
Abstract
The literature on development has focused on the concept of transition in understanding the emergent challenges facing poor but rapidly developing countries. Scholars have focused extensively on the health and urban transitions associated with this change and, in particular, its use for understanding emerging infectious diseases. However, few have developed explicit empirical measures to quantify the extent to which a transitions focus is useful for theory, policy, and practice. Using open source data on avian influenza in 2004 and 2005 and the Vietnam Census of Population and Housing, this paper introduces the Kuznets curve as a tool for empirically estimating transition and disease. Findings suggest that the Kuznets curve is a viable tool for empirically assessing the role of transitional dynamics in the emergence of new infectious diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The Health and Urban Transitions: Applications to Emerging Infectious Diseases
Among public health scholars, one of the main concerns with rapid urban and economic development has been called a “health transition,”,17 during which societies undergoing rapid development face a dangerous period. As economic opportunity, land use, and household demands intensify, traditional illnesses remain present, even as new ones emerge. The importance of such rapid socioeconomic, environmental, and biological change on the transformation of human health risk has, in part, led interdisciplinary teams of scholars to focus on urbanization and health3,14: 270, 11, with particular relevance to the rapidly industrializing areas of Southeast Asia as major challenges facing planners and policymakers.
Concurrent with this focus on a health transition, scholars of urbanization have identified an urban transition (e.g.,4,5,8,24), a period of confusion and relative instability between states of stability regarding the economy, society, and politics. Periurban settlements are the spatial manifestation of these transitional urban shifts, and scholars have described the urban dynamics of emerging city neighborhoods where informal rules apply and informal institutions dominate as societies shift from rural to urban and from agriculture to industry 19,21.
Combining this literature on health and urban transitions, a growing focus of scholars has recently been on emerging infectious diseases, such as the reemergence of dengue fever and the evolution of new strains of avian influenza, in areas undergoing rapid and unplanned urbanization.6,7,9,25–27 Despite such innovative arguments, empirical evidence on the role of urban transition in the emergence of new infectious diseases is scant. This paper helps to fill this gap, using the case of avian influenza outbreaks in Vietnam during the disease’s initial outbreaks in 2004 and 2005.
Avian Influenza in Vietnam
As of May 21, 2005, at least 52 people had died of the H5N1 version of avian influenza: 36 in Vietnam, 12 in Thailand, and four in Cambodia. Of those 52 fatalities, 50 were infected through direct contact with diseased chickens or ducks. Only two were infected through direct human–human contact, and in these few cases, the virus was transmitted by intimate, daily contact between family members.23 Thus, there were no cases of human–human transmission of the disease through casual contact, and a feared global pandemic never emerged. Nevertheless, a threat of an avian influenza pandemic remains despite the fact that there appear to be few grounded and actionable policies to mitigate this risk. Because of the potentially severe consequences of even a low risk avian influenza scenario, this very real threat has generated extensive debate and concern among scholars, officials, and the general public about how to deal with the H5N1 epidemic, should it come to pass, and research on vaccines for the possible human virus have commenced.16
One of the primary limitations in developing steps to mitigate the risk of future H5N1 outbreaks is a lack of analysis of the disease’s origins. In general, scientists worry that a resistant human flu will develop from H5N1 reassorting with a human influenza virus22 or possibly reassorting with a pig flu virus and then with a human flu virus to create the resistant human strain.16 Footnote 1 A person infected with a human flu that is easily transmissible from human to human, if he becomes infected with an avian flu, provides the ideal biotic environment for a flu strain that is both resistant to human immune systems and easily spread among the human population. If this happens, a flu pandemic will be hard to stop. Virulogic surveillance suggests, statistically, that these situations have existed in Asia for some time,16,22 and some research has commenced on the conditions under which such reassortment might happen.22
Specifically, Kapan et al.7 have hypothesized that risk increases as contact with formerly dispersed farm environments that include potentially infected poultry and swine populations come into close contact with ever-denser human populations living in periurban regions. Such urban–rural interfaces have been hotspots of other infectious diseases, such as leishmaniasis,15 and it is even believed that similar wild population/human interfaces are the origins of the HIV/AIDS epidemic. Expanding fronts of human settlement, intensified agriculture, conversion of land use from rural to urban/industrial, and societal/cultural changes from government stability to family structure13 can increase the risk of such emerging infectious diseases.
