risk of bias into account and we excluded information with substantial problems of temporality, we cannot avoid problems with temporality in the observational studies, especially from those using a cross-sectional or retrospective study design. Problems with recall bias in the studies could explain some findings if, for instance, homeless people to a higher degree recall adverse life events than others. Structural factors that certainly will influence the risk of becoming homeless and the chances for exiting homelessness were not taken into account. There are of course difficulties in separating individual- from structural-level predictors, but in the present review, we used the definition of variables that are measurable and variable on the level of individuals. With the broad scope employed in the present review, we also cannot identify the extent to which individual-level risk factors vary according to societal context. We have attempted to minimise the impact of this, however, by focusing exclusively on high-income countries. Although we checked funnel plots, we cannot exclude the risk of publication bias as we did not contact authors for unpublished data. Finally, apart from bias assessment, data extraction was performed by a single author. While she consulted the remaining authors when in doubt, this may have introduced errors in the data extraction process.
Conclusions
In conclusion, we have identified several strong individual-level sociodemographic, social, and psychiatric predictors for becoming homeless and exiting homelessness. Even adversities in childhood seem to play a role to the risk of later homelessness and this supports the need for improved social interventions aimed at antecedents for street involvement and family problems. An increased focus on the risk of homelessness when leaving prison might also reduce homelessness. Also, people with a history of suicide attempt, drug use problems, and other psychiatric problems seem to require extra support and awareness from health care and social services to avoid that these health problems lead to social exclusion in the longer run. The strongest risk factors are in themselves important to intervene against, but with this review, their association with homelessness has become clearer. Even in the case of non-modifiable risk factors, it would then also be prudent to have a special focus on these at-risk groups, and to tailor prevention efforts and interventions to the needs of these groups. Interventions aimed at supporting people to exit from homelessness should be targeted according to individual needs taking into account the availability of and problems with social relations and psychiatric problems. Our findings provide the strongest evidence to date based on observational studies for the need of improved structural support to the identified vulnerable groups in future initiatives aimed at preventing and reducing homelessness in high-income countries. While our findings related to individual-level risk factors, such interventions may still need to be context-specific, as societal-level factors are certainly also of tremendous importance.
References
Fazel S, Geddes JR, Kushel M. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet. 2014;384(9953):1529–40. https://doi.org/10.1016/S0140-6736(14)61132-6.
Fransham M, Dorling D. Homelessness and public health. BMJ. 2018;360:k214. https://doi.org/10.1136/bmj.k214.
Nielsen SF, Hjorthøj CR, Erlangsen A, Nordentoft M. Psychiatric disorders and mortality among people in homeless shelters in Denmark: a nationwide register-based cohort study. Lancet (London, England). 2011;377(9784):2205–14. https://doi.org/10.1016/S0140-6736(11)60747-2.
Fazel S, Khosla V, Doll H, Geddes J. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. McGrath J, ed. PLoS Med. 2008;5(12):e225. https://doi.org/10.1371/journal.pmed.0050225.
Baggett TP, Hwang SW, O’Connell JJ, Porneala BC, Stringfellow EJ, Orav EJ, et al. Mortality among homeless adults in Boston: shifts in causes of death over a 15-year period. JAMA Intern Med. 2013;173(3):189–95. https://doi.org/10.1001/jamainternmed.2013.1604.
Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, et al. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. Lancet (London, England). 2018;391(10117):241–50. https://doi.org/10.1016/S0140-6736(17)31869-X.
Feodor Nilsson S, Laursen TM, Hjorthøj C, Nordentoft M. Homelessness as a predictor of mortality: an 11-year register-based cohort study. Soc Psychiatry Psychiatr Epidemiol. 2018;53(1):63–75. https://doi.org/10.1007/s00127-017-1456-z.
Nilsson SF, Laursen TM, Hjorthøj C, Thorup A, Nordentoft M. Risk of psychiatric disorders in offspring of parents with a history of homelessness during childhood and adolescence in Denmark: a nationwide, register-based, cohort study. Lancet Public Health. 2017;2(12):e541–50. https://doi.org/10.1016/S2468-2667(17)30210-4.
Tsai J, Rosenheck RA. Risk factors for homelessness among US veterans. Epidemiol Rev. 2015;37(1):177–95. https://doi.org/10.1093/epirev/mxu004.
Byrne T, Montgomery AE, Dichter ME. Homelessness among female veterans: a systematic review of the literature. Women Health. 2013;53(6):572–96. https://doi.org/10.1080/03630242.2013.817504.
Embleton L, Lee H, Gunn J, Ayuku D, Braitstein P. Causes of child and youth homelessness in developed and developing countries: a systematic review and meta-analysis. JAMA Pediatr. 2016;170(5):435–44. https://doi.org/10.1001/jamapediatrics.2016.0156.
Susser E, Moore R, Link B. Risk factors for homelessness. Epidemiol Rev. 1993;15(2):546–56. http://www.ncbi.nlm.nih.gov/pubmed/8174670. Accessed February 11, 2019
Hwang SW, Burns T. Health interventions for people who are homeless. Lancet (London, England). 2014;384(9953):1541–7. https://doi.org/10.1016/S0140-6736(14)61133-8.
