
Abstract
There were over 23,000 opioid overdose deaths in the USA in 2013, and opioid-related mortality is increasing. Increased access to naloxone, particularly through community-based lay naloxone distribution, is a widely supported strategy to reduce opioid overdose mortality; however, little is known about the ecological and spatial patterns of the distribution and utilization of lay naloxone. This study aims to investigate the neighborhood-level correlates and spatial relationships of lay naloxone distribution and utilization and opioid overdose deaths. We determined the locations of lay naloxone distribution sites and the number of unintentional opioid overdose deaths and reported reversal events in San Francisco census tracts (n = 195) from 2010 to 2012. We used Wilcoxon rank-sum tests to compare census tract characteristics across tracts adjacent and not adjacent to distribution sites and multivariable negative binomial regression models to assess the association between census tract characteristics, including distance to the nearest site, and counts of opioid overdose deaths and naloxone reversal events. Three hundred forty-two opioid overdose deaths and 316 overdose reversals with valid location data were included in our analysis. Census tracts including or adjacent to a distribution site had higher income inequality, lower percentage black or African American residents, more drug arrests, higher population density, more overdose deaths, and more reversal events (all p < 0.05). In multivariable analysis, greater distance to the nearest distribution site (up to a distance of 4000 m) was associated with a lower count of Naloxone reversals [incidence rate ratio (IRR) = 0.51 per 500 m increase, 95% CI 0.39–0.67, p < 0.001] but was not significantly associated with opioid overdose deaths. These findings affirm that locating lay naloxone distribution sites in areas with high levels of substance use and overdose risk facilitates reversals of opioid overdoses in those immediate areas but suggests that alternative delivery methods may be necessary to reach individuals in other areas with less concentrated risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The global prevalence of opioid use increased steadily from 2009 to 2014, and opioid dependence is the most important contributor to the global burden of disease from illicit drug dependence.1,2 In the USA, an estimated 25 million people initiated non-medical use of opioid analgesics between 2002 and 2011, and the age-adjusted mortality rate from drug poisoning more than doubled in the same period.3,4 Notwithstanding a slowing of the increases in abuse and mortality related to opioid analgesics in recent years, there has also been a 37 % annual increase in heroin-related deaths from 2010 to 2013 and a total of over 23,000 opioid overdose deaths in 2013.3,5–7
In response to these global and domestic trends, the World Health Organization, American Medical Association, American Public Health Association, and others have recommended increased lay person access to naloxone, an opioid antagonist that reverses the effects of overdose, as a key strategy in reducing overdose-related mortality.8–12 Whereas emergency medical services (EMS) are the primary source of naloxone access outside of hospitals, access for community bystanders continues to expand in the USA.13,14 In total, 36 states and the District of Columbia (D.C.) have passed laws to facilitate the prescription and distribution of naloxone. The last available census of community-based naloxone distribution programs reported 644 sites in 32 states and D.C. in 2013, up from 188 in 15 states and D.C. in 2010.8,15 A growing body of research has demonstrated the viability and effectiveness of community naloxone programs in training non-medical bystanders, distributing naloxone, and facilitating its use to reverse opioid overdoses.8,16–20
A wide range of physical and social characteristics of neighborhoods has been linked to substance use and overdose mortality and are theorized to operate through a variety of mechanisms.21–25 Specifically, residents of lower income neighborhoods may be more likely to engage in substance use and be at higher risk of overdose as a result of limited access to health and social services, disproportionate psychosocial stress, and lower levels of social capital and social trust.25–29 Income maldistribution may influence substance use behavior through underinvestment in social resources such as education and healthcare, or by eroding social capital, and promoting mistrust of authority and reluctance to seek medical help in cases of drug overdose.22,25,30–33 Greater police activity may heighten fear of arrest and result in reluctance to seek help when witnessing an overdose and may also drive substance use to more secluded and isolated areas, where overdoses may be less likely to be witnessed and victims less likely to receive medical attention.23,34–38 Population density may affect substance use and overdose risk through a higher degree of collective socialization within dense urban areas, in which the norms and activities of a social network influence individual behaviors.39–42 In addition, spatial analysis is increasingly used to examine critical public health issues in urban areas, including the location of HIV services, improper syringe disposal, and hotspots of high risk.43–49 Despite this extensive body of research pertaining to substance use and overdose risk, no studies have assessed the relationship between neighborhood-level factors and lay naloxone distribution and little is known about the spatial patterns of the distribution and utilization of lay naloxone.
