
Abstract
We sought to describe: (1) the prevalence of internet, cellular phone, and text message use among women attending an urban sexually transmitted infections (STI) clinic, (2) the acceptability of health advice by each mode of information and communication technology (ICT), and (3) demographic characteristics associated with ICT use. This study is a cross-sectional survey of 200 English-speaking women presenting to a Baltimore City STI clinic with STI complaints. Participants completed a self-administered survey querying ICT use and demographic characteristics. Three separate questions asked about interest in receiving health advice delivered by the three modalities: internet, cellular phone, and text message. We performed logistic regression to examine how demographic factors (age, race, and education) are associated with likelihood of using each modality. The median age of respondents was 27 years; 87% were African American, and 71% had a high school diploma. The rate of any internet use was 80%; 31% reported daily use; 16% reported weekly use; and 32% reported less frequent use. Almost all respondents (93%) reported cellular phone use, and 79% used text messaging. Acceptability of health advice by each of the three modalities was about 60%. In multivariate analysis, higher education and younger age were associated with internet use, text messaging, and cellular phone use. Overall rate of internet use was high, but there was an educational disparity in internet use. Cellular phone use was almost universal in this sample. All three modalities were equally acceptable forms of health communication. Describing baseline ICT access and the acceptability of health advice via ICT, as we have done, is one step toward determining the feasibility of ICT-delivered health interventions in urban populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Heterosexual transmission of HIV is increasing among women in the United States. Unprotected sexual activity and sex with high-risk partners are associated with increased risk of HIV.1 Effective health interventions targeting risky behaviors among women visiting sexually transmitted infections (STI) clinics may curb HIV transmission.
Information and communication technology (ICT) for the delivery of behavioral health interventions has shown promising results.2–6 While this strategy has the potential for low-cost widespread dissemination, access to ICT among certain groups such as urban women at high risk for HIV infection is variable. Characterizing ICT use is the first step in determining whether delivering interventions via these modalities is feasible.
We sought to describe: (1) the prevalence of internet, cellular phone, and text message use among women attending an urban STI clinic; (2) the acceptability of health interventions by each of the three modalities; and (3) demographic characteristics associated with ICT use in this sample. We hypothesized that internet use would be associated with younger age and higher education.
Methods
This was a cross-sectional survey of 200 English-speaking women presenting to a Baltimore City STI clinic with STI complaints conducted during August 2008. Participants completed a 15-minute, self-administered survey querying internet, cellular phone, and text message use and interest in receiving health advice by each of the three modalities. Oral informed consent was obtained. Participants received a five-dollar gift card as compensation for their time. The institutional review boards of the Johns Hopkins University School of Medicine and the Baltimore City Health Department approved this study.
Our independent variables of interest included: (1) education, categorized as grades 6–12, high school diploma/GED, “some college”, or “other”; (2) race categorized into African American or Non-African American; and (3) age, dichotomized at the median. ICT use was assessed with the following three questions: (a) “How often do you use the internet? (1) Never, (2) once per month, (3) <1 day per week, (4) 1–6 days per week, (5) daily”; (b) “Do you use a cellular phone? Yes or No”; and (c) “Do you send or receive text messages? Yes or No”. Three separate questions asked whether the participant would be interested in receiving health advice delivered by each of the three modalities (e.g., “If it was free for you (no cellular phone or clinic charge), would you like to receive health advice on your cellular phone?”).
We determined the prevalence of internet use, cellular phone use, and text message use. We tabulated the number of respondents who would be interested in receiving health advice by each of the modalities. We performed logistic regression to assess how demographic factors (age, race, and education) were related to the likelihood of using each modality. Due to the high prevalence of ICT use, it was necessary to define the outcome as non-use. We also performed multivariate logistic regression: (1) to assess the effect size of each factor while controlling for the other factors and (2) to assess the association of demographic factors (age, race, and education) on the likelihood of acceptability of health advice via each modality.
Results
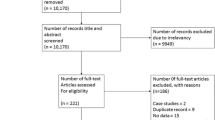
Characteristics of our sample are summarized in Table 1. One hundred ninety-one surveys had complete information and were used for the final analyses. The median age of respondents was 27 years (range 18–62 years), and 87% were African American. The majority of individuals surveyed (93%) reported cellular phone use and 79% used text messaging. The prevalence of any internet use was 80%; 31% reported daily use; 16% reported weekly use; and 32% reported less frequent use. Of 39 respondents who reported never using the internet, 79% used a cellular phone and 42% sent or received text messages. Sixty percent of respondents were interested in receiving health advice by each of the three modalities (results stratified by use shown in Table 2).
