
Abstract
Asthma is a leading cause of hospitalizations, acute care utilization, health care costs, and school absences in children. Asthma morbidity is disproportionately high in inner city populations. In general, community-based public health interventions to reduce asthma morbidity have had modest success due in part to their limited reach and low participation by the targeted population. Adolescents have been especially difficult to reach. A coalition of community organizations developed a school-based, population-level system to identify, prioritize, and provide interventions for middle school children with asthma in a large urban school district in Oakland, CA. Nearly 92% (n = 8,326) of students in the targeted schools took an asthma case identification survey. Of those students who took the survey, 17.5% (n = 1,458) had active asthma and were eligible for services. Among those identified with active asthma, 83% (n = 1,217) voluntarily attended asthma self-management classes at school. The 4-week curriculum previously has been shown to significantly improve several indicators of asthma control in this population. Retention was high—72% of students who enrolled attended at least three of the four curriculum sessions. Many higher-risk students were subsequently referred to and enrolled in off-site asthma services. Large school districts with incomplete or inadequate health records, high asthma prevalence, and internal or external services available for students with asthma may benefit from a similar model. A system such as the one described may be an effective public health strategy for school districts, health departments, and community coalitions addressing asthma or other conditions with high childhood prevalence.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Asthma is one of the most common chronic diseases and is a leading cause of hospitalizations and emergency room visits among children and adolescents.1,2 In the U.S., the direct medical costs of asthma for school-aged children is over $1 billion per year with an additional $1 billion per year in indirect costs.3 Inner city and many minority populations suffer disproportionately from asthma prevalence and most indicators of asthma control.1,4–8
Asthma-related morbidity is largely preventable with appropriate medications, proper self-management skills, and the avoidance of triggers. Although the physician takes a primary role in the pharmacological management of asthma, there is rarely enough time in the clinical setting to sufficiently educate patients and caregivers on the complexities of asthma management, nor address the often complex social and environmental conditions that can serve as barriers to successful asthma control.9 The most recent clinical guidelines for asthma emphasize the need to educate asthma patients at multiple points of contact throughout the community, not just the principal clinician.10
Several studies have documented the effectiveness of community-based asthma education at reducing morbidity among program participants.11–15 From a public health perspective, community-based interventions should occur on a scale large enough to have a population-level impact. The success of most community-based asthma interventions depends on both effective identification of individuals with poorly controlled asthma and provision of appropriate services. However, reaching potential beneficiaries of such programs is rarely straightforward. Even free programs often suffer poor attendance. The identification of large numbers of potential participants in a community and the subsequent communication with these individuals can be logistically and legally difficult. These barriers diminish the potential public health impact of the available services. It can be especially difficult to identify and recruit adolescents into health intervention programs for a variety of reasons, especially those with lower socioeconomic status. Parents/guardians have less influence over adolescents than younger children and health tends not to be a high priority for adolescents. Logistical challenges, such as a lack of access to transportation, further diminish participation of this age group. Moreover, few effective adolescent-focused interventions exist for asthma,11,16 and none are specific to the inner city population.
Schools may be logical locations for the implementation of public health interventions because they offer a structured environment for the identification and communication with a large proportion of a community’s children.10 Few studies have investigated the link between school-based asthma case identification and an actual asthma intervention. To determine if the large-scale case identification of adolescents with asthma and subsequent enrollment into asthma-related services was feasible in a large urban school district, a group of community stakeholders developed and demonstrated a large-scale, school-based asthma intervention program for middle school students in Oakland, CA. This report describes the development of this system and its effectiveness at identifying and enrolling students into asthma services.
Background
In 2001, the U.S. Centers for Disease Control and Prevention (CDC) provided funding to a coalition of stakeholders in Oakland, CA through its Controlling Asthma in American Cities Project (CAACP)—one of seven such centers in the United States. The goals of this project were to institutionalize asthma-related services and reduce childhood asthma morbidity through a collaborative, community-based approach in a city with at least 400,000 people. Children residing in Oakland experience the highest asthma hospitalization rates in California (California Department of Health Services EHIB, 1 July 2004, personal communication).