To build on existing overdose research and contribute to our understanding of community-based naloxone distribution, we assessed the neighborhood-level correlates of naloxone reversals and opioid overdose deaths, including proximity to naloxone distribution sites. We used data from the Drug Overdose Prevention Education (DOPE) Project, an overdose prevention and naloxone distribution program in San Francisco, California and the California Electronic Death Reporting System (CA-EDRS). Prior studies using these data sources have described DOPE Project participant demographics, refills, and reversals and explored spatial patterns of opioid overdose deaths, but this is the first study using these data to explore the neighborhood-level correlates and spatial relationships of lay naloxone distribution, utilization, and opioid overdose deaths.50–53
Methods
Data Collection and Measures
Opioid Overdose Deaths
The locations of all opioid overdose deaths in San Francisco between January 1, 2010 and December 31, 2012 were extracted from CA-EDRS using methods described elsewhere.53 Cases were included if the death occurred within the City and County of San Francisco, and the cause of death included any illicit opiate (e.g., heroin, morphine) or synthetic or semi-synthetic opioid analgesic (e.g., methadone, oxycodone, fentanyl). Cases were excluded if the decedent was under 18 or if the primary cause of death did not include “acute intoxication” or was determined to be intentional (i.e., suicide or homicide). Out-of-hospital deaths were mapped to their observed locations, and in-hospital deaths mapped to the decedent’s San Francisco residence. Both were then geocoded using an ESRI ArcGIS address locator and in a final step mapped to census tracts.54,55
Naloxone Administration Events
Naloxone administration events occurring in San Francisco between January 1, 2010 and December 31, 2012 were obtained from the DOPE Project. The DOPE Project provides brief overdose education and naloxone trainings and distributes 2-dose intranasal or injectable naloxone kits to individuals at needle exchange sites, re-entry programs, pain management clinics, opioid substitution treatment programs, and single room occupancy hotels (SROs). Participants who return to any DOPE site to obtain a new naloxone kit complete a questionnaire in which they report the date and nearest intersection of any event in which naloxone was administered on a suspected overdose victim (referred to here as a reversal) as well as the substances involved.
All reversals for which valid location data was available were geocoded, and the count of reversal events in each census tract was determined using the same methods as the overdose deaths.
DOPE Distribution Site Locations
The DOPE Project distributed naloxone from a total of 17 locations that had recurring distribution events during the study period. These sites were selected for naloxone distribution based on geocoding of heroin overdose deaths from 1997 to 1999 and later on perceived need.52 Because naloxone was distributed from some sites infrequently or for only a small portion of the study period, this analysis only includes DOPE Project sites that provided trainings and naloxone distribution during more than 18 of the 36 months of the study period (n = 11). Locations for the sites included in our analysis, which distributed 87 % of the total number of naloxone kits distributed from all 17 sites during the study period, were obtained from DOPE Project distribution records and geocoded using the ESRI ArcGIS address locator. We classified all census tracts according to whether they included a distribution site or were adjacent to a census tract that did. Distance to the nearest DOPE Project site was calculated in meters from the census tract centroid.
Census Tract Characteristics
Census tract socioeconomic status was measured by tract median income, and economic inequality was measured by tract Gini coefficient, both obtained from the 2009 to 2013 American Community Survey 5-Year Estimates.56,57 A Gini coefficient of zero represents perfect equality, and a coefficient of one represents maximal inequality; the overall value for San Francisco is 0.516.56
To measure police activity, the number of drug arrests in each census tract was obtained using geocoded crime incident reports from the San Francisco Police Department between January 1, 2010 and December 31, 2012.58 In addition to opioids, drug arrests can involve marijuana, cocaine, methamphetamine, and other controlled substances.
