
Abstract
Bioelectrical fetal heart activity being recorded from maternal abdominal surface contains more information than mechanical heart activity measurement based on the Doppler ultrasound signals. However, it requires extraction of fetal electrocardiogram from abdominal signals where the maternal electrocardiogram is dominant. The simplest technique for maternal component suppression is a blanking procedure, which relies upon the replacement of maternal QRS complexes by isoline values. Although, in case of coincidence of fetal and maternal QRS complexes, it causes a loss of information on fetal heart activity. Its influence on determination of fetal heart rate and the variability analysis depends on the sensitivity of the heart-beat detector used. The sensitivity is defined as an ability to detect the incomplete fetal QRS complex. The aim of this work was to evaluate the influence of the maternal electrocardiogram suppression method used on the reliability of FHR signal being calculated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The recording of electrical activity of fetal heart succeeded for the first time in 1906 by the use of intravaginal and abdominal electrodes connected to a simple string galvanometer. For many subsequent years, technical difficulties in recording and processing of abdominal signals hindered the development of fetal electrocardiography. Progress in electronics, application of new technologies in electrodes, and first of all widespread application of personal computers together with digital signal processing software allowed improving the quality of signals recorded (Horoba et al. 2004). The main advantage of the method based on acquisition of the signals from electrodes placed on maternal abdomen is its noninvasiveness. This method can be practically applied from the 16th week of gestation (Jezewski et al. 2002b).
Monitoring of the mechanical activity of fetal heart via ultrasound is performed using Doppler shift effect of ultrasound beam reflected from moving valves of a fetal heart (Jezewski et al. 2002a). However, the distance from a given event in the cardiac cycle to the same point in the next cycle is just the T RR interval equivalent. Thus, the higher accuracy of FHR determination can be ensured by using the abdominal electrocardiography (Peters et al. 2001). Additionally, this allows the morphology analysis of the fetal electrocardiogram (FECG) and thus improves the efficiency of diagnosis being made (Rosen 2001).
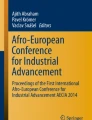
Signals recorded from maternal abdomen (Fig. 1a) besides the useful component—the fetal electrocardiogram—also contain artefacts: the maternal electrocardiogram (MECG), mother’s muscles activity or artefacts resulting from fetal movements. Essential problem is the efficient suppression of maternal electrocardiogram, since its amplitude many times exceeds the level of the useful signal. In our studies, the averaged MECG amplitude was approximately 300 μV, whereas the FECG amplitude of 10/20 μV was comparable to the muscular artefacts in some cases (Jezewski et al. 2002b). In addition, the frequency bands of maternal and fetal electrocardiographic signals overlapped which makes the application of simple filtration impossible. Maternal QRS complex covers the frequency range from 10 to 40 Hz, whereas the fetal QRS complex just starts from 20 Hz. The process of overlapping of these frequency bands is shown in Fig. 1 comprising a fragment of raw signal recorded from maternal abdomen (a), and result of its analysis in joined time-frequency domain (b). Analysis was carried out using the LabView JTFA Toolkit (National Instruments, USA). The short-time Fourier transform was applied with a Hanning window (48 samples wide) shifted with every new sample. Sampling frequency of input electrocardiogram was 500 Hz. The intersection of plot b at the level of 30 Hz corresponding to the maximal peak in the power spectrum of fetal QRS is presented on the plot c. Amplitude in the part b and c has been normalized in relation to the maximum energy of maternal electrocardiogram.

Process of overlapping of frequency bands of fetal and maternal components in the abdominal signal
It can be noted that even for the frequency corresponding to the highest peak of power spectrum of fetal QRS complex, the maternal electrocardiogram is still a dominant component in the abdominal signal (Fig. 1c). It makes the suppression of MECG by the frequency separation impossible, because it may lead to full suppression of FECG as well.