These ecological and landscape changes associated with the conversion of rural environments into periurban regions is enabled by a governance structure in transition as well as by the intensification of a regional food processing industry. While individuals and households can be competent individual negotiators of these changes, in a new, periurbanized economic, governance and environmental context, they are understandably less attentive to take steps that preserve societywide human security beyond the household. Studies from elsewhere in Southeast Asia suggest that rural residents of the city face a lag time during which they must adapt sociocultural practices to new physical and social environments.2
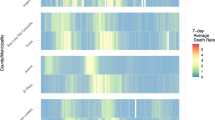
Vietnam is an excellent case study for empirically investigating the spatial phenomenon of urban transition and its relationship to H5N1. Figure 1 provides an overview of outbreaks in Vietnam during the 24 months covering 2004 and 2005, the initial major period of avian influenza. It is clear that areas surrounding the two major urban centers of Ha Noi and Ho Chi Minh cities were disproportionately affected by outbreaks, but the investigation below specifies precisely the relationship between urbanization and outbreaks in Vietnam.
Modeling an Urban Health Kuznets Curve: Settlement Coherence
While it has already been useful as a broad conceptual tool, the concept of an urban transition has remained largely theoretical and qualitative in nature. However, the possible empirical significance of transitional dynamics in spatially identifying emerging health challenges is great. In this paper, I take inspiration from Simon Kuznets,12 who has been influential in proposing that the economic development process is nonlinear with respect to economic inequality. In general, Kuznets’ hypothesis and supporting evidence argued that economic development was a transition from an initial state of relative equality to an end state, also of relative equality. Nation states in the middle of the economic development process, he went on to argue, displayed high levels of economic inequality.
Important critiques to this hypothesis suggesting that some unequal nations were permanently stuck in a transitional state between two states of equilibrium did not undermine the basic idea that inequality was nonlinear but predictable. This powerful idea was later adapted to environmental questions, suggesting that many environmental problems are at their worst in midlevel states of economic development,10 and the general idea of economic development and “transitional” states, called the Kuznets curve, has become a simple but elegant heuristic for empirically testing hypotheses about nonlinear change.
In the decades since the hypothesis first gained acceptance, the method has not been applied to urban development issues or to emerging infectious disease challenges. The balance of this paper applies the Kuznets method to the urban transition in Vietnam and the Mekong Delta where the prevalence of the avian influenza has been particularly high. In describing issues of settlement transition rather than economic development transitions, I develop a distinct method focused on urbanization and settlement that can help to geographically identify environmental health risks. The main advancement of the method over the original Kuznets model is that the explanatory factor is not “development” broadly defined, as in the economic inequality and environmental quality Kuznets curves. Rather, I introduce the concept of “settlement coherence” as a significant predictor of emerging infectious disease.
Vietnam is a particularly important area for examining settlement coherence, which is a rough measure of the degree of land conversion, urbanization, and environmental transformation that are simultaneously occurring,4 as traditional agricultural lands are reshaped into more formalized urban settlements to provide for increasing material demands of the population. While the empirical work presented here is on Vietnam, findings have potentially significant implications for other regions of Southeast Asia and the world, in particular Sub-Saharan Africa, in which societies are currently transitioning from agrarian to urban ones.