Consistent with a prior study assessing neighborhood correlates of overdose mortality as well as the disproportionate rate of opioid overdose mortality among African Americans in San Francisco, census tract racial composition was measured by the percentage of residents that identified as black or African American, as reported in Summary File 1 of the 2010 Census.22,53,59
The total population of each census tract was obtained from the Summary File 1 of the 2010 Census. Population density was calculated by dividing the total census tract population by its area, calculated using ESRI ArcMap 10 (ESRI, Redlands, CA).60
Descriptive Statistics and Bivariate Analyses
Wilcoxon rank-sum tests were used to compare median income, Gini coefficient, number of drug arrests, percentage of black or African American residents, population density, and our two primary outcomes, overdose deaths, and naloxone reversal events, between census tracts including or adjacent to a naloxone distribution site and all other census tracts. We then used Kruskal-Wallis tests to assess unadjusted associations between census tract characteristics and our two outcomes.
We also assessed differences in the distance to the nearest DOPE Project site between census tracts that had at least one heroin-related overdose death and census tracts that had only non-heroin-related overdose deaths using a Wilcoxon rank-sum test.
Multivariable Analyses
With census tract as the unit of analysis, we used negative binomial regression models to examine the independent relationship between distance to nearest DOPE Project site and 1) the number of opioid overdose deaths and 2) the number of naloxone reversal events. We hypothesized that the primary driver of these events is the rate of opioid use, which was not directly measured. Thus, our models adjusted for available markers of that rate, specifically the characteristics assessed in our bivariate analysis, as well as population size.
We modeled the effect of distance to nearest DOPE Project site as piecewise linear with a change in slope at 4000 m, located using a non-parametric smoother. This approach provides separate estimates of the distance effect within and beyond 4000 m from a DOPE Project site. The specification of other covariate effects was determined using orthogonal contrasts to assess linearity across quartiles; those with no clear evidence (p > 0.1) of non-linearity were included as continuous and otherwise as quartiles.
Results
Opioid Overdose Deaths
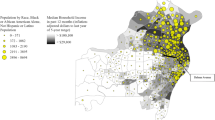
There were 353 accidental opioid overdose deaths in San Francisco in the study period. Eleven (3 %) cases occurred in-hospital and the decedent was not a resident of San Francisco with a valid address so were excluded from analysis. The remaining 342 opioid overdose deaths were included in this analysis. Eighteen (5 %) of the included deaths occurred in-hospital and were linked to the decedent’s address. Fig. 1a shows that while opioid overdose deaths were clustered around DOPE Project sites, they were nonetheless observed throughout the city.

a Overdose deaths in San Francisco, CA 2010–2012. b Naloxone reversals in San Francisco, CA 2010–2012.
Naloxone Reversal Events
There were 450 naloxone reversal events reported to DOPE Project sites in the study period. Of these, 316 (70 %) had valid location data and were included in our analysis; 99 (22 %) had missing or invalid location data, and 35 (8 %) occurred outside of San Francisco and were thus excluded from analysis. Fig. 1b shows that naloxone reversal events were primarily clustered near DOPE Project sites, with few reversal events occurring in other areas.
Descriptive Statistics and Bivariate Analyses
Of the 195 census tracts included in our analysis, 44 (23 %) had a DOPE Project distribution site or were adjacent to a census tract that had one (Table 1). Those 44 census tracts had significantly higher income inequality and population density, lower percent black or African American residents, and more drug arrests, overdose deaths, and reversal events (all p < 0.05).
There was an average of 1.8 opioid overdose deaths per census tract in the study period (Table 2). The mean number of overdose deaths declined across increasing quartiles of distance to nearest DOPE site and median income and increased across quartiles of Gini coefficient, number of drug arrests, percentage black or African American residents, and population density.
There was an average of 1.6 naloxone reversal events per census tract in the study period (Table 2). The mean number of reversal events declined across increasing quartiles of distance to nearest DOPE site and median income and increased across quartiles of number of drug arrests, percentage black or African American residents, and population density.
Of the 119 census tracts that had at least one opioid overdose death, those that had at least one heroin-related overdose death were located significantly closer to DOPE Project sites compared to census tracts that had only non-heroin-related overdose deaths (Table 3).