Thus, the separation of the FECG signal requires more complex algorithms to be applied. They are usually based on adaptive filtration (Widrow et al. 1975), weighted summation of signals (Bergveld et al. 1981) and spatial filtration (Callaerts et al. 1990; Kanjilal et al. 1997). Their basic shortcoming is the necessity of recording of relatively large number of abdominal signals and sometimes also signals from maternal chest leads. Very often they require strictly determined configuration of electrodes on maternal body that is usually difficult to accomplish during the labour. The method developed by us, which is based on a subtraction of averaged maternal P–QRS–T complex and its derivative, not has the disadvantages mentioned above (Matonia et al. 2003). However, this method requires a large computational time that makes it impossible to use in instrumentation for longitudinal monitoring of fetal heart rate. Therefore, we decided to find MECG suppression algorithm the most suitable for longitudinal (even for 24 h) monitoring and for analysis of fetal heart rate variability. The simplest one seems to be a blanking procedure for the removal of interfering maternal QRS complexes (Pieri et al. 2001). The aim of this work was to evaluate the influence of this maternal electrocardiogram suppression method on the reliability of the FHR signal being calculated.
2 Methods
In the blanking method, with every maternal QRS complex detected, the corresponding segment of abdominal signal is replaced by the isoline values. The detection of maternal QRS complexes is quite simple, since they keep the major energy of the signal recorded from the abdominal wall. This can be accomplished by the threshold detection where the instantaneous amplitude of the abdominal signal, after preliminary filtration of low frequency and power line interferences, is compared with the threshold undergoing adaptive modification during monitoring. Unfortunately, in any case of coincidence of maternal and fetal QRS complexes, the blanking leads to some information loss in FECG signal (Fig. 2). It is obvious when a whole fetal QRS complex is overlapped by the maternal one then the information on the fetal heart-beat will be lost. However, in most cases, only the part of the fetal QRS complex is overlapped. Therefore, the sensitivity of the detector used, which has been defined as an ability to detect incomplete fetal QRS, is crucial.

Segment of abdominal signal (a) with fetal electrocardiogram extracted using two methods for suppression of maternal electrocardiogram: subtraction (b) and blanking of maternal QRS complexes (c)
The proposed method has been developed with the use of generator of artificial signals simulating waveforms recorded on the abdominal wall. It enabled generation of electrocardiographic signals with strictly determined parameters. Both the maternal and the fetal electrocardiograms were generated using the first three Hermit functions (Matonia et al. 2005a). These functions can be adapted to model the QRS complexes as well as the P and T waves constituting the single cardiac cycle. The complete electrocardiograms of different parameters (Table 1) were created by repetition of the generated cardiac cycle with certain heart rate (Fig. 3). Sampling frequency has been set up at 500 Hz corresponding to the frequency used in our system for acquisition and analysis of signals from the maternal abdominal surface (Horoba et al. 2004).

Fragment of artificially generated electrocardiographic signal together with its description parameters. RND generator of pseudo-random numbers describing the variability of maternal and fetal heart rate, respectively
The signals were generated in the following way: the beat-to-beat variability was added to the constant (for a given signal) base values of maternal and fetal intervals (T M and T F). The pseudorandom generator of a normal distribution was used to generate the beat-to-beat variability, since the real signals are characterized by such type of distribution. The variation range resulting from physiology of a heart activity is specified by the variables ΔT M(i) and ΔT F(i). Due to variability of the heart rate, the phase shift between signals of mother and fetus is not essential; hence, it has not been regarded in our algorithm. Database containing 1,050 signals was created by combination of the parameters presented in Table 1. In a single trace of 5 h length the number of maternal QRS complexes varied from 18,000 to 36,000 while the number of fetal complexes were from 30,000 to 60,000.
The acceleration and deceleration patterns as well as other trends, which can occur in real signals, did not take a part in the generating process. It was necessary for the evaluation of the influence of the base value of fetal T RR interval on the complexes’ coincidence events. From the other hand, it can be expected that being long-term patterns they are insensitive to signal loss caused by the blanking method. It results from the fact that lost samples in the FHR signal do not constitute continuous segments of significant duration but they occur rather singularly from time to time dependently on electrocardiogram parameters. Such characteristic of the signal loss does not influence the shape of acceleration and deceleration. Additionally, the averaging process over 2.5 s periods is performed which corrects the lost samples. This input signal is required by the filtering algorithms for estimation of the FHR baseline which is necessary for the recognition of acceleration and deceleration.
