
Abstract
We present a new method measuring body impedance using a thigh-to-thigh current path, which can reflect the abdominal fat portion more sensitively and can be conveniently applied during the daily use on a toilet seat. Two pairs of electrodes were installed on a toilet seat to provide current and to permit voltage measurement through a thigh-to-thigh current path. The effectiveness of the method was compared with conventional foot-to-foot and hand-to-foot current paths by simulation and by experiments referenced to computed tomography (CT) image analysis. Body impedance using three different current paths was measured, and abdominal CT images were acquired for eight subjects. Measured body impedances were compared with the visceral to subcutaneous fat ratio (VF/SF) calculated from the CT-determined abdominal fat volume. The thigh-to-thigh current path was about 75% more sensitive in abdominal fat measurement than the conventional current paths in simulation experiments and displayed a higher VF/SF correlation (r = 0.768) than the foot-to-foot (r = 0.425) and hand-to-foot (r = 0.497) current paths.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The prevalence of obesity is increasing worldwide. As the risks of some adult diseases are positively correlated with body fat, body fat monitoring is considered as an appropriate method to maintain good health level [1–6]. Obesity-related adult diseases, so-called adult diseases, include type 2 diabetes: coronary heart disease (CHD) and severe sleep apnea. CHD is a major risk factor for cardiovascular disease (CVD).
Abdominal body fat is strongly correlated to adult diseases compared to limb body fat. People with an abnormally high level of abdominal body fat (especially visceral adipose tissue) have a higher risk of adult disease than other traditionally obese people, even though they appear similar to non-obese people and their waist and hip girths and weight are in the normal (non-obese) range [7].
There are several methods currently available to estimate human body composition including body fat [8–10]. Imaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI) can accurately determine the amount of body fat from the human abdomen. Even though they are regarded as the standard of human abdominal body fat measurements, the expense and radiation exposure of these methods strictly limit their practical use.
Bioelectrical impedance analysis (BIA) is a widely used approach that measures electrical impedance at specific frequencies and estimates a person’s body fat proportion. BIA has advantages of being portable, safe, easy and quick to perform, noninvasive and reproducible, in addition to its low evaluation cost. BIA methods commonly use hand-to-foot (wrist-to-ankle), foot-to-foot (ankle-to-ankle), or hand-to-hand (wrist-to-wrist) paths, or combinations of these paths for the electrical current flow [11]. In these paths, the impedance of limbs contributes more to total measured impedance than torso impedance does, because the cross-sectional area of limbs is much smaller than those of the trunk [12, 13]. While measured data mainly reflect the impedance changes of limbs, the change of the trunk represents an appreciably smaller contribution. Impedance across the abdomen constitutes only 5–10% of the total impedance of the foot-to-foot and hand-to-foot paths [14]. Therefore, it is hard to estimate visceral fat sensitively and distinguish viscerally obese people from non-obese people using these current paths.
In order to monitor the variation of visceral fat, a more sensitive method that is also convenient for daily use is needed. Here, we present a new method of measuring body impedance using a thigh-to-thigh current path that can reflect abdominal fat portion more sensitively. For body fat proportion estimation, this method is localized to the abdominal area and can be applied during daily home life as a health-monitoring option.
2 Subjects and methods
2.1 Thigh-to-thigh current path for impedance measurements
The thigh-to-thigh current path was introduced to increase the sensitivity of body impedance measurements for abdominal fat. Figure 1 depicts the thigh-to-thigh current path that was applied during use of a toilet seat for practical measurement, along with the conventional foot-to-foot (ankle-to-ankle) and hand-to-foot (wrist-to-ankle) current paths. During the experiment, body impedances of the subjects were measured with these current paths. A 100-μA current was applied with a frequency of 50 kHz, because this frequency is most frequently used at the single-frequency BIA [9, 15]. Also, the frequencies of applied current were varied from 1.0 kHz to 1.0 MHz to evaluate the dependency of impedance on current frequency. Thirty frequencies were chosen logarithmically per decade, so that the whole frequency samples consisted of 91 points. The impedance was calculated by dividing measured voltage by applied current [16].