An Empirical Test of Avian Influenza Outbreaks and Settlement Coherence
This study brings together spatial and spatially referenced data to empirically explore the urban transition Kuznets curve. The first step required for developing an urban transition Kuznets curve is to match spatially referenced data on H5N1 poultry outbreaks with a measure of urban transition. One of the conventional definitions of urbanization is as the level of infrastructure able to manage all of the negative externalities associated with denser living. Thus, my urbanization measure is that of the “mixing” of different types of household-level infrastructure, including water supply, sanitation, and housing construction materials, as an area transitions from one kind of settlement to another. I term this measure of mixing “coherence.” These coherence measures are then tested against outbreaks for a Kuznets relationship.
Data and Methods: Spatial Units of Analysis, Provincial Outbreak Burden, and Sociospatial Coherence
Administratively, Vietnam is comprised of small-scale governmental units called districts. In general, several districts comprise a province, and there are 61 provinces in the country. Through an exhaustive search, Butler1 has compiled a global geographic database of H5N1 outbreaks among poultry and humans and made them available through Google Earth. For Vietnam, these data have been compiled at the district level. The overall dataset is described in detail in Butler.1 This study uses the data for outbreaks documented during each 4-month period in 2004 and 2005, a very active period for the disease in Vietnam. The data extracted from this file includes information on the number of poultry at risk, the total number of cases, number of deaths, and the number of birds destroyed. It also includes the district in which each outbreak occurred by start date. From this file, I created a measure of “Outbreak Burden '04–'05.” This provincial-scale measure is defined as the percentage of each province’s total districts which experienced an outbreak in either 2004 or 2005.Footnote 2
To construct an empirical Kuznets curve of the urban transition, I also developed a set of indices of settlement coherence based on household-level infrastructure and amenities. Vietnam’s 1999 Census of Population and Housing provides an excellent starting point for assessing the urbanization characteristics at the district level. First, settlement density patterns and human proximity has long been associated with increased risk of disease transmission, making dense settlements higher risk for the emergence of new diseases for which there is little human immunity. On the other hand, settlement infrastructure is an important control on disease risk where consistent and clean sources of water and sanitation as well as good electricity and housing stock can significantly reduce the risks associated with urbanization through frequent washing, minimization of standing water, and temperature control, for example. Thus, any index of risk for emerging infectious disease, such as H5N1, must accurately estimate transitional or periurban areas as distinct from both highly urban and highly rural areas. According to the hypothesis, the former is high risk and the latter two, low risk. I characterize the two ends of this measure as “modern coherence” for highly urbanized areas and “traditional coherence” for highly rural and subsistence-oriented areas.
One of the first changes in the physical environment—or “disturbances” to an existing state of relative equilibrium—as urbanization and population density increases is the construction of housing, closely followed by the provision of water, and then later by sanitation systems. These three measures of urbanization and residents’ ability to manage population concentration form the bases of my settlement coherence index. The argument is that this index roughly measures a location’s physical change in which the risk of environmentally generated diseases increases and then decreases following a symmetric pathway in which the center represents the highest risk and the two end points of the pathway represent the lowest risks. My argument is that each of these extremes has evolved familiar physical and social mechanisms to minimize risks of disease. Those relatively “incoherent” physical settlements falling in the middle portions of the index are areas in which the built environment and social practices have not yet developed effective ways to control emerging infectious diseases.
The 1999 Vietnam Census of Population and Housing file includes district-level counts of households with improved housing construction materials, improved water supply, and improved sanitation infrastructure. These three variables are the basis for four measures of urban settlement coherence centered on (1) housing materials, (2) water supply, (3) sanitation, and (4) a composite index of all three measures. Each of these three indices is centered on a value of “0”, which signifies incoherent or periurban settlement patterns hypothesized to be at high risk of disease emergence. High positive values indicate provinces dominated by “modern coherence” settlement patterns, and extreme negative values indicate provinces dominated by “traditional coherence” settlement patterns. The Appendix specifies how these indices were constructed.