There are two aspects essential for the fetal QRS complexes’ detection when the blanking method is used for suppression of maternal complexes: (1) how often does the coincidence of fetal and maternal QRS complexes occur in the abdominal signal? (2) how large part of the fetal complex is not overlapped by the maternal complex when the coincidence occurs? It can be expected that various fetal QRS detection algorithms are able to detect such incomplete QRS with different sensitivity. The part of fetal QRS complex remaining unchanged after application of the blanking method, and expressed as a percentage of the complex width has been named the rest component. Four classes (C) defining the lower limit of rest component have been considered: 25, 50, 75 and 100%. For example, the class C of 75% comprises all complexes in a given signal whose width after the overlapping has been at least 75% of their original width (Fig. 4).

Definition of C classes concerning the rest component of fetal QRS complex
The coincidence coefficient (CF) has been defined for the quantitative evaluation of the percentage of the fetal QRS complexes that preserved their assumed rest part during the coincidence events in a given signal:
where:
-
C class limiting the size of the rest component of QRS (25, 50, 75, 100%)
-
N number of all fetal QRS complexes in the signal
-
\({\text{CR(}}i{\text{)}} = \left\{ {\begin{array}{*{20}c} {1} & {{\begin{array}{*{20}c} {{\quad {\text{if}}}} & {{{\text{CP}}(i) \ge C}} \\ \end{array} }} \\ {0} & {{\begin{array}{*{20}c} {{{\text{otherwise}}}} & {{}} \\ \end{array} }} \\ \end{array} } \right.\) marker of class membership
-
\({\text{CP(}}i{\text{)}} = \frac{{{\text{QRS}}^{{\text{R}}}_{{\text{F}}} (i)\;[{\text{ms}}]}} {{{\text{QRS}}^{{}}_{{\text{F}}} \;[{\text{ms}}]}}\; \cdot \;100\%\) the rest component of the i-th fetal QRS complex
-
QRS RF (i) width of the i-th fetal QRS complex after blanking
-
QRSF width of original fetal QRS complex (constant in a given signal).
In the next stage of this work, the sensitivity of fetal heart-beats detector has been evaluated considering incomplete fetal QRS complex. The perfect detection function should response with single positive peak to the occurrence of every QRS complex and its maximum should correspond to the R wave. This function should not generate such peaks for any other waves of electrocardiogram as well as for possible interferences (Kohler et al. 2002). Two approaches for determination of the detection function have been proposed (Afonso 1993; Pan and Tompkins 1985). The first approach (DFD) is based on linear combination of the first and the second derivative of the FECG (the weight coefficients have been set empirically at w 1 = 1 and w 2 = 2). Before the derivatives are determined, the FECG is preliminary filtered using a low-pass Bessel filter of the second order and cut-off frequency of 60 Hz. The second approach (DFF) relies upon linear filtration, the aim of which is to suppress dominating interferences, thanks to its adaptation to the frequency band of QRS complex exclusively (middle frequency of 27 Hz and bandwidth of 24 Hz).
Two detection functions were analysed in order to detect all peaks corresponding to fetal QRS complexes. Preliminary peaks detection was accomplished by comparison of the detection function amplitude with established and continuously adjusted detection threshold. Additionally, some improving modifications were made (Matonia et al. 2005b). The detector was put to an inactive state for certain time period after a peak was found. The threshold value was adjusted when the amplitude decreased and repeated searching was carried out when the peak was not found in the expected localization. The decision rule to validate the detection function peak as corresponding to the true QRS complex was set on the basis of the physiological range of T RR variation. Any invalid interval (for example of double value) is excluded from further processing and then the signal loss is marked in FHR signal.