Current paths to measure impedances. a Thigh-to-thigh current path, which was applied on toilet seat for measurement. b Foot-to-foot current path c Hand-to-foot current path
A SI 1260 impedance analyzer (Solartron Analytical) was used for impedance measurements with a 1294 impedance interface (Solartron Analytical) for safety. For thigh-to-thigh current path measurements, electrodes were made of commercial copper tape and were attached to the toilet seat. These metal electrodes were directly connected to the 1294 impedance interfaces. Each subject was seated on a toilet seat, and the tetra-polar bioelectrical impedance measurement method was used [17]. The electrode pair closer to the knees drove electrical current and the other pair sensed voltage difference under the driven current (Fig. 1a).
For measurements using the foot-to-foot and hand-to-foot current paths, clip-type metal electrodes were used for tetra-polar measurements with the electrodes being placed on each subject’s ankle or wrist (Fig. 1b and c). The current driven electrodes were on the outside of both ankles for the foot-to-foot path and the right wrist and right ankle for the hand-to-foot path, with the voltage sensing electrodes on the inside of the same positions of the limbs. Subjects maintained a stable lying position on a couch during the measurement with these two current paths.
Every measurement was performed after a 10-min rest in the measuring posture for the stabilization of water distribution in the body. For each measurement, at least 200 ms of stable segment were used for impedance calculation. The average of two measurements was used for the calculation of impedance for each path. The contacts between skin and electrodes were fully saturated with water to minimize the effects of skin-electrode contact impedances.
2.2 Simulation analysis
Simulation analysis was performed to ascertain the sensitivity of the impedance according to the current paths. The finite element model (Fig. 2) was used to represent the right half of trunk, right leg, and right arm. The left half of trunk, left leg, and right arm were omitted by an equivalent model using the symmetric property. The size of the trunk was 20 cm (anterior–posterior) × 20 cm (proximal–distal) × 70 cm (superior–inferior), and the trunk was divided into three areas: chest, abdomen, and pelvis. The leg was made of an ellipsoid and truncated cone, 15 cm in diameter at the maximum point and 70 cm in length. The arm was cylinder-shaped, 6 cm in diameter, and 50 cm in length. By checking the relationship between the conductivity of fat-mixture of the trunk and calculated impedance, the sensitivity of the body impedance measuring method was evaluated according to the variation of the fat. In the simulation, we allocated the fat in abdominal blocks as shown in Fig. 2 with different portions of fat composition.

Modeling to evaluate the sensitivity of the method on fat concentrated location. a Thigh-to-thigh path. b Foot-to-foot and hand-to-foot paths
Body tissues could be divided into three tissue groups: negligibly conductive (bone), partially conductive (fat), and fully conductive (such as flesh and muscle) [16]. Impedances were calculated based upon the geometry of volume and the equivalent conductivity. Equivalent conductivity was calculated from the conductivities of different types of tissues (Table 1) and their constitutional proportions (r fat) by Eq. 1.
Impedances were calculated in the simulation by varying the fat proportions from 0 to 40% in 5% stepwise increments. The computer simulations were performed with finite element modeling and simulation software “COMSOL Multiphysics” Ver. 3.4 (COMSOLAB).
2.3 Subjects
For the evaluation experiments, impedance was measured from eight healthy male volunteers whose average age, height, and weight were 27.6 years, 173.4 cm, and 69.4 kg, respectively. Their waist and hip girths were also measured, and these data were used for the calculation of body mass index (BMI) which was calculated by dividing body weight by height squared [18, 19]. The average of waist and hip girths were 79.3 and 94.2 cm, respectively, and average BMI was 23.0 kg/m2 (Table 2). Each subject was initially examined by a CT scan, and impedance was measured with the three different current paths on the same day.
2.4 CT image analysis
CT scans were done using a Siemens Somatom Sensation 16. CT images of 20–23 slices from the L2–L5 level with a 5-mm slice thickness were stored in the DICOM file format with a 512 × 512 pixel size. For image segmenting and analysis, public domain Java image-processing software (ImageJ Ver. 1.37) was used. Since visceral obesity highly correlates with adult diseases like hypertension or diabetes [20–22], the CT parameter of visceral fat (VF) to subcutaneous fat (SF) ratio (VF/SF) is widely used for the evaluation of visceral obesity [23]. In order to calculate the amount of VF and SF separately, the fat area was first extracted from the abdomen area (L2–L5) based on CT numbers. Pixels having Hounsfield units from −250 to −50 were considered as the fat region. The fat region was divided into VF and SF (Fig. 3). The number of pixels from visceral adipose tissue (VF) and subcutaneous adipose tissue (SF) was calculated from each CT image slice, and the number of pixels was summed up through all the CT slices from L2–L5.