The coalition of Oakland stakeholders (Coalition) includes the Oakland Unified School District (OUSD), American Lung Association of California, University of California at Berkeley School of Public Health, Children’s Hospital Oakland, and other community-based organizations that have an interest in combating childhood asthma. The OUSD is a public K-12 school system with 48,000 students. It is ethnically very diverse and predominantly low income. About one-half of students’ families receive Aid for Families with Dependent Children. The student-to-nurse ratio is high, at 3,200:1 (does not include special education and screening nurses). Less than one-fifth of the middle and high schools in the OUSD has a full-time or part-time nurse.
Based on a formal community needs assessment, the Coalition determined that services were needed for children over 10 years of age since, at the time, there was already a program in Oakland for the younger children. Older children are generally less adherent with medications than are younger children and are at an important developmental age to learn disease self-management skills.17–19 The Coalition determined that the best strategy to reach a large proportion of the age group was through the public schools. A process was needed that could identify the children with asthma, prioritize those most in need of asthma-related services, and refer and enroll these students into these services in a timely manner.
To identify students with asthma in the school setting, Boss et al. recommend that school districts utilize routine administrative records, combined with other information available to the school nurse, such as written asthma management plans on file or student visitation to the nurse.20 In an ideal setting, these methods are convenient, cause minimal burden to students or school staff, and require few additional resources to implement.
However, this approach has limitations and may be especially difficult in some large or underfunded school districts, or school districts serving lower socioeconomic status populations. A high-quality asthma case identification system should capture nearly all students with asthma, contain enough information to make decisions about which students should be allocated more resources, and should be timely and accessible. In the OUSD before the start of CAACP’s efforts to address asthma in 2002, reliance on administrative records or nurse report fell far short of the standard needed for an active asthma case identification system. Although no formal assessment was attempted, there was sufficient anecdotal evidence that school nurses and school administrators were aware of only a small minority of the students who had asthma. There were many reasons why the existing mechanisms for identifying students with asthma were insufficient.
As is the case with many school districts nationally, OUSD has too few school nurses. Only 19% of OUSD schools had even a part-time nurse, and 6% had a full-time nurse. Even in schools where a nurse was available, relatively few students made an asthma-related visit to the nurse over the course of a year. Asthma management plans, which require a physician signature, were seldom completed and returned to the school. Similarly, administrative health forms in general were not completed and returned annually by parents in sufficient numbers to identify most of the students with asthma. Nurses reported especially low return rates in the secondary schools. The management of these forms was the responsibility of each school, and no standard collection or enforcement procedures were in place. The management of the forms was often left to administrative office staff or other nonhealth-related personnel. Moreover, the forms were not entered into an electronic data system, were not organized in a central location, and were often outdated or otherwise difficult to access. As the forms existed in hard copy only, acquiring lists of students with asthma at all schools was very time consuming. Moreover, it would have been necessary to create an electronic database of students’ names and contact information for purposes of creating class invitations, mailed parent letters, and summary reports.
Another problem was that the information elicited on the existing administrative health forms was not sufficient to determine whether a student had active asthma or to assess their level of asthma control. The form simply allowed for the parent to check off any of 18 health conditions that applied to the student, among which asthma was included. Many adolescents are diagnosed with asthma when much younger and may not have symptoms for many years, or have very mild or infrequent symptoms, and are unlikely to benefit significantly from an asthma intervention.21,22
Whereas administrative improvements were clearly needed at OUSD, such changes would take much time and resources. A case identification system was needed immediately that would have very high coverage and could elicit information about students’ current asthma control and could be accessed in a timely manner. Such supplemental information would allow OUSD to prioritize those students who could benefit the most from a given intervention, thereby maximizing existing resources.
Methods
In response to the program’s identified needs and the challenges with the existing administrative information, the Coalition decided to develop an age-appropriate paper-and-pencil survey tool to be self-administered by secondary school students in class. Results of the survey would then be used to identify and recruit students to asthma education classes at the school site where a health educator or school nurse could evaluate them further for possible referral to additional off-site services. A potential barrier to such a system was the need for parental consent to allow students to complete the survey. Return rates for the written consent form for another survey administered to OUSD secondary school students in 2001 ranged from 10% to 50%—levels considered unacceptable for a case identification program. OUSD school administrators determined that, because of the benign nature of the asthma survey, parental consent was not necessary for survey administration. Instead, parents/guardians could sign and return a decline-to-consent form if they did not wish to allow their children to complete the survey. The survey would not be part of the child’s school record; therefore, FERPA regulations did not apply.23 The University of California, Berkeley Committee for the Protection of Human Subjects waived the requirement for signed consent, based on the fact that there was no risk or harm to welfare as well as the fact that the project could not be carried out without such a waiver (Federal Regulation 46.116d). Nonetheless, the OUSD still required the use of a decline-to-consent form.