For the evaluation of the ability of the detector to recognize the incomplete fetal QRS complex, we generated three signals of different noise level in relation to the useful component SNR: −10, 0, 10 dB (Fig. 5). The length was 10 min, and for the fixed FHR value of 135 bpm, it provided 1,350 QRS complexes. The noise was defined as a sum of the low-frequency, power line and muscles’ signals. The low-frequency interferences were modelled using the 0.5 Hz sinusoid waveform, whereas the power line interferences were modelled using the 50 Hz sinusoid. The phase shift was a random value of the regular distribution from the range 〈−π, + π〉. Harmonic components of the power line interference were not modelled, because the 50 Hz component is usually the dominant one. The muscular activity interferences were modelled by the Gaussian white noise (Friesen et al. 1990; Matonia et al. 2005a). In the obtained signals, the distortion of the fetal QRS complex being normally caused by the application of blanking method was simulated by removing the same fragment from each of the fetal QRS complex in a given signal. The size of the rest component was constant for a given signal, but it was changed a step of 10% for the consecutive generated signals. Finally, we obtained 27 testing signals.

Generated fetal electrocardiograms with a different noise level
For each signal, the detection efficiency (DE) defined as a percentage of the detected QRS complexes to their overall number was determined. The given complex was marked as detected if the difference between its localization and the reference one did not exceed a half of the complex width. Additionally, for the correctly detected complexes the detection error ΔR (mean value and standard deviation) expressed in milliseconds was calculated.
3 Results
The calculations were done for all 1,050 signals generated. Table 2 presents CF values calculated for C = 75% and for variable maternal and fetal cardiac intervals and constant (boundary) values of the width of maternal and fetal QRS complexes. Obtained results confirm that minimum and maximum correspond to the boundary values of intervals. This tendency does not change itself for any other combinations of maternal and fetal QRS width as well as for particular C classes.
It appeared that the change of the base fetal interval does not influence the value of coincidence coefficient CF for a given width of the maternal and fetal QRS complexes as well as for a given length of base maternal interval T M (Tables 2, 3). This is caused by the fact that change of the T F influences both the number of these intervals in the signal and the probability of complexes’ coincidence.
As it could be expected, the electrocardiographic parameters relating to the mother (T M, QRSM) had the strongest influence on the coincidence coefficient. This results directly from the wide range of their values. Generally, the increase of CF coefficient can be noted as the length of maternal beat-to-beat interval increases and the width of maternal QRS complex decreases. Such tendency increases the probability that fetal QRS will not overlap with maternal QRS at all or it will overlap but with smaller degree. The influence of the width of fetal QRS complexes on the CF is very small, but more complex than for the maternal parameters.
For the class of 25%, an increase of CF can be observed together with increase of fetal complex width. However, for C = 50% when fetal QRS width changes, the value of CF coefficient is practically constant, but for classes of 75 and 100% the increase of QRSF width causes a decrease of CF value. Origin of this relation is explained in Fig. 6. For the class of 25%, if the CP value of the fetal QRS complex being considered is slightly lower than the class value, an increase of the QRSF causes an increase of the CP value above 25%, and as a result adds this fetal complex to the class considered (CR = 1). For the class of 75%, the tendency is opposite. The increase of the width of fetal QRS complex belonging to this class (CP = 78%) leads to excluding this complex from the class, since the CP decreases to the value of 70% (CR = 0).

The influence of a change of fetal QRS width on the coincidence coefficient CF value illustrated for two classes of incomplete fetal QRS complexes
It can be noted that the CF value in a signal decreases when the size of required remaining part of fetal QRS complex increases (Fig. 7). Using the determined CF and having the QRS detector with a known ability to detect incomplete complexes of a given size, we can evaluate the signal loss in the final FHR signal. For example, if the detector is able to recognize the complexes, the rest component of which are not lower than 75%, then depending on the parameters of the electrocardiographic trace we can detect 75.6–92.9% of the complexes. But for trace parameters close to the typical values, the number of complexes detected is expected to be around 86%. This value does not comprise the influence of other interferences being present in electrocardiogram.