Multivariable Analyses
The results of our multivariable negative binomial regression models are shown in Tables 4 and 5. In the model for opioid overdose deaths, distance to nearest DOPE site (up to a distance of 4000 m) was not statistically significantly associated with number of overdose deaths [incident rate ratio (IRR) = 0.88 per 500 m increase, 95% CI 0.76–1.02, p = 0.093]. Overdose deaths were inversely associated with median income [IRR = 0.93 per $10,000 increase, 95% CI 0.87–0.99, p = 0.021] but increased with numbers of drug arrests [IRR = 1.50 per 10-fold increase, 95% CI 1.34–1.68, p < 0.001] and percentage of black or African American residents [IRR = 1.13 per 10 % increase, 95% CI 1.00–1.27, p = 0.049].
In the model for naloxone reversal events, distance to the nearest DOPE site (up to 4000 m) was independently associated with a 49 % lower count of naloxone reversals [IRR = 0.51 per 500 m, 95% CI 0.39–0.67, p < 0.001]. Naloxone reversals increased with the number of drug arrests [IRR = 2.29 per 10-fold increase, 95% CI 1.86–2.82, p < 0.001] but declined with quartile of percentage of black or African American residents [Q2 vs Q1: IRR = 0.26, 95% CI 0.11–0.60, p = 0.002; Q3 vs Q1: IRR = 0.33, 95% CI 0.15–0.73, p = 0.006; Q4 vs Q1: IRR = 0.31, 95% CI 0.13–0.74, p = 0.009].
Discussion
Our analyses determined that DOPE project sites are located in and near census tracts with lower socioeconomic status, higher income inequality, more drug arrests, lower percent black or African American residents, higher population density, and more overdose deaths compared to the rest of San Francisco. After accounting for these census tract characteristics, we found strong evidence that proximity to DOPE Project distribution sites increased reversal events, which were clustered in census tracts including or adjacent to a site. In contrast, we found only weak evidence that proximity increased overdose mortality, which was more widely dispersed across the city. In addition, we found that heroin-related overdose deaths occurred in census tracts that were closer to DOPE Project sites than opioid overdose deaths that did not involve heroin. This is the first analysis to examine the census tract correlates and spatial relationships between naloxone distribution sites, opioid overdose deaths, and naloxone reversal events and has important implications for understanding current opioid overdose patterns and their relationship to lay naloxone access and utilization.
The DOPE Project locates its services and distributes naloxone in the census tracts with the highest numbers of opioid overdose deaths. Moreover, 76 % of opioid overdose deaths in San Francisco from 2010 to 2012 occurred in either the decedent’s residence or the residence of a friend or family member, confirming that DOPE project sites are appropriately located to provide convenient services to those at highest risk for overdose. Geographic proximity of the target population to health care services has been shown to be an important driver of service utilization61; for example, people who inject drugs who live closer to syringe exchange sites are more likely to use these services.62 DOPE Project sites are also located in census tracts with lower income and higher levels of police activity, which have been associated with drug use and overdose mortality.23,25,28
A prior analysis of data from the DOPE Project has shown that this community-based naloxone distribution program facilitates large numbers of overdose reversals among high-risk populations.51 However, Fig. 1a shows that while a large proportion of opioid overdose deaths occur close to naloxone distribution sites, many deaths occur in areas distant from these sites, possibly representing a distinct population not readily reached by traditional lay naloxone distribution. It has been previously shown that heroin is involved in the majority of DOPE Project reversals (90.3 % from 2010 to 2013), but only a small fraction of overdose deaths in San Francisco (9.4 % from 2010–2012), with the vast majority of overdose deaths involving prescription opioid analgesics.51,53 We also found that opioid overdose deaths that do not involve heroin tend to occur in census tracts farther from DOPE Project sites. Together, these findings may explain the fact that we found an independent association of proximity to a distribution site and reversal events but not overdose deaths. It is possible that users of opioids other than heroin that live in outlying areas are not being reached through community-based naloxone distribution as readily as heroin users in areas with historically endemic levels of substance use where DOPE Project sites are appropriately located.52 In New York City, opioid analgesic overdose fatalities exhibit spatial patterns distinct from those related to heroin.25 Nationally, the majority of naloxone reversals by laypersons target heroin overdoses, but the majority of opioid overdose deaths involve prescription analgesics, further suggesting that these findings may not be unique to San Francisco.8
The strong positive associations between drug arrests, a marker of substance use, and both overdose mortality and naloxone reversals are consistent with prior research and further show that naloxone is being used in the census tracts with the greatest risk of overdose mortality.23 These associations may also suggest that increased police activity directly influences overdose risk, perhaps by promoting higher risk drug use practices (e.g., rushed injections) or increasing reluctance to seek medical attention. Despite the utility of this marker of the community-level use of opioids, a reliable independent measure of opioid use is needed in order to better understand our findings related to police activity.