Limitations of the Study
As with most empirical models, choices about data and methods present a number of limitations on the analysis to be considered. First, using a bivariate analysis to explore transitional settlement environments does not imply causality. Any possible relationship between the measure of settlement coherence and disease outbreak need not suggest that settlement patterns cause outbreaks, but only that they are associated with them. Further studies should conduct multivariate models that build on any correlations. Given the small dataset, the bivariate relationship’s primary intention is not to statistically estimate the strength of the relationship between settlement coherence and disease burden but primarily to illustrate the concept of urban transitions and its utility in analyzing emerging infectious disease. In this way, the study is exploratory and, depending on the preliminary findings, might justify being followed up with more rigorous statistical analysis. Using secondary data collected on avian influenza and on the population and housing characteristics of Vietnam presents choices regarding the variables of interest and the time element of the analysis, since the variables available in these datasets are limited. Fortunately, for the purposes of this study, there were a number of variables relevant to the hypothesis of an urban transition related to water, sanitation, and housing characteristics. These measures relate to the physical aspects of an urban transition but are, by no means, comprehensive. Thus, any findings about the relationship between disease outbreak and settlement coherence are generally limited to these aspects of the urban transition.
Finally, the time lag between the two datasets used here allows only a partial answer to the basic question. Kapan et al.7 divide landscape changes and effects on H5N1 into short- and long-term factors. Given the 5-year time lag between the hypothesized cause, urban transition, and the hypothesized effect, H5N1, this analysis is only able to speak to the long-term effect of urban transition on health risk. Despite these limitations, the gap in the literature on empirical estimations of the urban transition suggests that findings generated from these models will shed new light on a theoretical concept that has been usefully debated in the literature but never operationalized.
Findings
An examination of the full dataset, all 61 provinces, shows no apparent Kuznets relationship between outbreaks and settlement coherence at the province level. Figure 2 presents the four indices of urban transition plotted against provincial outbreak burdens. The figure shows a regression line with a cubic function, since this mathematical function for fitting the curve to the data is more accurate than either a quadratic or linear function. Thus, for building coherence, the defined levels of settlement coherence explain roughly 34.4 % (r 2 = 0.344) of the H5N1 outbreak burden levels. The strongest predictor of H5N1 outbreaks, however, is the water supply coherence index which predicts with almost 50 % accuracy (r 2 = 0.453) the level of outbreak expected based on knowledge of settlement coherence.

HPAI incidence in Vietnam by district in 2004 and 2005.

Coherence indices and avian influenza: building materials, water supplies, sanitation, and composite (complete dataset).
None of the curves presented in Figure 2 follows a neat Kuznets shape. However, this result occurs because most occurrences of H5N1 happened in districts that are overwhelmingly closer to “traditional coherence,” even though these places do not necessarily have the highest levels of outbreak burdens. For the three primary indicators, building construction materials, water supply, and sanitation, approximately half of all outbreaks in 2004 and 2005 occurred in provinces that were extremely undeveloped with respect to household-level infrastructure. In other words, half of the outbreaks occurred in provinces where the local diversity of these household infrastructure showed, for example, greater than 90 % temporary structures, 90 % “other” water sources, or 90 % no toilet. This finding is not surprising given that these are the areas least able to address fast-moving epidemics in the poultry population. More interesting to those concerned with emerging health risk and the impact of development, however, is the pattern found among those district-level settlements that have already begun to make a significant shift from “traditional” to “modern.” In other words, very small increases in more modern household infrastructure are not likely to have much impact, but moderate to large ones may have larger impact.
A closer interpretation of the indices based on this logic, however, does show that the urban transition is likely an important predictor of emerging infectious disease risk. For each coherence index, one of the two possible maximum risk values lies at or close to the “0” score on the coherence index, a sign that risk is greater where coherence is lowest. In other words, after “traditional coherence” begins to be disrupted to a point where fewer than 90 % of structures are temporary, fewer than 90 % of household water sources are “other” (usually a household-level mix of bottled and natural sources) water sources, and fewer than 90 % of households have no toilet, increasing settlement incoherence is associated with much higher rates of outbreak. Similarly, when each index approaches “modern coherence,” the likelihood of outbreak at the provincial level drops significantly.