Range of changes of coincidence coefficient CF for various class C describing the rest component of fetal QRS as a result of maternal and fetal QRS complex coincidence. Filled square minimal value of CF; filled triangle maximal value; filled circle CF value for typical physiological abdominal signal
Detailed results of evaluation of fetal QRS detection efficiency in relation to different noise level and different size of the rest component of the fetal QRS complex are presented in Table 4. When the noise level was low (SNR = 10 dB), both detectors were able to detect all complexes, even if their rest component was small (CP did not exceed 30%). However, such a large distortion of fetal QRS complex led to a very large detection error ΔR equal to 9.97 ± 0.24 ms for the DFD and 9.14 ± 3.32 ms for the DFF. These values do not differ with statistical significance. For both methods, the mean detection error calculated for the signals of CP ≥ 50% was statistically different from the signals of CP < 50%. Additionally, for a given rest component, an increase of the detection error caused by noise increase is not statistically significant. There is no such tendency when ΔR is accompanied with low detection efficiency (DE < 10%). Then these results are unreliable because of the small number of detected complexes. For high noise level (SNR = −10 dB), the rapid decrease of the detection efficiency was noted when size of the rest component dropped below 50%. It is caused by the fact that the signal slope around the R wave is the largest, and thus a slight decrease of the rest component can imply a significant decrease of the signal amplitude to the value comparable or even smaller than the noise level.
Generally, worse results, as regards both efficiency and mean detection error, were obtained for the detector relying linear filtration of fetal electrocardiogram (DFF). This is a result of a change of QRS frequency parameters caused by the decrease of the size of the rest component of complex. Thus, the detector based on bandpass filtration with the middle frequency of 30 Hz will be less sensitive to QRS complexes being distorted in such a way.
We can see that if the DFD is used for the signal with the rest component of 50%, the ΔR error takes a very low value. It is caused by the fact that in the generated signals the R wave was the middle point of fetal QRS complex. Therefore, when a half of fetal QRS complex is removed, the slope of the R wave reaches a maximum value and thus the derivative function in this point takes also the maximum. It is worth to emphasize that, although for the rest component below 50% the ΔR error is large, its dispersion in signals is rather small and resulted from the noise added.
The rest component being the half of the original complex is the boundary value, for which the detector based on derivatives of fetal electrocardiogram is able to detect all fetal QRS complexes. Above this value the error slightly increases but it still keeps the acceptable value. However, the percentage of complexes being in the C class of 50% is in the range from 79.6 to 93.9% (Fig. 7). For the electrocardiogram parameters close to typical values, the number of detected complexes fluctuated around 88%. It should be marked that a loss of one QRS complex causes a loss of information on two T RR intervals and consequently on two FHR values. Thus, the FHR signal loss will be about 24%.
Fortunately, in real signals the lost heart-beats do not constitute the continuous segment but occur randomly and thus the single lost cardiac intervals can be interpolated with correct neighbouring values. Figure 8 presents 1 min fragment of FHR signal obtained from real electrocardiographic signal, where maternal QRS complexes have been eliminated using blanking (a) and by subtraction of reference maternal QRS complex (b). The detection of QRS complexes was accomplished by the algorithm based on linear combination of derivatives.

One-minute segments of FHR signal determined from fetal electrocardiogram, the first one (a) is with large signal loss resulted from the blanking method. The segment (b) of a good quality is obtained by subtraction of reference maternal QRS complex
According to our assumptions, after samples averaging over 2.5 s periods the influence of the blanking method on evaluation of long-term patterns is insignificant (Fig. 9). The FHR baseline was estimated using nonlinear bidirectional filter. Relying on this baseline, the clinically important patterns—accelerations and deceleration of fetal heart rate—were detected. The mean value of differences between corresponding samples was equal to 0.01 ± 0.26 bpm (−0.02 ± 0.74 ms), but due to the averaging the signal loss resulting from the blanking method did not affect the shape of FHR trace, and acceleration patterns could be correctly determined.