Lay naloxone distribution in San Francisco has demonstrated success in reaching individuals and facilitating overdose reversals in the high-risk areas where distribution sites are located, but additional methods may be needed to reach individuals at risk of opioid overdose who do not live near naloxone distribution sites, particularly those who use opioid analgesics. Limited resources for community-based naloxone distribution programs such as the DOPE Project, together with a lower concentration of overdose risk and service demand in these outlying areas, suggest that additional community-based distribution sites may not be appropriate for these areas.8,63 Current studies in San Francisco aim to assess the feasibility and acceptability of naloxone prescription programs at multi-provider primary care clinics in a safety net healthcare system, as well as an educational outreach program with the goal of increasing naloxone prescribing among medical providers (NIDA R21 DA036776; E. Behar, personal communication, October 5, 2015). Both of these programs have the potential to facilitate broader distribution of naloxone throughout the city. In multiple states in the USA, models of pharmacy-based naloxone distribution have leveraged the capacity of pharmacies and the skills of pharmacists to expand access to naloxone beyond those who are reached by community-based organizations.64–66 Recent qualitative studies examining the feasibility of implementing naloxone prescription programs in both primary care and emergency department settings have found support among clinical staff but have also identified logistical, attitudinal, and knowledge barriers that would need to be addressed to enhance uptake among providers.67,68 Although primary care clinics, emergency departments, and pharmacies offer promising avenues for reaching opioid users at risk of overdose, additional research and pilot interventions are needed to reduce opioid overdose mortality among individuals not personally accessing or associated with individuals who access lay naloxone distribution services such as the DOPE Project.
This study has several limitations. First, reversal events are reported only by individuals who return to a DOPE Project site to obtain a naloxone refill. In addition, only 78 % of reported reversals had valid location data. These missing data could bias our findings if either obtaining a refill or having missing or invalid location data was associated with where the relevant reversal occurred. Another limitation is that our analysis only includes DOPE Project sites that distributed naloxone kits during more than half of the period under study; however, these sites accounted for the majority (87 %) of kits distributed from regularly scheduled sites. Also, geographic distance between census tract centroids and DOPE Project sites may not adequately reflect difficulty of access, in particular by public transportation.
This study affirms that locating lay naloxone distribution sites in areas with high levels of substance use and overdose risk facilitates reversals of opioid overdoses in those immediate areas but suggests that alternative delivery methods may be necessary to reach individuals in other areas with less concentrated risk.
References
United Nations Office on Drugs and Crime. World Drug Report 2014
Degenhardt L, Hall W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet. 2012; 379(9810): 55–70.
Dart RC, Surratt HL, Cicero TJ, et al. Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015; 372(3): 241–248.
Warner M, Hedegaard H, Chen LH. Trends in drug-poisoning deaths involving opioid analgesics and heroin: United States, 1999–2012. In: National Center for Health Statistics CfDCaP, ed; 2014
Unick GJ, Rosenblum D, Mars S, Ciccarone D. Intertwined epidemics: national demographic trends in hospitalizations for heroin- and opioid-related overdoses, 1993–2009. PLoS One. 2013; 8(2), e54496.