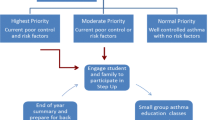
During the 2002–2003 school year, the OUSD tested a ten-question survey tool, modified from the International Survey of Asthma and Allergy in Children survey,24 at one middle and one high school. The OUSD survey included supplemental questions to determine the level of control and degree of severity. Decline-to-consent forms in multiple languages were sent home with the students 1 week before the survey date. At the designated survey time, questionnaires were distributed to all students in the class who did not return a decline-to-consent form. In addition, students had the opportunity to decline to take the survey. Surveys were administered during school hours and were proctored by schoolteachers, OUSD nurses, and staff and volunteers from the local American Lung Association (ALA). Surveys were then sent to UCB for data entry and analysis. Students eligible for asthma-related services were identified using an algorithm applied to the survey results. The questionnaire, detailed methodology, and algorithm to determine asthma categories have been published previously.25 Students who reported an asthma diagnosis and met the criteria for active asthma were eligible for basic services. Students with active asthma were further subdivided into two “risk groups.” Students with two or more of the following characteristics due to asthma-like symptoms in the previous 12 months were placed in the higher-risk group: reported visit to the ER, trouble sleeping, inability to finish saying a sentence, dry cough, or sitting out of P.E. Students in the higher-risk group were also eligible for more intensive off-site services.
The student survey was implemented on a larger scale during the 2003–2004, 2004–2005, 2005–2006, and 2006–2007 school years. The Coalition decided to focus on the middle schools exclusively and not high schools because of much higher participation among students. To avoid duplication of efforts, only incoming sixth grade students were surveyed each year. A complicating feature of most middle schools, in general, is that students change teachers each period. To address this challenge and to maximize convenience for each school, principals or designees were asked to choose their preferred strategy to survey all sixth grade students. For example, some schools administered surveys in physical education classes throughout the day, whereas others had all surveys administered in all sixth grade classes at the same time. Students who were absent on the day of the initial survey were given the survey on their return to school.
After surveys were completed for a given school, small packets were mailed by the OUSD to the parent/guardian of all children determined to have active asthma. The packet included a one-page customized letter with the survey results, as well as basic information about asthma and a list of services available by the school district and in the community. A medical evaluation was recommended if the survey indicated poorly controlled asthma. Students who reported multiple and frequent asthma-like symptoms but did not report a physician diagnosis were given a classification of possible asthma (criteria listed in Tables 1 and 2). Letters were sent to parents/guardians of these students to inform them of the results and to suggest that they speak with their physician regarding the reported symptoms. The letters also informed parents that, if their child received a physician diagnosis of asthma, they might be eligible for asthma-related services from the OUSD asthma program. The outcomes of these letters were not tracked.
Students with active asthma were eligible for school-based services that consisted of asthma education classes and limited follow-up by a school nurse. The Coalition developed a curriculum called Kickin’Asthma© for this purpose. This curriculum has been designated a “Best Practice” by the ALA, meaning it merited a sufficient score by a panel of ALA reviewers on each of the following criteria: effectiveness, cost for implementation, rigor of evaluation, accuracy, appearance, and input from the target population. The curriculum consists of four, 45-min sessions spaced 1-week apart and one review session 3 months after the fourth session. A volunteer school liaison helped schedule classes and identify children, and an OUSD school nurse or health educator from the ALA taught all the classes. The purpose of the curriculum is to teach students practical self-management skills to reduce asthma symptoms and morbidity. The sessions are designed to be fun and interactive and incorporate modalities such as role-playing, games, skits, video, and peer educators.
All eligible students were sent invitations through school to attend Kickin’Asthma©. As class attendance was voluntary, students were encouraged, but not pressured, to attend. To avoid removal of students from academic classes, the asthma classes were conducted during lunchtime and lunch was provided. Attendance was taken at the beginning of each of the four sessions. Between one and four courses of Kickin’Asthma© were conducted at each participating school throughout the year depending on the number of eligible students at each school. Class size typically ranged from 8 to 15 students. For each year of the program (except for 2005–2006), a $10 gift certificate was provided at the end of the four sessions to those students who attended at least three sessions.