Splitting each cubic graph into two quadratic graphs can help us to understand the urban transition.Footnote 3 In other words, it can help us to understand the relationship between the urban transition and outbreaks once settlement incoherence reaches critical points. Based on the graphs, one can assert that there are critical points at the 90 % coherent mark, of either the “traditional” or the “modern” type, where the cubic version of the fitted line has two nadirs, one at −0.40 and one at 0.40 on the water supply and sanitation urban transition indices.
Figure 3 presents the split pairs of fitted curves for each urban transition index using two quadratic functions separated at the first nadir (−0.40), the point at which settlement coherence appears to become important. In particular, the water supply coherence and sanitation indices appear precisely as hypothesized by a Kuznets relationship between the 90 %–90 % values marked by −0.40 and 0.40. It is important also to note that the r 2 values for the 90 %–90 % range fitted line explain more of the variation than does the line fitted for the extreme low values greater than 90 % traditional coherence (i.e., below the −0.40 value). This is particularly the case for water supply where the urban transition index explains over 50 % of the outbreak risk, while the extremely low (traditional) coherence part of the curve explains only 28.3 % (not presented here). The transitional aspects of construction coherence as measured by the building coherence index, importantly, does not match with the theory of an urban settlement transition, though not enough to distort the nature of the Kuznets relationship when all three aspects of household infrastructure are combined in the composite index.

Coherence indices and avian influenza: building materials, water supplies, sanitation, and composite (90–90 split curves).
Overall, the findings strongly suggest that, at the national level, transitional dynamics in household-level infrastructure are associated with avian influenza outbreaks and may be used as a general predictor of emerging infectious disease risk. In particular, the urban transition of household water and sanitation infrastructure seem to be important correlates of outbreaks at the provincial level.
Implications of the Urban Kuznets Curve: Future Risk in the Mekong Delta
Spencer20 has described the growing process of urbanization and an increasing conflict between the pressures of economic development and natural resources in the Mekong Delta. A regional examination of the urban health transition curve suggests that the Mekong Delta region is likely to face the greatest threat of H5N1 outbreaks as it develops economically, and settlement patterns grow increasingly incoherent before they may possibly reach a fully modern equilibrium. For example, Figure 4 shows that no outbreaks occurred in a Mekong Delta province with greater than −0.40 coherence, which is largely because there are no provinces beyond the center (maximum incoherence) of the building coherence index. Outbreaks occurred in provinces slightly closer to the center (maximum incoherence) on the water supply and sanitation indices, but there still remain no modern coherent provinces in the Mekong Delta. Overall, for the Mekong Delta, the regional nadir of water, for example, of (−0.30) is closer to the complete incoherence point than the national average of (−0.47). This shift in the curve is similar to that for sanitation. For the Red River Delta (Figure 5), it is similarly shifted closer to the 0 point than the national average for water and for sanitation. These findings suggest also that the river deltas have compressed settlement transitions when compared to mountainous and coastal regions, consistent with the idea that the urban transition is compressed in the main river delta regions. While promising, on the one hand, because it means that the period between traditional coherence and modern coherence may be shorter, it is a bit concerning because it suggests that the appearance of new health challenges may appear more quickly and suddenly in these regions than elsewhere.

Mekong Delta coherence indices and avian influenza: building materials, water supplies, sanitation, and composite (complete dataset).

Red River Delta coherence indices and avian influenza: building materials, water supplies, sanitation, and composite (complete dataset).