Segmented fat area from a representative CT image. a Raw image of CT data. b Segmentation of whole fat area from a. c Segmentation of visceral fat area from b. d Segmentation of subcutaneous fat area from b
2.5 Data analysis
In order to estimate the sensitivity of the suggested thigh-to-thigh current path by simulation, sensitivity index α was calculated as in Eq. 2 for each measurement and compared.
In this equation, Zfat free is the body impedance data when the fat proportion is 0% in the tissue and Zwith fat is the impedance data from fat mixed tissue with allocated proportion at the abdomen area of the model in Fig. 2. The sensitivity index α was evaluated for each of current path by varying fat proportions. For the experimental data, correlations between impedance of each current path and VF/SF of CT volume data were calculated and compared. In order to ascertain the dependency of impedance on current frequency, these correlations were calculated by varying the frequencies of applied current from 1.0 kHz to 1.0 MHz.
3 Results
Table 3 shows the results for the sensitivity simulation of thigh-to-thigh path in comparison with foot-to-foot and hand-to-foot current paths with the model in Fig. 2. We confirmed that the sensitivity index α was higher with the thigh-to-thigh path than with the other paths. With increased fat proportion, the sensitivity of the thigh-to-thigh path increased, reaching a maximum of 3.62% at a fat proportion of 40%. This value was 82% higher than the sensitivity of the foot-to-foot path and 66% higher than the sensitivity of the hand-to-foot path.
Table 4 shows the impedance data of each subject at 50 kHz frequency. These data are the averaged values of two measurements for each current path. The impedance with thigh-to-thigh current path displayed much smaller impedances than those with the other two current paths. Impedance was only about 8.7% of the data with the foot-to-foot path (28.85–331.64 Ω) and about 7.5% of the data with the hand-to-foot path (28.85–384.58 Ω). These differences likely resulted from the bypass of the high impedance regions of the limbs [12, 14]. The average impedances of the eight subjects with current frequencies from 1.0 kHz to 1.0 MHz for three current paths are shown in Fig. 4. Impedances with the foot-to-foot and hand-to-foot current paths were about 10 times bigger than the impedance with the thigh-to-thigh path throughout the whole frequency range. Even though the impedances decreased slowly with increasing frequency, it was difficult to find any frequency-dependent characteristics.

Dependence of measured impedance on current frequency for three current paths. Frequencies varied from 1.0 kHz to 1.0 MHz
Calculated fat volumes (VF, SF) and their ratio (VF/SF) from the CT image data are shown in Table 5. The average VF/SF was 79.86%. The smallest and largest values of VF/SF were 56.77 and 98.05%, respectively.
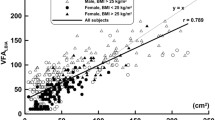
Correlations between impedance of each current path at 50-kHz frequency and VF/SF from CT volume are shown in Fig. 5. The impedance with the thigh-to-thigh path at 50-kHz frequency had a stronger correlation (r = 0.768) than the foot-to-foot and hand-to-foot current paths, whose correlations were 0.425 and 0.497, respectively. Correlations between the impedance of each current path and VF/SF of CT volume data depending on current frequencies are shown in Fig. 6 at frequencies from 1.0 kHz to 1.0 MHz. The thigh-to-thigh path displayed a higher correlation with abdominal CT volume data than the foot-to-foot and hand-to-foot paths throughout the frequency range.

Correlations between the impedances measured by three different current paths at 50-kHz frequency and VF/SF from CT volume data

Correlations between the impedances measured by three different current paths for frequencies from 1.0 kHz to 1.0 MHz and VF/SF from CT volume data
4 Discussion
Concerning correlation to CT data, positions while measuring impedance are relatively unimportant [24]. Therefore, we presently chose different positions with every current path in consideration of actual measurement conditions.