Six-minute segments of FHR signal periods obtained from fetal electrocardiogram after using simple blanking method (a) and technique of subtraction of reference maternal QRS complex (b). On the right side is given parameters of accelerations recognized and values of difference of FHR inside the acceleration pattern. Segments marked with grey are shown as enlarged in Fig. 8
Mathematical indices describing the FHR variability provide very important and clinically useful information for fetal well-being assessment. They are defined on a basis of intervals between consecutive heart-beats. We have stated that FHR signal loss exceeding 20% significantly changes values of these indices and they cannot be used for fetal-state assessment (Jezewski et al. 2006; Wrobel 2001). Therefore, the signal loss in FHR signal resulting from the application of the blanking method makes the beat-to-beat analysis unreliable. For example, in the relevant fragment presented in Fig. 8a the signal loss reached 21.6%.
4 Discussion and conclusions
In the work, the influence of the coincidence events on the number of fetal QRS complexes remaining detectable has been evaluated with regard to the different grade of maternal and fetal QRS overlapping, e.g. for different coincidence class. For this purpose the abdominal signal generator has been created, which input parameters (heart rate and QRS width) enabled us to control the coincidence of QRS complexes. For a given fetal QRS detector, the boundary width of incomplete fetal QRS complex has been evaluated, for which the signal loss remained on the acceptable level. The results obtained have made it possible to evaluate the loss of information that can be expected to occur in real FECG traces when the blanking method together with a given fetal QRS detector are used.
It is very difficult to find other works which would be close to ours and thus let us to validate our results. Even if some work concerns the problems of MECG suppression, rather sophisticated methods are evaluated which are based on wavelet-transform or independent components analysis. Such algorithms are completely useless for on-line longitudinal ambulatory fetal monitoring. In addition, these works do not test the influence of suppression methods on the efficiency of fetal QRS detection. Comparing several detection methods Azevedo and Longini (1980) concluded that their performance depends on precise choice of the threshold level in the detection functions. The method using digital filtration (filter matched to fetal QRS frequency spectrum) appeared to be the least sensitive.
Kotas (1995, 1996) compared the efficiency of various fetal QRS detection function. He focussed on the three different linear operations: digital filtration, matched filtration and operation based on summation of absolute differences. The efficiency of the fetal QRS detection was evaluated using a small group of real signals, where QRS complexes were marked manually. The performance index (96.26%) considering the number of true-negative and false-positive detections showed that the best results were provided by matched filtration combined with expanded decision rules. There was no type of algorithm based on signal derivative, which provided best results in our study.
In our study, we tried to evaluate FHR loss level caused by application of the blanking method for suppression of maternal electrocardiogram. Therefore, we calculated the efficiency DE of the detector tested in the same way like in (Friesen et. al. 1990), and additionally mean detection error ΔR. We chose two fundamental detection functions which were based on derivative and filtration of electrocardiogram (Afonso 1993; Pan and Tompkins 1985). We did not consider a detection of false-positive fetal QRS complexes, because their origin is connected rather with high noise level and not with application of the blanking method. It should be emphasized that testing the influence of noise level on the detection efficiency was not the aim of our work.
Abdominal fetal electrocardiography is a diagnostic method being still under development. However, it may have a significant impact on the perinatal medicine in the near future. The portable monitoring system based on the abdominal fetal electrocardiography together with a telemetry technique seems to be the best approach for on-line longitudinal monitoring of a pregnant woman. This enables analysis of the circardian and ultradian rhythm of the fetal heart rate, which is expected to improve the fetal well-being assessment. The commonly used cardiotocography should not be applied for 24 h monitoring, since the energy of ultrasound beam is not safe for the fetus for such a long period. Additionally, a power consumption of the ultrasound-based system is rather high, which causes some problems relating to battery supply of the portable system.
The most significant problem is the extraction of the useful component—fetal electrocardiogram—from the abdominal signal, where the dominating components are the maternal electrocardiogram and muscle interferences. There are many methods of maternal electrocardiogram suppression; however, the required computational effort makes their use difficult in the system for longitudinal monitoring of the fetal heart rate. The best solution seems to be the use of the blanking method relying on the replacement of the previously detected maternal QRS complexes by the isoline values. Unfortunately, in the case when a whole fetal QRS complex is overlapped by the maternal one, the information on the fetal heart-beat will be lost. Usually, the overlapping of the fetal complex is partial and then detection of a given fetal heart-beat depends on the sensitivity of the detector used, which is defined as an ability to detect the incomplete fetal QRS complex.