The second important point revealed through the comparison is that the Mekong Delta, unlike the Red River Delta, is very early in its urban transition. Regarding the two more important transition indicators, water supply and sanitation, no provinces in the region have achieved a value of even roughly −0.10 on water supply or even −0.25 on the sanitation index. Taking the greater south region (Figure 6) into account to provide more cases of modern coherence, the curves for water supply and sanitation show a similar pattern to the national norm, even though there are no cases of modern coherence beyond Ho Chi Minh City itself. Thus, the Mekong Delta has very low rates of urbanization comparatively, but all indicators, the relationship between urban transition and health risk in this region, are very similar to the national and Red River Delta picture. In short, the Mekong Delta is likely to urbanize the most, and the most rapidly over the coming years, and it has yet to approach the urbanization stages of the highest risk indicated by 0 scores (maximum incoherence) on the water supply and sanitation coherence indices.

Greater south coherence indices and avian influenza: building materials, water supplies, sanitation, and composite (complete dataset).
Concluding Thoughts and Implications
While many scholars have discussed the qualitative aspects of the urban transition in developing countries, Southeast Asia, and in particular Vietnam, none have attempted to model such nonlinear dynamics in relation to emerging infectious diseases. The societal changes implied by the term have remained virtually invisible to the policy debate because there have been few models for systematically estimating such a transition. Without a model to estimate transitional dynamics, it is difficult to fully understand the relationship between urbanization, development, and the host of health18 and social5 challenges that have been hypothesized in the literature.
The case of avian influenza provides an excellent example of the hypothesized impact of urban transition on emerging infectious diseases like H5N1. Empirically and precisely defining the relationship between a new urban transition index and H5N1 outbreaks in Vietnam using a Kuznets curve-base model can provide policymakers with tools for identifying those regions most at risk, and when they are most at risk of emerging infectious disease.
The empirical results of the study suggest that settlement incoherence with regard to water supply is associated with outbreaks of avian influenza, as is sanitation settlement incoherence. Moreover, the construction materials used for constructing housing seems not to be an important predictor of H5N1 outbreaks.
The analysis presented here also suggests that three conditions place the Mekong Delta region of Vietnam at particular risk. First, the region has yet to approach the peak period of urban transition, and most of its settlement transformation lies ahead, assuming it continues along a similar development pathway. Second, when one considers the greater southern region of Vietnam, which does include modern, urbanized regions, the relationship between the urban transition and health risk is identical to the national picture where settlement incoherence with respect to water and sanitation maximizes outbreak risk. Finally, evidence from both the Red River Delta and the Mekong Delta suggest that the range of the highest risk during the urban transition is compressed, compared to the rest of the country. These conditions strongly suggest that to the greatest degree in Vietnam, the Mekong Delta is the region with the most transitioning from agrarian societies to an urban one in the future; that environmental health risk will evolve similarly to how it has throughout the rest of the country; and that though it will be shorter than other regions, it will also become apparent more quickly and, therefore, is likely to be more surprising unless strong surveillance and preventative measures are taken.
As important as the findings above, this analysis provides a platform for further empirical work on how urban transitional dynamics may be at the heart of emerging infectious diseases. Scholars should advance the methods described here by focusing on three new areas. First, as a binary analysis, the data discussed above describes correlations that may become spurious once controlled for other factors, such as poultry levels, education, and development, for example. Such variables are certainly related to outbreaks, but the key question here is whether the coherence indices remain significant predictors. Second, because outbreak data are only available at the district level, the analysis must be conducted at the next highest level of spatial aggregation, the province level, where outbreak ratios can be calculated into metric values. Because of this data limitation, the measure of coherence is calculated at the provincial level, even though this may not be the most relevant spatial scale. Finally, the issue of timing must be better resolved. While some scholars (e.g.,25) suggest that urbanization’s effects on emerging infectious disease operates at the “landscape” level—an assertion supportive of both the provincial geography used here as well as the combination of Census 1999 data matched with outbreak data from 2004/2005—, it is possible that both results will vary by spatial scale and/or by temporal lag time between hypothesized “cause” and “effect.” Future studies would usefully address these limitations.