Presently, impedances with the foot-to-foot and hand-to-foot current paths were about 10 times bigger than the impedance measured with the thigh-to-thigh path. These results were likely attributable to the higher impedances of limbs. In these current paths, current flows through the arm and foot, which have relatively higher impedance due to their geometry, while the thigh-to-thigh path bypasses limb-related high impedance. This reduced impedance caused by bypassing of the limb impedances is the main reason for the increased sensitivity of measured impedance to the fat proportion in the abdominal torso region. A slow decrease in measured impedance with increasing frequency was evident. This could be partly due to the capacitive nature of human tissue; impedance values with relatively lower frequencies are larger than those with relatively higher frequencies [25].
As shown in Fig. 6, correlations of impedance with the thigh-to-thigh path to the CT volume data were much higher than those with the other paths throughout the frequency range from 1.0 kHz to 1.0 MHz of applied current. The correlation of impedance with the foot-to-foot path to the CT data showed a similar aspect with the hand-to-foot path, as compared with the thigh-to-thigh path. Despite the marginally decreased correlation between impedance with a foot-to-foot path and CT data at higher frequencies, correlations between impedance with the foot-to-foot and hand-to-foot paths and the CT data maintained lower levels. Therefore, we conclude that there is little frequency specific characteristics with the three methods, and a single nominal frequency of 50 kHz is sufficient to evaluate abdominal fat by the thigh-to-thigh path.
The measured impedance with the thigh-to-thigh current path was more strongly correlated to the abdominal fat ratio, because measured impedances with the conventionally used foot-to-foot and hand-to-foot paths had much lower correlations to the abdominal VF/SF fat ratio. This means that impedance measurements with the thigh-to-thigh current path is a good way to evaluate body fat in the abdominal area, especially with respect to VF/SF. Moreover, this method can be used more effectively to monitor the possibility of visceral obesity, which can be related to adult diseases including CVD [26].
The thigh-to-thigh current path is easily accommodated using a toilet seat format. By installing metal electrodes on the top surface of a toilet seat, data can be collected during a subject’s daily activities in a bathroom without additional measurement efforts. Humans use a toilet seat more than once a day, with bare skin contacting the toilet seat during the time of use. This provides a perfect opportunity for the direct skin contact of the metal electrodes that is necessary for the measurements. Moreover, the measurements can be obtained unobtrusively during a natural daily activity. Use of other objects such as a seat or a bed is more onerous since direct contact of electrodes with skin is much less apt to occur. Therefore, this method can be used to manage body fat intelligently and diminish the occurrence and progress of obesity-related adult diseases in the realm of ubiquitous healthcare.
5 Conclusion
We suggest a new method to measure body impedance with a higher correlation to abdominal VF/SF. The suggested thigh-to-thigh current path shows higher sensitivity to abdominal fat proportion and reflects visceral obesity more effectively than the conventionally used current paths for body impedance measurement. Also, the thigh-to-thigh path is suitable for ubiquitous healthcare monitoring and can be measured easily on a toilet seat without constraints and even the awareness of subjects.