We noted that the method based on the linear combination of the derivatives of fetal electrocardiogram is able to detect all fetal QRS complexes for which the size of the rest component is at least 50% of the original size even with high noise level. We estimated how often the coincidence of fetal and maternal QRS complexes occurs in the abdominal signal, and thus we can say that for the electrocardiograms close to physiological ones (T M = 700 ms, QRSM = 80 ms) 88% of complexes being in class of 50% will be detected when the blanking method and the detector based on the signal derivatives are used. This corresponds to the FHR signal loss of 24%.
Detailed analysis of the fetal heart rate variability is based on clinically important quantitative measures—the so-called short- and long-term variability indices. These indices are calculated automatically over 1 min FHR segments. The FHR signal loss exceeding 20% makes the variability indices unreliable from clinical point of view. We showed that just the blanking method itself causes FHR signal loss above 20% almost for all conditions. This makes assessment of FHR variability on the beat-to-beat level rather impossible.
However, for longitudinal ambulatory fetal monitoring, it is enough to perform classical analysis of FHR which includes baseline estimation, recognition of tachycardia and bradycardia, as well as detection of accelerations and decelerations. Such range of analysis corresponds to the visual assessment of the paper FHR trace, which is done by a clinician. Algorithm for the baseline estimation needs FHR samples being averaged over 2.5 s intervals. Thus the influence of the MECG suppression method on the FHR shape is insignificant, and consequently all the above-mentioned signal patterns can be successfully recognized.
The results obtained in the paper should be verified using a database of real signals. Unfortunately, there are no such database with fetal electrocardiograms and accompanied detailed interpretation from clinical experts. These databases are available only for adult ECG (MIT-BIH, AHA). Currently, we are working on representative FECG database, but it requires a lot of time and great effort.
Abbreviations
- ΔR :
-
Detection error of the R wave
- ΔT F :
-
Variation of fetal T RR duration
- ΔT M :
-
Variation of maternal T RR duration
- C :
-
Class of rest component
- CF:
-
Coincidence coefficient
- CP:
-
Rest component of the fetal QRS complex
- CR:
-
Marker of class membership
- DE:
-
Percentage of the detected QRS complexes to their overall number
- DFD :
-
Detection function based on combination of derivative of the FECG
- DFF :
-
Detection function based on linear filtration of the FECG
- FECG:
-
Fetal electrocardiogram
- FHR:
-
Fetal heart rate
- JTFA:
-
Joined time-frequency analysis
- MECG:
-
Maternal electrocardiogram
- N :
-
Number of all fetal QRS complexes in the signal
- QRSF :
-
Width of fetal QRS complex
- QRS RF :
-
Width of the fetal QRS complex after blanking
- QRSM :
-
Width of maternal QRS complex
- SNR:
-
Signal to noise ratio
- T F :
-
Base value of fetal T RR interval
- T M :
-
Base value of maternal T RR interval
- T RR :
-
Time interval between two consecutive R waves
References
Afonso VX (1993) ECG QRS detection. In: Tompkins WJ (eds) Biomedical digital signal processing. PTR Prentice-Hall, Englewood Cliffs, pp 236–264
Azevedo S, Longini RL (1980) Abdominal-lead fetal electrocardiographic R-wave enhancement for heart rate determination. IEEE Trans Biomed Eng 27:255–260
Bergveld P, Meijer WJH (1981) A new technique for the suppression of the MECG. IEEE Trans Biomed Eng 28:348–354
Callaerts D, De Moor B, Vandewalle J, Sansen W (1990) Comparison of SVD method to extract the fetal electrocardiogram from cutaneous electrode signals. Med Biol Eng Comput 28:217–224