The nurse or health educator sent individualized letters to all parents/guardians of children who attended Kickin’Asthma©. The letters detailed any asthma-related issues that the nurse encountered with each student, along with any recommendations. Common issues include reported symptoms two or more times per week, lost or expired medications, not keeping an extra inhaler at school, or difficulty sleeping or exercising because of asthma. As time permitted, a school nurse called parents of students especially those with frequency of symptoms or other, more complex social barriers to good asthma control.
If the nurse or health educator deemed a student in asthma classes to be high risk or the students’ survey results indicated particularly poorly managed asthma, they were referred to off-site asthma case management services or medical care, also supported by CAACP as part of the larger, community-wide effort. Referrals were at the health educator’s or school nurses’ discretion and took into consideration reported symptom frequency, overnight hospitalizations and emergency room use, medication use or lack thereof, and the capacity of the case management program, which varied throughout the year depending on staffing level and availability.
The UCB Committee for the Protection of Human Subjects, as well as the OUSD administration, approved the survey tool, survey methodology, and all program elements. Protocols were developed for sharing information between organizations, and only select program staff were given access to personal information. For purposes of statistical analysis, all data were deidentified.
Results
All 17 OUSD middle schools with greater than 500 students participated in the program. Small schools and charter schools associated with the OUSD, but with fewer than 500 students, were not included. Asthma case identification surveys and Kickin’Asthma© classes were administered at all participating schools. Of the estimated 9,335 decline-to-consent forms that were disseminated, 275 (2.9%) were signed and returned. A total of 8,326 surveys were returned between October 2003 and January 2007, representing 91.9% of sixth grade students at eligible middle schools during the 4 years of program implementation.
Of the 8,326 students who returned a survey, 1,546 (18.6%) reported being told they have asthma by a doctor or parent, and 422 (5.1%) were determined to have possible asthma (i.e., substantial asthma-like symptoms but no reported diagnosis; Tables 1 and 2). Among the students told previously that they had asthma, 94.3% (n = 1,458) were classified as having active asthma (diagnosis plus one or more asthma-like symptoms or episodes). About one-quarter of these students reported an emergency room visit for asthma during the preceding 12 months, and approximately one-half reported activity limitations and sleep disturbances because of asthma (Tables 1 and 2).
All students with active asthma were invited to attend school-based asthma education classes. Of the 1,449 children eligible for asthma education who were still enrolled in school at the time of the classes, 1,217 (83%) attended at least one Kickin’Asthma© session (Table 3). During the 3 years that attendance was tracked for each session, 732 out of the 1,207 eligible students (60.6%) attended at least three out of the four class sessions. Attendance varied from year to year. During the 2005–2006 school year, incentives were dropped because of budget constraints. Retention was lower during 2005–2006 than the other years, although it is not possible to ascribe definitively that the drop in retention was because of the lack of incentives. Of 681 students who were eligible and referred for off-site case management services, 232 (34%) participated.
Discussion
A large, urban school district in Oakland, CA, and its community partners, was able to demonstrate a large-scale system to effectively identify and recruit adolescent students with asthma into appropriate services. The proportion of all middle school students in the targeted schools who took the case identification survey was notably high (92%), as was the proportion of eligible students who participated in the school-based services (83%).
Detailed health outcomes of the Kickin’Asthma© education program are presented in a separate paper.26 It is worth noting that students who participated experienced significantly fewer symptoms, days with activity limitation, nights of sleep disturbance, and emergency department visits. These results are stronger than those previously published for adolescents participating in school-based asthma programs.19,27 Truly effective public health programs must not only improve outcomes among participants, they must also be able to efficiently identify and engage large numbers of the targeted population.