Stergiopoulos V, Hwang SW, Gozdzik A, Nisenbaum R, Latimer E, Rabouin D, et al. Effect of scattered-site housing using rent supplements and intensive case management on housing stability among homeless adults with mental illness: a randomized trial. JAMA. 2015;313(9):905–15. https://doi.org/10.1001/jama.2015.1163.
O’Campo P, Stergiopoulos V, Nir P, et al. How did a Housing First intervention improve health and social outcomes among homeless adults with mental illness in Toronto? Two-year outcomes from a randomised trial. BMJ Open. 2016;6(9):e010581. https://doi.org/10.1136/bmjopen-2015-010581.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12. http://www.ncbi.nlm.nih.gov/pubmed/10789670. Accessed February 11, 2019.
The World Bank. High Income. https://data.worldbank.org/income-level/high-income. Published 2016. Accessed February 11, 2019.
Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Published 2014. Accessed February 11, 2019.
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Converting Among Effect Sizes. Introduction to Meta-analysis. Chichester: Wiley; 2009. http://doi.wiley.com/10.1002/9780470743386
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Biostat Inc. Comprehensive Meta-Analysis Software (CMA). https://www.meta-analysis.com/index.php?cart=BP2W1080211. Published 2019. Accessed February 11, 2019.
Bassuk EL, Weinreb LF, Buckner JC, Browne A, Salomon A, Bassuk SS. The characteristics and needs of sheltered homeless and low-income housed mothers. JAMA. 1996;276(8):640–6. http://www.ncbi.nlm.nih.gov/pubmed/8773638. Accessed February 11, 2019
Caton CL, Shrout PE, Dominguez B, Eagle PF, Opler LA, Cournos F. Risk factors for homelessness among women with schizophrenia. Am J Public Health 1995;85(8 Pt 1):1153–1156. http://www.ncbi.nlm.nih.gov/pubmed/7625518. Accessed February 11, 2019.
Rocha C, Johnson AK, McChesney KY, Butterfield WH. Predictors of permanent housing for sheltered homeless families. Fam Soc J Contemp Soc Serv. 1996;77(1):50–7. https://doi.org/10.1606/1044-3894.838.
Greenberg GA, Hoblyn J, Seibyl C, Rosenheck RA. Housing outcomes for hospitalized homeless veterans. J Health Care Poor Underserved. 2006;17(2):425–40. https://doi.org/10.1353/hpu.2006.0061.
Spicer B, Smith DI, Conroy E, Flatau PR, Burns L. Mental illness and housing outcomes among a sample of homeless men in an Australian urban centre. Aust N Z J Psychiatry. 2015;49(5):471–80. https://doi.org/10.1177/0004867414563187.
Van Straaten B, Van der Laan J, Rodenburg G, Boersma SN, Wolf JRLM, Van de Mheen D. Dutch homeless people 2.5 years after shelter admission: what are predictors of housing stability and housing satisfaction? Health Soc Care Community. 2017;25(2):710–22. https://doi.org/10.1111/hsc.12361.
Shaheen G, Rio J. Recognizing work as a priority in preventing or ending homelessness. J Prim Prev. 2007;28(3–4):341–58. https://doi.org/10.1007/s10935-007-0097-5.
Poremski D, Rabouin D, Latimer E. A randomised controlled trial of evidence based supported employment for people who have recently been homeless and have a mental illness. Adm Policy Ment Health Ment Health Serv Res. 2017;44(2):217–24. https://doi.org/10.1007/s10488-015-0713-2.
Poremski D, Stergiopoulos V, Braithwaite E, Distasio J, Nisenbaum R, Latimer E. Effects of housing first on employment and income of homeless individuals: results of a randomized trial. Psychiatr Serv. 2016;67(6):603–9. https://doi.org/10.1176/appi.ps.201500002.
Acknowledgements
Thanks to Manon Chaine and Karl Ole Köhler-Forsberg for help with translation of French and German articles during this work.
Contributors
SFN and CH led the conception and design of the study. SFN did the literature search. SFN and CH selected the studies. SFN extracted the data. SFN and CH did the quality assessment. SFN performed the analyses and interpreted data with supervision from CH and MN. SFN drafted the manuscript with critical revisions for important intellectual content from CH and MN.
Funding
This study was funded by a stipend from the University of Copenhagen and by iPSYCH – The Lundbeck Foundation Initiative for Integrated Psychiatric Research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Supplementary file 1
(PDF 55 kb)
Supplementary file 2
(PDF 386 kb)
Supplementary file 3
(PDF 77 kb)
Supplementary file 4
(PDF 2223 kb)
Supplementary file 5
(PDF 569 kb)
Supplementary file 6
(PDF 779 kb)
Supplementary file 7
(PDF 180 kb)
Supplementary file 8
Forest plot of meta-analyses of predictors for becoming homeless based on studies with low risk of bias with summary estimates (PNG 283 kb)
High resolution image
(EPS 51 kb)
Supplementary file 9
Forest plot of meta-analyses of predictors for exiting homelessness based on studies with low risk of bias with summary estimates (PNG 143 kb)
High resolution image
(EPS 33 kb)
Rights and permissions
About this article

Cite this article
Nilsson, S.F., Nordentoft, M. & Hjorthøj, C. Individual-Level Predictors for Becoming Homeless and Exiting Homelessness: a Systematic Review and Meta-analysis. J Urban Health 96, 741–750 (2019). https://doi.org/10.1007/s11524-019-00377-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-019-00377-x