Hedegaard HC, L.H., Warner M. Drug-poisoning Deaths Involving Heroin: United States, 2000–2013: National Center for Health Statistics, Centers for Disease Control and Prevention; 2015
Rudd RA, Paulozzi LJ, Bauer MJ, et al. Increases in heroin overdose deaths—28 States, 2010 to 2012. MMWR Morb Mortal Wkly Rep. 2014; 63(39): 849–854.
Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. MMWR Morb Mortal Wkly Rep. 2015; 64(23): 631–635.
World Health Organization. WHO model list of essential medicines (18th Edition); 2013
World Health Organization. Consolidated guidelines on HIV prevention, treatment and care for key populations. Geneva, Switzerland: World Health Organization; 2014.
American Medical Association. Policy D-95.987: prevention of opioid overdose. In: Association AM, ed; 2015
American Public Health Association. Policy 20133: reducing opioid overdose through education and naloxone distribution. In: Organization APH, ed; 2013
Davis CS, Southwell JK, Niehaus VR, Walley AY, Dailey MW. Emergency medical services naloxone access: a national systematic legal review. Acad Emerg Med. 2014; 21(10): 1173–1177.
Davis CS, Walley AY, Bridger CM. Lessons learned from the expansion of naloxone access in Massachusetts and North Carolina. J Law Med Ethics. 2015; 43(Suppl 1): 19–22.
LawAtlas—the policy surveillance portal. Naloxone overdose prevention laws map. Available at: http://lawatlas.org/query?dataset=laws-regulating-administration-of-naloxone. Accessed 15 Oct 2015.
Bennett T, Holloway K. The impact of take-home naloxone distribution and training on opiate overdose knowledge and response: an evaluation of the THN Project in Wales. Drugs: education, prevention, and policy. 2012; 19(4): 320–328.
Strang J, Manning V, Mayet S, et al. Overdose training and take-home naloxone for opiate users: prospective cohort study of impact on knowledge and attitudes and subsequent management of overdoses. Addiction. 2008; 103(10): 1648–1657.
Wagner KD, Valente TW, Casanova M, et al. Evaluation of an overdose prevention and response training programme for injection drug users in the Skid Row area of Los Angeles. CA Int J Drug Policy May. 2010; 21(3): 186–193.
Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013; 346: f174.
Davidson PJ, Wheeler E, Proudfoot J, Ronghui X, Wagner KD. Abstract #150: Naloxone distribution to drug users in California and opioid-related overdose death rates. Paper presented at: College on Problems of Drug Dependence 77th Annual Meeting, 2015; Phoenix, Arizona
Hembree C, Galea S, Ahern J, et al. The urban built environment and overdose mortality in New York City neighborhoods. Health Place. 2005; 11(2): 147–156.
Galea S, Ahern J, Vlahov D, et al. Income distribution and risk of fatal drug overdose in New York City neighborhoods. Drug Alcohol Depend. 2003; 70(2): 139–148.
Bohnert AS, Nandi A, Tracy M, et al. Policing and risk of overdose mortality in urban neighborhoods. Drug Alcohol Depend. 2011; 113(1): 62–68.
Fuller CM, Borrell LN, Latkin CA, et al. Effects of race, neighborhood, and social network on age at initiation of injection drug use. Am J Public Health. 2005; 95(4): 689–695.
Cerda M, Ransome Y, Keyes KM, et al. Revisiting the role of the urban environment in substance use: the case of analgesic overdose fatalities. Am J Public Health. 2013; 103(12): 2252–2260.
Gotsens M, Mari-Dell'Olmo M, Martinez-Beneito MA, et al. Socio-economic inequalities in mortality due to injuries in small areas of ten cities in Spain (MEDEA Project). Accid Anal Prev. 2011; 43(5): 1802–1810.
Marzuk PM, Tardiff K, Leon AC, et al. Poverty and fatal accidental drug overdoses of cocaine and opiates in New York City: an ecological study. Am J Drug Alcohol Abuse. 1997; 23(2): 221–228.
Boardman JD, Finch BK, Ellison CG, Williams DR, Jackson JS. Neighborhood disadvantage, stress, and drug use among adults. J Health Soc Behav. 2001; 42(2): 151–165.