Notes
In addition to reassortment, scientists believe that evolutionary drift may also explain the emergence of H5N1. This paper focuses on the former, which is of most relevance to urban and spatial scholars of health.
It is important to note that I use the presence of an outbreak rather than the number of affected poultry, which is also present in the original data source. First, the data itself showed vastly differing values for these numbers, ranging from below 10 to over 200,000 dead birds. While it is certainly possible that these numbers are accurate, using them introduces a potential source of error not necessary for this analysis. As importantly, the hypothesis assessed here is regarding the factors that give rise to an outbreak more so than the factors determining the severity of any given outbreak. The number of dead poultry reflects the human ability to respond to any given outbreak (or efforts to avoid responding) as much as it does the source of why the outbreak occurred in the first place.
Because a quadratic fit to the data will, by definition, result in either a Kuznets or an inverse Kuznets curve, results should be interpreted based on the degree to which the resulting curve fits the hypothesized Kuznets. In particular, the steepness of the curve’s two slopes and the overall r 2 value fit are important.
References
Butler D. Mashups mix data into global service. Nature. 2006; 439: 6–7.
Bunnell T. Kampung rules: landscape and the contested government of urban(e) Malayness. Urban Studies. 2002; 39(9): 1686–1701.
Costa CH, Werneck GL, Rodrigues L Jr, Santos MV, Araújo IB, Moura LS, Moreira S, Gomes RB, Lima SS. Household structure and urban services: neglected targets in the control of visceral leishmaniasis. Ann Trop Med Parasitol. 2005; 99(3): 229–236.
Douglass M. From global intercity competition to cooperation for livable cities and economic resilience in Pacific Asia. Environ Urban. 2002; 14(1): 53–68.
Friedmann J. China’s urban transition. Minneapolis: University of Minnesota Press; 2005.
Gubler DJ. The global emergence/resurgence of arboviral diseases as public health problems. Arch Med Res. 2002; 33: 330–342.
Kapan DD, Bennett SN, Ellis B, Fox J, Lewis ND, Spencer JH, Saksena S, Wilcox BA. Avian influenza (H5N1) and the evolutionary and social ecology of infectious disease emergence. EcoHealth. 2006; 3(3).
Kessides C. The urban transition in sub-Saharan Africa: implications for economic growth and poverty reduction. Washington, DC: Cities Alliance; 2006.
King DA, Peckham C, Waage JK, Brownlie J, Woolhouse MEJ. Epidemiology: infectious diseases: preparing for the future. Science. 2006; 313(5792): 1392–1393.
Kijima M, Nishide K, Ohyama A. Economic models for the environmental Kuznets curve: a survey. J Econ Dyn Control. 2010; 34(7): 1187–1201.
Knudsen, Slooff. Vector-borne disease problems in rapid urbanization: new approaches to vector control. Bull World Health Organ. 1992; 70(1): 1–6.
Kuznets S. Economic growth and income inequality. Am Econ Rev. 1955; 45(1): 1–28.
Lambin EF, Geist H, Lepers E. Dynamics of land use and cover change in tropical regions. Annu Rev Env Resour. 2003; 28:205–241.
Montgomery MR, Stren R, Cohen B, Reed HE, eds. Cities transformed: demographic change and its implications in the developing world. London: Earthscan; 2004.
Oliveira CCG, Lacerda HG, Martins DRM, Barbosa JDA, Monteiro GR, Queiroz JW, Sousa JMA, Ximenes MFFM, Jeronimo SMB. Changing epidemiology of American cutaneous leishmaniasis (ACL) in Brazil: a disease of the urban–rural interface. Acta Trop. 2004; 90(2): 155–162.
Osterholm MT. Preparing for the next pandemic. N Engl J Med. 2005; 352: 1839–1842.
Smith KR. Development, health, and the environmental risk transition. In: Shahi G, Levy BS, Binger A, Kjellstrom T, Lawrence R, eds. International perspectives in environment, development, and health. New York: Springer; 1997: 51–62.