Multivariate analysis of factors associated with internet use revealed that individuals with an age above the median were three times more likely to not use the internet. In addition, higher educational attainment was inversely associated with being a non-user; in other words, those with higher education were more likely to use the internet (Table 3). We found similar multivariate associations with cellular phone and text messaging use. Age above the median [cellular phone: adjusted odds ratio (AOR) 5.74, 95% confidence interval (CI) 1.21–27.3, p = 0.028; text message: AOR 10.61, 95% CI 3.84–29.3, p < 0.001] was associated with not using a cellular phone or text messaging, and higher educational attainment (cellular phone: AOR 0.10, 95% CI 0.01–0.81, p = 0.032; text message: AOR 0.21, 95% CI 0.08–0.59, p = 0.003) was inversely associated with not using a cellular phone or text messaging. When multivariate regressions were performed for the acceptability of receiving health advice by each modality, no significant associations were found, with the exception that older age was associated with being less likely to express interest in receiving health advice via text message (AOR 0.45, 95% CI 0.24–0.82, p = 0.009).
Discussion
In this sample of urban women attending an STI clinic, the prevalence of internet use was higher than expected and significantly associated with higher educational attainment and younger age. Cellular phone use, however, was nearly ubiquitous and equally acceptable for receipt of health advice suggesting that cellular phones may be an appealing alternative to the internet for dissemination of health interventions.
The rate of internet use (80% overall) in our study is higher than that quoted in similar populations. Studies of similar populations conducted between 2000 and 2005 have reported internet use between 29%–52%; the difference is likely due to a steep increase in use since 2005 amongst all sectors of the population.7–9 This assertion is supported by the fact that national estimates of internet use have shown a steep increase over the past 5 years; US adults who ever or occasionally use the internet rose from 59% in 2004 to 73% in 2008.10 The rate of rise was paralleled amongst African Americans—45% in 2004 to 59% in 2008.10 Not surprisingly, we found that younger age was associated with internet use. We found a disparity by educational attainment which may preclude using the internet to reach high-risk groups. The 60% acceptability rate of health advice via internet is in accord with figures from a recent study in a Nashville community health clinic.11
Our finding of a 93% prevalence of cellular phone use in our sample is similar to recent national estimates, including a recent study that found 89% prevalence in the general population.12 Text message use, though associated with higher education and younger age in our sample, was overall higher than that in a national survey conducted by Pew, which asked respondents whether they use their cellular phone for text messaging.13 They found a 35% rate of text message use among cellular phone users compared with 79% in our sample. In the same survey, text messaging was reported by 65% of persons in the 18–29 age group and 37% in the 30–49 age group, as compared with our sample where we found a prevalence of 93% and 60%, respectively.13 Notably, the Pew survey surveyed 50% of their participants by cellular phone. Despite this, their estimates of text messaging were lower than our sample. Landline use is declining among low-income adults and youth, of which our sample was largely comprised, and being replaced by cellular phones. Thus, even with 50% cellular phone surveying, these national estimates may not represent our population.14
Behavioral interventions delivered via internet and cellular phone have demonstrated efficacy in smoking cessation, alcohol reduction, and weight loss.4,5,15–20 However, most of these studies have recruited college students and/or excluded those with low literacy. None, to our knowledge, have focused on urban, high-risk women. Recording complete contact information including cellular phone and texting capability has become increasingly important in this clinic for follow-up of positive test results. Thus, we sought to explore the feasibility of the cellular phone for interventions. It is critically important to determine access to ICT so that we might test efficacy in this group.
Limitations of this study include: (1) a cross-sectional design which limits our ability to make causal associations; (2) convenience sampling method which introduces bias; and (3) lack of generalizability except to other urban STI clinic populations which tend to be younger, more heavily female, and with a higher proportion of minorities than the general population. Of note, despite the convenience sampling method, the sample was representative of the Baltimore City STI clinic population with characteristics corresponding to a 2007 report summarizing the female population visiting both sites of the Baltimore City STI clinic (i.e., 21% of women visiting the clinic in 2007 were under 21 years of age, 90% were African American). Therefore, our sample reflects the population attending this STI clinic. Another limitation includes the use of the phrase “health advice” in our survey, which could be interpreted as either general health information or tailored health information. Finally, we do not know where the women access the internet (access at work or school may preclude health communication about sensitive issues) and we do not know the current purpose of their internet use.
Conclusion
Given the significant association of education, an indicator of socioeconomic status, with internet use, web-based interventions for urban women may serve to widen health disparities. Cellular phones, in contrast, are omnipresent among Baltimore City STI clinic attendees. Describing high rates of internet and cellular phone use and the acceptability of health advice via these methods, as we have done, is the first step toward designing effective behavioral interventions to reduce risky sexual behavior which contribute to the HIV epidemic.