Galea S, Ahern J, Vlahov D. Contextual determinants of drug use risk behavior: a theoretic framework. J Urban Health. Dec 2003;80(4 Suppl 3):iii50-58
Nandi A, Galea S, Ahern J, Bucciarelli A, Vlahov D, Tardiff K. What explains the association between neighborhood-level income inequality and the risk of fatal overdose in New York City? Soc Sci Med. 2006; 63(3): 662–674.
Hannon L, Cuddy MM. Neighborhood ecology and drug dependence mortality: an analysis of New York City census tracts. Am J Drug Alcohol Abuse. 2006; 32(3): 453–463.
Ross CE, Jang SJ. Neighborhood disorder, fear, and mistrust: the buffering role of social ties with neighbors. Am J Community Psychol. 2000; 28(4): 401–420.
Kawachi I, Kennedy BP. Income inequality and health: pathways and mechanisms. Health Serv Res. 1999; 34(1 Pt 2): 215–227.
Baca CT, Grant KJ. What heroin users tell us about overdose. J Addict Dis. 2007; 26(4): 63–68.
Dovey K, Fitzgerald J, Choi Y. Safety becomes danger: dilemmas of drug-use in public space. Health Place. 2001; 7(4): 319–331.
Pollini RA, McCall L, Mehta SH, Vlahov D, Strathdee SA. Non-fatal overdose and subsequent drug treatment among injection drug users. Drug Alcohol Depend. 2006; 83(2): 104–110.
Tobin KE, Davey MA, Latkin CA. Calling emergency medical services during drug overdose: an examination of individual, social and setting correlates. Addiction. 2005; 100(3): 397–404.
Tracy M, Piper TM, Ompad D, et al. Circumstances of witnessed drug overdose in New York City: implications for intervention. Drug Alcohol Depend. 2005; 79(2): 181–190.
Schroeder JR, Latkin CA, Hoover DR, Curry AD, Knowlton AR, Celentano DD. Illicit drug use in one's social network and in one's neighborhood predicts individual heroin and cocaine use. Ann Epidemiol. 2001; 11(6): 389–394.
Galea S, Rudenstine S, Vlahov D. Drug use, misuse, and the urban environment. Drug Alcohol Rev. 2005; 24(2): 127–136.
Latkin CA, Forman V, Knowlton A, Sherman S. Norms, social networks, and HIV-related risk behaviors among urban disadvantaged drug users. Soc Sci Med. 2003; 56(3): 465–476.
Latkin CA, Hua W, Forman VL. The relationship between social network characteristics and exchanging sex for drugs or money among drug users in Baltimore, MD. USA Int J STD AIDS Nov. 2003; 14(11): 770–775.
Cooper HL, Bossak B, Tempalski B, Des Jarlais DC, Friedman SR. Geographic approaches to quantifying the risk environment: drug-related law enforcement and access to syringe exchange programmes. Int J Drug Policy. 2009; 20(3): 217–226.
de Montigny L, Moudon AV, Leigh BC, Kim SY. A spatial analysis of the physical and social environmental correlates of discarded needles. Health Place. 2011; 17(3): 757–766.
Stopka TJ, Lutnick A, Wenger LD, Deriemer K, Geraghty EM, Kral AH. Demographic, risk, and spatial factors associated with over-the-counter syringe purchase among injection drug users. Am J Epidemiol. 2012; 176(1): 14–23.
Martinez AN, Mobley LR, Lorvick J, Novak SP, Lopez A, Kral AH. Spatial analysis of HIV positive injection drug users in San Francisco, 1987 to 2005. Int J Environ Res Public Health. 2014; 11(4): 3937–3955.
Fulcher C, Kaukinen C. Mapping and visualizing the location HIV service providers: an exploratory spatial analysis of Toronto neighborhoods. AIDS Care. 2005; 17(3): 386–396.
Kaukinen C, Fulcher C. Mapping the social demography and location of HIV services across Toronto neighbourhoods. Health Soc Care Community. 2006; 14(1): 37–48.
Heimer R, Barbour R, Shaboltas AV, Hoffman IF, Kozlov AP. Spatial distribution of HIV prevalence and incidence among injection drugs users in St Petersburg: implications for HIV transmission. AIDS. 2008; 22(1): 123–130.