Smith KR, Ezzati M. How environmental health risks change with development: the epidemiologic and environmental risk transitions revisited. Annu Rev Environ Resour. 2005; 30: 291–333.
Special Journal Issue. Becoming urban: periurban dynamics in Vietnam and China. Pacific Affairs. 2011; 83(3): 425–534.
Spencer JH. Health, human security and the peri-urban transition in the Mekong Delta: market reform, governance and new analytic frameworks for research in Southeast Asia. Int J Asia-Pacific Stud. 2007; 3(2): 43–64.
Spencer JH, Guzinsky C. Periurbanization, public finance, and local governance of the environment: lessons from small-scale water suppliers in Gresik, Indonesia. Environ Plann. 2010; 42(9): 2131–2146.
Stöhr K. Avian influenza and pandemics—research needs and opportunities. N Engl J Med. 2005; 352: 405–407.
Ungchusak K, Auewarakul P, Dowell SF, et al. Probable person-to-person transmission of avian influenza A (H5N1). N Engl J Med. 2005; 352: 333–340.
Waibel M. The production of urban space in Vietnam’s metropolis in the course of transition: internationalization, polarization, and newly-emerging lifestyles in Vietnamese society. Trialog. 2006; 89(2).
Wilcox BA, Colwell RR. Emerging and re-emerging infectious diseases: biocomplexity as an interdisciplinary paradigm. EcoHealth. 2005; 2(4): 244–257.
Wilcox BA, Gubler DJ. Disease ecology and the global emergence of zoonotic pathogens. Environ Health Prev Med. 2005; 10(5): 263–72.
Wilcox Bruce A, Gubler D, Pizer HF. Urbanization and the social ecology of emerging infectious diseases. In: Mayer KH, Pizer HF, eds. Social ecology of infectious diseases. Boston: Elsevier/Academic Press; 2007: 113–37.
Acknowledgement
The author would like to thank the East West Center’s Research Program, in particular John Vogler and Nancy Lewis, and ISCA Technologies for assistance in assembling the data. The research is associated with National Science Foundation Award #0909410. All factual and analytic errors, of course, are the author’s own.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
The Census file includes district-level counts of households with improved housing construction materials, improved water supply, and improved sanitation infrastructure. These three variables are the basis for four measures of urban settlement coherence centered on (1) housing materials, (2) water supply, (3) sanitation, and (4) a composite index of all three measures. In general, each of these four indices are centered on a value of “0,” which signifies perfect incoherence or periurban settlement patterns hypothesized to be at very high risk of disease emergence. High positive values indicate provinces dominated by “modern coherence” settlement patterns, and extreme negative values indicate provinces dominated by “traditional coherence” settlement patterns.
Technically, my index of settlement coherence converts four ranked responses contained within the Census data into a metric variable symmetric around the zero value. Specifically, using the example of water supply source:
where:
- X 1 :
-
percentage of households using running tap water as their main source
- X 2 :
-
percentage of households using well water as their main source
- X 3 :
-
percentage of households using rain water as their main source
- X 4 :
-
percentage of households using other water (a combination of surface water and bottled water) as their main source.
The four categories of household building materials and sanitation systems are organized similarly into rank-order classes, and the same steps are repeated using each of those four categories to construct these two indices. Finally, the dependent variable of outbreak burden for a province that is plotted on the y-axis is estimated by:
Displaying the relationship between outbreak burden during 2004 and 2005 and the various settlement coherence indices, therefore, defines the relationship between the urban transition and the emergence of H5N1.
Rights and permissions
About this article
Cite this article
Spencer, J.H. The Urban Health Transition Hypothesis: Empirical Evidence of an Avian Influenza Kuznets Curve in Vietnam?. J Urban Health 90, 343–357 (2013). https://doi.org/10.1007/s11524-012-9719-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-012-9719-1