Schools are logical places to conduct large-scale public health activities because they offer a structured environment for locating and working with a large proportion of a community’s children. Schools often have resources (e.g., meeting space, parental contact information, and nursing staff) not necessarily available elsewhere, and previous studies have found that school-based health education garners higher attendance rates compared to clinic-based programs, particularly in urban settings.28,29 Many school districts have additional interest in addressing asthma, as poorly controlled asthma can impact school attendance, academic performance, and general well being of students.28
Several studies have reported the results of school-based programs aimed at finding students with asthma (case identification) and/or students with asthma symptoms but no asthma diagnosis.4,30–36 However, few studies have investigated the link between school-based case identification and an actual asthma intervention.37 Likewise, few studies have focused on the identification of students with asthma in the secondary schools, an age group with whom many perceive to be more difficult to work compared to elementary school-aged children.17,38
Factors that likely contributed to the success in Oakland include the allowance of flexibility for the schools in the survey completion process, minimization of the burden on teachers, and identification of volunteer school liaisons to help with all facets of the process. Scheduling of classes during nonacademic times facilitated support from school staff. Persistent marketing and recruitment contributed to our success at getting over 83% of eligible students to come to the classes. An engaging curriculum and enjoyable environment likely played a role in retaining students for multiple sessions—nearly 75% of students who enrolled in classes attended at least three out of the four sessions. Self-administration of the surveys by students during school contributed to the high completion rate of the surveys. Furthermore, OUSD administrators allowed a “partial waiver” of parental consent, such that signature was required only if the parent did NOT want the student to participate. If parental consent to take the survey had been required by the UCB Review Board or OUSD, it would have made the estimates of asthma occurrence too imprecise to be useful and would have missed many children who would have participated in the classes. Lastly, the collaborative nature of this community-based undertaking brought in the necessary skills, manpower, expertise, and volunteers to make it possible.
One limitation to the system is that some children at participating schools were not captured by the surveys, including those students who were absent on the survey date and whose teachers did not provide the make-up, and students who transferred into school after the survey date. Those children in the community who are home-schooled, attend private or charter schools, or were not in school at all are not captured.
Some misclassification is to be expected, as is the case with most surveys that rely on self-report. The question as to whether the respondent had ever been diagnosed by a physician with asthma is nearly identical to that used in several other school-based surveys, including the validated asthma prevalence survey developed for the International Study of Asthma and Allergies in Childhood, which is administered to 13- to 14-year-old children.24 The OUSD asthma surveys as well as similar ones done in other settings demonstrate good or very good concordance between adolescent and parental reporting of asthma diagnosis.25,39,40 Children tended to report more symptoms than the parents. Reliability studies have shown mixed results for asthma surveys among children younger than middle school age.41–43 One other limitation of an annual asthma survey, as with any variable disease or condition, is that measures of asthma control vary according to time, particularly with regard to season. The main criteria for initially identifying students with asthma—ever receiving an asthma diagnosis and the experience of symptoms during the previous 12 months—are minimally subject to this natural variation. The variability is most likely to influence which students are designated as higher risk and referred for the more intensive services, although additionally the nurse or health educator had the opportunity to further assess students over a period of 4 weeks.
While CDC recommends school-based case identification approaches to find students with diagnosed and active asthma, the benefits of population-based case detection—finding undiagnosed cases of asthma—are unproven.20,31,44 Although previous studies have shown that asthma case detection surveys have high reproducibility, the American Thoracic Society Working Group on Asthma Screening (ATS-WGAS) determined that case detection in schools and other community settings is currently not recommended, citing the inevitable impact of false positives, the lack of evidence of cost-effectiveness, uncertain benefit, and inconsistent access to follow-up clinical care, among other concerns.45 However, surveys administered for asthma case identification purposes, such as those administered at the OUSD, inevitably produce information that can be used to identify individuals with undiagnosed asthma. The ATS-WGAS did not provide recommendations for this particular circumstance. The OUSD and its partners believed it was ethically obligated to inform the parent/guardian of those students who did not report a diagnosis but whose survey responses suggested a particularly high likelihood of having asthma (i.e., “possible asthma”) based on a conservative physician-designed algorithm.
It should also be noted that three OUSD high schools participated during the first 2 years of the program. The survey methodology and curriculum were the same as for the middle schools. Whereas survey response was similar to that of the middle schools, attendance to the onsite asthma education program was substantially lower. It was very difficult to schedule asthma classes in these high schools at a time other than lunch because of increased pressure to have students attend academic classes. We attribute the lower attendance to the observation that many high school students leave campus during lunchtime to eat and socialize and are unwilling to voluntarily attend asthma classes during this time. Although we were able to obtain high attendance during physical education at one high school, we decided to focus on middle schools exclusively.