Enteen L, Bauer J, McLean R, et al. Overdose prevention and naloxone prescription for opioid users in San Francisco. J Urban Health. 2010; 87(6): 931–941.
Rowe C, Santos GM, Vittinghoff E, Wheeler E, Davidson P, Coffin PO. Predictors of participant engagement and naloxone utilization in a community-based naloxone distribution program. Addiction. 2015; 110(8): 1301–1310.
Davidson PJ, McLean RL, Kral AH, Gleghorn AA, Edlin BR, Moss AR. Fatal heroin-related overdose in San Francisco, 1997–2000: a case for targeted intervention. J Urban Health. 2003; 80(2): 261–273.
Visconti AJ, Santos GM, Lemos NP, Burke C, Coffin PO. Opioid overdose deaths in the city and county of San Francisco: prevalence, distribution, and disparities. J Urban Health. Jun 16 2015
City and County of San Francisco. Census 2010: census tracts for San Francisco (Zipped Shapefile Format); 2013
City and County of San Francisco. Streets of San Francisco (Zipped Shapefile Format); 2015
United States Census Bureau. B19083: Gini Index of Income Inequality. 2009–2013 5-Year American Community Survey. 2013
United States Census Bureau. S1903: median income in the past 12 months (in 2013 inflation-adjusted dollars). 2009–2013 5-Year American Community Survey. 2013
San Francisco Police Department Crime Incident Reporting System. SFPD Incidents—from 1 January 2003; 2015
United States Census Bureau. P3: race. 2010 Census Summary File 1. 2010
United States Census Bureau. P1: total population. 2010 Census Summary File 1. 2010
Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981; 19(2): 127–140.
Rockwell R, Des Jarlais DC, Friedman SR, Perlis TE, Paone D. Geographic proximity, policy and utilization of syringe exchange programmes. AIDS Care. 1999; 11(4): 437–442.
Church RL, ReVelle CS. The maximal covering location problem. Papers of the Regional Science Association. 1974; 32: 101–118.
Zaller ND, Yokell MA, Green TC, Gaggin J, Case P. The feasibility of pharmacy-based naloxone distribution interventions: a qualitative study with injection drug users and pharmacy staff in Rhode Island. Subst Use Misuse. 2013; 48(8): 590–599.
Rose VJ, Lutnick A, Kral AH. Feasibility of providing interventions for injection drug users in pharmacy settings: a case study among San Francisco pharmacists. J Psychoactive Drugs. 2014; 46(3): 226–232.
Green TC, Dauria EF, Bratberg J, Davis CS, Walley AY. Orienting patients to greater opioid safety: models of community pharmacy-based naloxone. Harm Reduct J. 2015; 12: 25.
Binswanger IA, Koester S, Mueller SR, Gardner E, Goddard K, Glanz J. Abstract #53: Overdose education and naloxone for patients prescribed opioids in primary care: a qualitative study. Paper presented at: College on Problems of Drug Dependence 77th Annual Meeting, 2015; Phoenix Arizona
Drainoni M, Ellison J, Koppelman E, et al. Abstract #167: Implementing routine emergency department naloxone rescue kits for patients at risk of opioid overdose. Paper presented at: College on Problems of Drug Dependence 77th Annual Meeting, 2015; Phoenix, Arizona
Acknowledgments
This study was supported by funding from the National Institutes of Health (NIDA R03 DA038084). Authors would like to acknowledge those who participated in the establishment and early conduct of the DOPE Project, including Pete Morse, Rachel McClean, Emalie Huriaux, Lauren Enteen, and Alex Kral, as well as medical director Josh Bamberger.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclaimer
The authors are solely responsible for the content of this article, which does not necessarily represent the official views of the San Francisco Department of Public Health
Rights and permissions
About this article

Cite this article
Rowe, C., Santos, GM., Vittinghoff, E. et al. Neighborhood-Level and Spatial Characteristics Associated with Lay Naloxone Reversal Events and Opioid Overdose Deaths. J Urban Health 93, 117–130 (2016). https://doi.org/10.1007/s11524-015-0023-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-015-0023-8