References
Hutton HE, McCaul ME, Santora PB, Erbelding EJ. The relationship between recent alcohol use and sexual behaviors: gender differences among sexually transmitted disease clinic patients. Alcohol Clin Exp Res. 2008; 32(11): 2008-2015. Epub 6 Sep 2008.
Linke S, Murray E, Butler C, Wallace P. Internet-based interactive health intervention for the promotion of sensible drinking: patterns of use and potential impact on members of the general public. J Med Internet Res. 2007; 9(2): e10.
Riper H, Kramer J, Smit F, Conijn B, Schippers G, Cuijpers P. Web-based self-help for problem drinkers: a pragmatic randomized trial. Addiction. 2008; 103(2): 218-227.
Vidrine DJ, Arduino RC, Lazev AB, Gritz ER. A randomized trial of a proactive cellular telephone intervention for smokers living with HIV/AIDS. AIDS. 2006; 20(2): 253-260.
Rodgers A, Corbett T, Bramley D, Riddell T, Wills M, Lin RB. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005; 14(4): 255-261.
Levine D, McCright J, Dobkin L, Woodruff AJ, Klausner JD. SEXINFO: a sexual health text messaging service for San Francisco youth. Am J Public Health. 2008; 98(3): 393-395.
Rietmeijer CA, Bull SS, McFarlane M, Patnaik JL, Douglas JM Jr. Risks and benefits of the internet for populations at risk for sexually transmitted infections (STIs): results of an STI clinic survey. Sex Transm Dis. 2003; 30(1): 15-19.
Kalichman SC, Weinhardt L, Benotsch E, DiFonzo K, Luke W, Austin J. Internet access and internet use for health information among people living with HIV–AIDS. Patient Educ Couns. 2002; 46(2): 109-116.
Mayben JK, Giordano TP. Internet use among low-income persons recently diagnosed with HIV infection. AIDS Care. 2007; 19(9): 1182-1187.
U.S. Census Bureau, Statistical Abstract of the United States: 2009 (128th Edition) Washington, DC, 2008. Available at: http://www.census.gov/compendia/statab/cats/information_communications/internet_publishing_and_broadcasting_and_internet_usage.html. Accessed on: August 20, 2009.
Peterson NB, Dwyer KA, Mulvaney SA. Computer and internet use in a community health clinic population. Med Decis Making. 2009; 29(2): 202-206.
Harris Interactive. The Harris Poll #36, April 4, 2008. Available at: http://www.harrisinteractive.com/harris_poll/index.asp?PID=890. Accessed on: February 22, 2009.
Pew Internet & American Life Project. Pew Internet Project Data Memo. Available at: http://www.pewinternet.org/∼/media//Files/Reports/2006/PIP_Cell_phone_study.pdf. Accessed on: July 29, 2009.
Blumberg SJ, Luke JV. Reevaluating the need for concern regarding noncoverage bias in landline surveys. Am J Public Health. 2009; 99(10): 1806-1810.
Cunningham JA, Humphreys K, Koski-Jannes A, Cordingley J. Internet and paper self-help materials for problem drinking: is there an additive effect? Addict Behav. 2005; 30(8): 1517-1523.
Hester RK, Squires DD, Delaney HD. The Drinker’s Check-Up: 12-month outcomes of a controlled clinical trial of a stand-alone software program for problem drinkers. J Subst Abuse Treat. 2005; 28(2): 159-169.
Kypri K, Saunders JB, Williams SM, et al. Web-based screening and brief intervention for hazardous drinking: a double-blind randomized controlled trial. Addiction. 2004; 99(11): 1410-1417.
Neighbors C, Larimer ME, Lewis MA. Targeting misperceptions of descriptive drinking norms: efficacy of a computer-delivered personalized normative feedback intervention. J Consult Clin Psychol. 2004; 72(3): 434-447.
Weitzel JA, Bernhardt JM, Usdan S, Mays D, Glanz K. Using wireless handheld computers and tailored text messaging to reduce negative consequences of drinking alcohol. J Stud Alcohol Drugs. 2007; 68(4): 534-537.
Joo NS, Kim BT. Mobile phone short message service messaging for behaviour modification in a community-based weight control programme in Korea. J Telemed Telecare. 2007; 13(8): 416-420.
Acknowledgements
We would like to acknowledge the assistance of clinical informationist Blair Anton, MLIS, MS, at the Welch Medical Library of Johns Hopkins University School of Medicine.
A poster based on this study was presented at the 32nd Annual Meeting of the Society of General Internal Medicine, May 13–16, 2009, Miami Beach, FL.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Samal, L., Hutton, H.E., Erbelding, E.J. et al. Digital Divide: Variation in Internet and Cellular Phone Use among Women Attending an Urban Sexually Transmitted Infections Clinic. J Urban Health 87, 122–128 (2010). https://doi.org/10.1007/s11524-009-9415-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-009-9415-y