Several criteria should be considered when deciding whether to implement a survey-based asthma case identification system in a school system.46 The added time and cost of such a system may be most appropriate in school settings with high asthma prevalence and poorly organized, incomplete, or otherwise inaccessible school health records. We suspect that these criteria are true of many school districts around the U.S. It is also crucial that school-based asthma services and/or off-site linkages with asthma case managers or medical providers exist for those students identified as having poorly controlled asthma. Lastly, to effectively optimize local resources, schools and school districts should consider opportunities for partnerships in their communities.47
As a result of the success of this program, and with help from the Coalition, the OUSD has taken steps toward institutionalization of the asthma case identification process. The OUSD School Board passed an asthma policy that requires that the District to maintain an unspecified system for identifying students with current asthma and to designate a nurse to be responsible for asthma-related activities.
As a first step toward improving the existing system, the OUSD Forms Committee added additional asthma questions to the emergency contact forms that are required to be completed by parents during school registration. These new forms allow school personnel to determine whether any student has asthma, whether it is active, and what asthma medications she/he currently uses. Additional questions could not be included because of space considerations and competing priorities. Concurrently, the OUSD has been able to increase parental completion of the emergency contact forms, asthma management plans, and other health forms by improving the appearance and readability of the forms, emphasizing to parents the importance of completing the forms during the registration process, and instructing school nurses and front-office staff to aggressively follow-up with parents who do not complete them. The emergency forms are now being used for asthma case identification at all elementary schools in the OUSD—over 85% of the enrolled students in a random sample of seven schools had an emergency contact form on file at the end of the 2006–2007 school year. Although many of the marginal benefits of the surveys remain, these steps have increased the viability of a sustainable asthma case identification system that the OUSD is able to implement without additional resources or outside support. These efforts have also improved school–parent communication in general and student health surveillance for other conditions besides asthma.
One remaining drawback of the administrative-based case identification system, compared to a survey-based system, is that it does not get the same amount of information about each child’s asthma. Unless additional questions can be added in the future, identifying children with the most poorly controlled asthma will be quite difficult. It is very important for schools to be able to prioritize higher-risk children, particularly in schools with limited resources and high asthma prevalence. Less detailed information also means a greater probability of misclassification. Another drawback is that the information exists in hard copy only and is not centralized in one location. Neither a computerized system, nor the staff to enter the data currently exists, making the information greatly more time consuming to access and to produce reports, such as lists of students or asthma prevalence. Furthermore, it remains to be seen if a nonsurvey-based system will be sufficient for large-scale case identification in the secondary schools where timely completion of the health forms can still be low at many schools. The OUSD continues to make improvements to its administrative infrastructure and will monitor the benefits of both survey-based and administrative-based asthma case identification systems to balance the need for sustainability with the need for high coverage, detailed information, and accessibility.
Conclusion
A coalition of community organizations demonstrated a population-level system to identify, stratify, and provide interventions for adolescents with asthma in a large urban school district. A brief paper-and-pencil survey captured 92% of students in the targeted schools, and 83% of those identified in need of services received support at school, many of whom were also referred to services off-site. School districts with incomplete or inadequate health records, high asthma prevalence, and internal or external services available for students with asthma may benefit from a similar system. A large-scale model, such as the one described, is generalizable and replicable; provides a model for successful collaboration between a school district, academic institution, and community organizations; and may be an effective public health strategy for other conditions as well as asthma.
Abbreviations
- CDC:
-
Centers for Disease Control and Prevention
- OUSD:
-
Oakland Unified School District
- CAACP:
-
Controlling Asthma in American Cities Project
- UCB:
-
University of California at Berkeley, School of Public Health
References
Mannino DM, Homa DM, Akinbami LJ, Moorman JE, Gwynn C, Redd SC. Surveillance for asthma—United States, 1980–1999. MMWR Surveill Summ. 2002;51(1):1–13.
Health Data for All Ages. CDC, National Center for Health Statistics. Available at: http://www.cdc.gov/nchs/health_data_for_all_ages.htm. Accessed 13 September 2007.
Wang LY, Zhong Y, Wheeler L. Direct and indirect costs of asthma in school-age children. Prev Chronic Dis. 2005;2(1):A11.