Friesen GM, Jannett TC, Jadallah MA, Yates AL, Quint SR, Nagle HT (1990) A comparison of the noise sensitivity of nine QRS detection algorithms. IEEE Trans Biomed Eng 37:85–98
Horoba K, Jezewski J, Matonia A, Gacek A, Bernys M, Wrobel J (2004) Fetal monitoring based on bioelectrical signals from maternal abdomen. Proc IFMBE LA Biomed Eng 5:1207–1210
Jezewski J, Horoba K, Wrobel J, Sikora J, Gacek A, Matonia A, Kupka T (2002a) Monitoring of mechanical and electrical activity of fetal heart: determination of the FHR. Arch Perinat Med 8:33–39
Jezewski J, Wrobel J, Horoba K, Cholewa D, Gacek A, Kupka T, Matonia A (2002b) Monitoring of mechanical and electrical activity of fetal heart: the nature of signals. Arch Perinat Med 8:40–46
Jezewski J, Wrobel J, Horoba K (2006) Comparison of doppler ultrasound and direct electrocardiography acquisition techniques for quantification of fetal heart variability. IEEE Trans Biomed Eng 53 (in press)
Kanjilal PP, Palit S, Saha G (1997) Fetal ECG extraction from single-channel maternal ECG using singular value decomposition. IEEE Trans Biomed Eng 44:51–59
Kohler BU, Hennig C, Orglmeister R (2002) The principles of software qrs detection—reviewing and comparing algorithm for detecting this important ECG waveform. IEEE Eng Med Biol Mag 21:42–57
Kotas M (1995) The investigation of QRS complex detection algorithms applied to fetal ECG signal. In: Proceedings of the international conference “SYMBIOSIS”, pp 104–106
Kotas M (1996) Fetal QRS detection-quantitative investigation of a class of algorithms. Biocybern Biomed Eng 16:133–145
Matonia A, Jezewski J, Kupka T, Horoba K, Wrobel J (2003) Algorithm for recognition and suppression of interfering maternal electrocardiography. In: Proceedings of the computer recognition systems, pp 55–61
Matonia A, Jezewski J, Kupka T, Horoba K (2005a) Modelling of noninvasively recorded maternal and fetal electrocardiographic signals. Biocybern Biomed Eng 25:27–39
Matonia A, Kupka T, Jezewski J, Horoba K (2005b) Evaluation of the QRS detection algorithms in relation to fetal heart rate estimation. In: Proceedings of the IFMBE 11 1709, pp 1–5
Pan J, Tompkins WJ (1985) A real-time QRS detection algorithm. IEEE Trans Biomed Eng 32:230–236
Peters MJ, Crowe JA, Pieri JF, Quartero H, Hayes Gill BR, James D, Stinstra JG, Shakespeare S (2001) Monitoring the fetal heart non-invasively: a review of methods. J Perinat Med 29:408–416
Pieri JF, Crowe JA, Hayes Gill BR, Spencer CJ, Bhogal K, James DK (2001) Compact long-term recorder for the transabdominal fetal and maternal electrocardiogram. Med Biol Eng Comput 39:118–125
Rosen KG (2001) Intrapartum fetal monitoring and the fetal ECG—time for a change. Arch Perinat Med 7:7–12
Widrow B. Glover JR, McCool JM, Kaunitz J (1975) Adaptative noise cancelling—principles and applications. Proc IEEE Inst Electr Electron Eng 63:1692–1716
Wrobel J (2001) Evaluation of accuracy of fetal heart rate variability parameters in respect to registration methods: ultrasound and electrocardiography. PhD Thesis, Poznan University of Medical Sciences
Acknowledgment
Scientific work financed from the State Committee for Scientific Research resources in the years 2004–2006 as a research project No. 3 T11E 01726. Adam Matonia is a fellowship holder of the Foundation for Polish Sciences
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Matonia, A., Jezewski, J., Kupka, T. et al. The influence of coincidence of fetal and maternal QRS complexes on fetal heart rate reliability. Med Bio Eng Comput 44, 393–403 (2006). https://doi.org/10.1007/s11517-006-0054-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-006-0054-0