References
Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash R, Hollenbeck A, Leitzmann MF (2006) Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old N. Engl J Med 355(8):763–778
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults N. Engl J Med 348(17):1625–1638
Flegal KM, Graubard BI, Williamson DF, Gail MH (2005) Excess deaths associated with underweight, overweight, and obesity. JAMA 293(15):1861–1867
Jeffreys M, McCarron P, Gunnell D, McEwen J, Smith GD (2003) Body mass index in early and mid-adulthood, and subsequent mortality: a historical cohort study. Int J Obesity 27:1391–1397
Maffeis C, Tatò L (2001) Long-term effects of childhood obesity on morbidity and mortality. Horm Res 55(suppl 1):42–45
Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, Eckel RH (2006) Obesity and cardiovascular disease: pathophysiology, evaluation and effect of weight loss. Circulation 113:898–918
Florence C, David BA, Re′mi R, Maxime O, David HP, Andre′anne T, Eric TP (2004) Metabolic and behavioral characteristics of metabolically obese but normal-weight women. J Clin Endocrinol Metab 89:5013–5020
Baumgartner RN, Chumlea WC, Roche AF (1989) Estimation of body composition from bioelectric impedance of body segments. Am J Clin Nutr 50:221–226
Kyle UG et al (2004) Bioelectrical impedance analysis-part I: review of principles and methods. Clin Nutr 23:1226–1243
Kyle UG et al (2004) Bioelectrical impedance analysis-part II: utilization in clinical practice. Clin Nutr 23:1430–1453
Tyrrell VJ, Richards G, Hofman P, Gillies GF, Robinson E, Cutfield WS (2001) Foot-to-foot bioelectrical impedance analysis: a valuable tool for the measurement of body composition in children. Int J Obesity 25:273–378
Turner AA, Lozano-Nieto A, Bouffard M (2002) Comparison of segmental and global bioimpedance spectroscopy errors using generalizability theory Physiol. Meas 23:43–57
Scharfetter H, Brunner P, Mayer M, Brandstätter B, Hinghofer-Szalkay H (2005) Fat and hydration monitoring by abdominal bioimpedance analysis: data interpretation by hierarchial electrical modeling. IEEE Trans Biomed Eng 52(6):975–982
Organ LW, Bradham GB, Gore DW, Lozier SL (1994) Segmental bioelectrical impedance analysis: theory and application of a new technique. J Appl Physiol 77:98–112
Mellar PD, Tugba Y, Dilara K, Jordanka K, Declan W, Lasheen W, Ruth L, Matthew TK (2009) Bioelectrical impedance phase angle changes during hydration and prognosis in advanced cancer. Am J Hospice Pall Med, CARE Online First, doi:10.1177/1049909108330028
Faes TJC, van der Meij HA, de Munck JC, Heethaar RM (1999) Topical review—The electric resistivity of human tissues (100 Hz–10 MHz): a meta-analysis of review studies. Physiol Meas 20:R1–R10
Lukaski HC, Bolonchuk WW, Hall CB, Siders WA (1986) Validation of tetrapolar bioelectrical impedance method to assess human body composition. J Appl Physiol 60(4):1327–1332
Frankenfield DC, Rowe WA, Cooney RN, Smith JS, Becker D (2001) Limits of body mass index to detect obesity and predict body composition. Nutrition 17:26–30
Pecoraro P, Guida B, Caroli M, Trio R, Falconi C, Principato S, Pietrobelli A (2003) Body mass index and skinfold thickness versus bioimpedance analysis: fat mass prediction in children. Acta Diabetol 40:S278–S281
Björntorp P (1992) Abdominal fat distribution and disease: an overview of epidemiological data. Ann Med 24(1):15–18
Michael IG, Barbara AG (1999) Relation between visceral fat and disease risk in children and adolescents. Am J Clin Nutr 70:S149–S156
Eguchi Y, Eguchi T, Mizuta T, Ide Y, Yasutake T, Iwakiri R, Hisatomi A, Ozaki I, Yamamoto K, Kitajima Y, Kawaguchi Y, Kuroki S, Ono N (2006) Visceral fat accumulation and insulin resistance are important factors in nonalcoholic fatty liver disease. J Gastroenterol 41:462–469
Tokunaga K, Matsuzawa Y, Ishikawa K, Tarui S (1983) A novel technique for the determination of body fat by computed tomography. Int J Obes 7:437–445
Allison GT, Singer KP, Marshall RN (1995) The effect of body position on bioelectrical resistance in individuals with spinal cord injury. Disab Rehab 17(8):424–429
Cornish BH, Thomas BJ, Ward LC (1993) Improved prediction of extracellular and total body water using impedance loci generated by multiple frequency bioelectrical impedance analysis. Phys Med Biol 38:337–346
Fujioka S, Matsuzawa Y, Tokunaga K, Tarui S (1987) Contribution of intra-abdominal fat accumulation to the impairment of glucose and lipid metabolism in human obesity. Metabolism 36(1):54–59
Acknowledgements
This work was supported by the ERC program of MOST/KOSEF. (Grant R11-2001-094-03001-0)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hong, K.H., Lim, Y.G. & Park, K.S. Effectiveness of thigh-to-thigh current path for the measurement of abdominal fat in bioelectrical impedance analysis. Med Biol Eng Comput 47, 1265–1271 (2009). https://doi.org/10.1007/s11517-009-0551-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-009-0551-z