Clark NM, Brown R, Joseph CLM, et al. Issues in identifying asthma and estimating prevalence in an urban school population. J Clin Epidemiol. 2002;55(9):870–881.
Lieu TA, Lozano P, Finkelstein JA, et al. Racial/ethnic variation in asthma status and management practices among children in managed medicaid. Pediatrics. 2002;109(5):857–865.
Bai Y, Hillemeier MM, Lengerich EJ. Racial/ethnic disparities in symptom severity among children hospitalized with asthma. J Health Care Poor Underserved. 2007;18(1):54–61 Feb.
Smith LA, Hatcher-Ross JL, Wertheimer R, Kahn RS. Rethinking race/ethnicity, income, and childhood asthma: racial/ethnic disparities concentrated among the very poor. Public Health Rep. 2005;120(2):109–116.
Kattan M, Mitchell H, Eggleston P, et al. Characteristics of inner-city children with asthma: the National Cooperative Inner-City Asthma Study. Pediatr Pulmonol. 1997;24(4):253–262.
Elward KS. Asthma days: an approach to planned asthma care. Fam Pract Manag. 2004;11:43–48. Available at: http://www.aafp.org/fpm/20041000/43asth.html. Accessed 25 September 2007.
National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health Expert Panel Report 3 (EPR 3): Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health; 2007.
Agency for Healthcare Research and Quality. Closing the Quality Gap: A Critical analysis of Quality Improvement Strategies. 04(07)-0051-5 ed. Agency for Healthcare Research; 2007.
Burkhart PV, Rayens MK, Oakley MG, Abshire DA, Zhang M. Testing an intervention to promote children’s adherence to asthma self-management. J Nurs Scholarsh. 2007;39(2):133–140.
Joseph CL, Peterson E, Havstad S, et al. A web-based, tailored asthma management program for urban African-American high school students. Am J Respir Crit Care Med. 2007;175(9):888–895.
Kaplan DL, Rips JL, Clark NM, Evans D, Wasilewski Y, Feldman CH. Transferring a clinic-based health education program for children with asthma to a school setting. J Sch Health. 1986;56(7):267–271.
Evans D, Clark NM, Feldman CH, et al. A school health education program for children with asthma aged 8–11 years. Health Educ Q. 1987;14(3):267–279.
Wolf FM, Guevara JP, Grum CM, Clark NM, Cates CJ. The Cochrane Database of Systematic Reviews. Issue 4. 2002. Wiley. Educational interventions for asthma in children.
Ayala GX, Miller D, Zagami E, Riddle C, Willis S, King D. Asthma in middle schools: what students have to say about their asthma. J Sch Health. 2006;76(6):208–214.
de Benedictis D, Bush A. The challenge of asthma in adolescence. Pediatr Pulmonol. 2007;42(8):683–692.
Bruzzese JM, Bonner S, Vincent EJ, et al. Asthma education: the adolescent experience. Patient Educ Couns. 2004;55(3):396–406.
Boss LP, Wheeler LS, Williams PV, Bartholomew LK, Taggart VS, Redd SC. Population-based screening or case detection for asthma: are we ready? J Asthma. 2003;40(4):335–342.
Sears MR, Greene JM, Willan AR, et al. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349(15):1414–1422.
Strachan D, Gerritsen J. Long-term outcome of early childhood wheezing: population data. Eur Respir J Suppl. 1996;21:42s–47s.
Family Educational Rights and Privacy Act. U S Department of Education. Available at: http://www.ed.gov/policy/gen/guid/fpco/ferpa/index.html. Accessed 14 July 2007.
Asher MI, Keil U, Anderson HR, et al. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Respir J. 1995;8(3):483–491.
Magzamen S, Mortimer KM, Davis A, Tager IB. School-based asthma surveillance: A comparison of student and parental report. Pediatr Allergy Immunol. 2005;16(8):669–678.
Magzamen S, Patel B, Davis A, Tager IB. “Kickin’ Asthma”: school-based asthma education in an urban community. J Sch Health. 2008; in press.
Berg J, Tichacek MJ, Theodorakis R. Evaluation of an educational program for adolescents with asthma. J Sch Nurs. 2004;20(1):29–35.
Christiansen SC, Zuraw BL. Serving the underserved: school-based asthma intervention programs. J Asthma. 2002;39(6):463–472.
Guevara JP, Wolf FM, Grum CM, Clark NM. Effects of educational interventions for self management of asthma in children and adolescents: systematic review and meta-analysis. BMJ. 2003;326(7402):1308–1309.
Yawn BP, Wollan P, Scanlon P, Kurland M. Are we ready for universal school-based asthma screening? An outcomes evaluation. Arch Pediatr Adolesc Med. 2002;156(12):1256–1262.
Yawn BP. Asthma screening, case identification and treatment in school-based programs. Curr Opin Pulm Med. 2006;12(1):23–27.
Bauer EJ, Lurie N, Yeh C, Grant EN. Screening for asthma in an inner-city elementary school in Minneapolis, Minnesota. J Sch Health. 1999;69(1):12–16.
Jones CA, Morphew T, Clement LT, et al. A school-based case identification process for identifying inner city children with asthma: the Breathmobile program. Chest. 2004;125(3):924–934.
Miles R. Four pilot projects completed for school-based allergy and asthma screening. Ann Allergy Asthma Immunol. 2003;90(5):461–463.
Wheeler LS, Boyle S. Attempting to use a district-wide asthma case identification system for asthma prevalence. J Sch Health. 2006;76(6):219–222.
Vargas PA, Magee JS, Bushmiaer M, et al. School-based asthma case finding: the Arkansas experience. J Sch Health. 2006;76(6):223–226.
Yawn BP, Wollan P, Scanlon PD, Kurland M. Outcome results of a school-based screening program for undertreated asthma. Ann Allergy Asthma Immunol. 2003;90(5):508–515.
Joseph CL, Baptist AP, Stringer S, et al. Identifying students with self-report of asthma and respiratory symptoms in an urban, high school setting. J Urban Health. 2007;84(1):60–69.
Wittich AR, Li Y, Gerald LB. Comparison of parent and student responses to asthma surveys: students grades 1–4 and their parents from an urban public school setting. J Sch Health. 2006;76(6):236–240.
Yawn BP, Wollan P, Kurland M, Bertram S. Comparison of parent and student responses to asthma surveys: students grades 3–12 and their parents from a suburban private school setting. J Sch Health. 2006;76(6):241–245.
Gerald LB, Grad R, Turner-Henson A, et al. Validation of a multistage asthma case-detection procedure for elementary school children. Pediatrics. 2004;114(4):E459–E468.
Redline S, Larkin EK, Kercsmar C, Berger M, Siminoff LA. Development and validation of school-based asthma and allergy screening instruments for parents and students. Ann Allergy Asthma Immunol. 2003;90(5):516–528.
Galant SP, Crawford LJ, Morphew T, Jones CA, Bassin S. Predictive value of a cross-cultural asthma case-detection tool in an elementary school population. Pediatrics. 2004;114(3):e307–e316.
CDC. Strategies for addressing asthma within a coordinated school health program, with updated resources. Atlanta, Georgia: CDC, National Center for Chronic Disease Prevention and Health Promotion, 2005. Available at: http://www.cdc.gov/HealthyYouth/asthma/pdf/strategies.pdf. Accessed 14 July 2007.
Gerald LB, Sockrider MM, Grad R, et al. An official ATS workshop report: issues in screening for asthma in children. Proc Am Thorac Soc. 2007;4(2):133–141.
Wheeler LS, Boss LP, Williams PV. School-based approaches to identifying students with asthma. J Sch Health. 2004;74(9):378–380.
Communities in Action for Asthma Friendly Environments Network. Available at: http://www.asthmacommunitynetwork.org/default.aspx. Accessed 25 September 2007.
Acknowledgement
This research is supported with a grant from the Centers for Disease Control and Prevention, Grant No. U59/CCU92324-02.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplemental Material
The following supplemental material is available for this article online: Appendix 1. Student Health Survey (DOC 38.5 KB)
Rights and permissions
About this article
Cite this article
Davis, A., Savage Brown, A., Edelstein, J. et al. Identification and Education of Adolescents with Asthma in an Urban School District: Results from a Large-scale Asthma Intervention. J Urban Health 85, 361–374 (2008). https://doi.org/10.1007/s11524-008-9266-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-008-9266-y