
Abstract
The aim of this study was to analyse the trends of the first three power spectral moments of the mechanomyogram (MMG) signal recorded by a microphone (MMGMIC) and an accelerometer (MMGACC) during sustained contractions. MMG signals were recorded from the biceps brachii muscle in 14 healthy male subjects during a 3 min isometric elbow flexion at 30% of the maximal voluntary contraction. MMG absolute and normalised root mean square (RMS), mean power frequency (MNF), power spectral variance (Mc2), and skewness (μ3) were computed. For both MMGMIC and MMGACC, absolute and normalised RMS and Mc2 increased while MNF and μ3 decreased with contraction time (P<0.001). The rates of change of RMS over time were significantly correlated (P<0.001) for MMGMIC and MMGACC but not correlated for spectral moments. The coefficient of variation of RMS was higher for MMGMIC than for MMGACC, while the opposite was observed for μ3 (P<0.05). It was concluded that higher order spectral moments of the MMG signal change during sustained contraction, indicating a complex modification of the shape of the power spectrum and not just scaling of the bandwidth. This is most likely due to the additional motor unit recruitment with fatigue and to the non-linear summation of motor unit contributions to the signal. Moreover, the characteristics of MMG signals recorded with microphones and accelerometers have important differences, which should be taken into account when comparing results from different studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Slow bulk movement of the muscle, excitation into ringing of the muscle at its own resonance frequency [1, 5], and pressure waves due to the dimensional changes of the active muscle fibres [15] generate oscillations recorded as the mechanomyogram (MMG) signal. MMG has been used to study the mechanical activity of a contracting muscle and may reflect motor unit recruitment, discharge rate, synchronisation and, to some extent, factors which affect the muscle physical milieu, such as intra-muscular pressure, stiffness, and osmotic pressure [15, 16].
Over the last two decades, several types of transducers have been applied to detect MMG signals, including piezoelectric contact sensor, microphones, accelerometers, and laser distance sensors. Piezoelectric contact sensors are not commonly used since their weight and the applied pressure to obtain a mechanical coupling damp the recorded MMG signal [16]. Condenser microphones acting as a displacement meter are more often applied but, as the piezoelectric contact sensors, they require a coupling, for example, air, gel between the muscle and the microphone [21]. The volume of the air chamber influences the amplitude and the frequency content of the recorded MMG signal [21]. Accelerometers, reflecting the acceleration of body surface vibration, are currently the most applied sensors for MMG recording due to their small weight and size, easy attachment, and high reliability [22]. Recently, laser displacement sensors have also been used since it is possible to study muscle dimensional changes without additional inertial load [16, 19]. However, accelerometers weighting less than 5 g do not interfere with muscle surface dynamics and provide accurate MMG recordings [22]. Due to different transduction modes inherent to the various sensors, MMG signals have different temporal and frequency characteristics [21]. However, there are no reports comparing the features of MMG signals recorded with different sensors during sustained isometric contractions.
During sustained isometric contractions at forces above 30% of the maximum voluntary contraction (MVC), time-domain MMG signal descriptors, such as root mean square (RMS), usually increase while characteristic power spectral frequencies, for example, mean frequency (MNF), decrease [6, 9, 10, 15, 20]. The first-order spectral moment provides full description of the relative changes in the power spectrum during sustained contraction if the shape of the spectrum does not change, that is, if only a compression of the bandwidth occurs. This assumption is usually done in electromyographic recordings [13], but it is likely not valid in MMG recordings, due to the complex non-linear summation of the single motor unit contributions [18]. However, there are no studies that investigated changes in higher order spectral moments of MMG signals during sustained contractions.
Therefore, the aim of this study is to analyse the trends of the first three power spectral moments of the MMG signal recorded concomitantly by a microphone and an accelerometer during sustained contractions.
2 Methods
2.1 Subjects
Fourteen healthy male volunteers (right-handed) without any history of neuromuscular or orthopaedic diseases participated in the study (age, mean ± SD: 26.7±4.9 years, body weight: 76.3±9.5 kg, height: 1.80±0.07 m). Informed consents were obtained from all participants. The study was conducted in conformity with the Declaration of Helsinki.
2.2 MMG signal recordings
The MMGMIC signal was detected by an air-coupled condenser microphone (type BCM 9765, BeStar Acoustic, Jiangsu, China; diameter 9.7 mm, weight 18 g, 54 dB sensitivity where 1Pa=7 mV, linear transmission in the frequency range 0.1–5,000 Hz). The distance from the microphone to the skin surface was 9 mm. The MMGMIC signal was amplified at 1–20, band-pass filtered at 1–500 Hz, sampled at 1 kHz, and converted in numerical format with a 14-bit A/D board (Analogue Devices, Norwood, MA).
MMGACC was recorded by a piezoelectric accelerometer (Bang & Olufsen Technology, Struer, Denmark; diameter 17.6 mm, weight 2.9 g, sensitivity 30 pC/m·s−2, linear transmission in the frequency range of 0.1–800 Hz). The MMGACC signal was amplified (Bruel & Kjær Nexus, Nærum, Denmark) in the bandwidth 0.1–100 Hz, sampled at 1 kHz, and digitised on 12 bits (National Instrument, Austin, TX, USA).
The two MMG transducers were attached with double-sided adhesive tape over the biceps brachii muscle, adjacent with respect to each other, along the line between the acromion and the fossa cubit. The accelerometer was placed 31 mm distal to the condenser microphone in order not to cover the end plate zone or to get too close to the musculotendinous region and to measure MMG with the two transducers from the same part of the muscle relative to the innervation zone.
Prior to data analysis, MMGACC and MMGMIC signals were off-line digitally band-pass filtered with bandwidth 2–100 Hz (second-order, anti-causal Butterworth filter).
2.3 General procedures
The subject sat comfortably in an upright position on a chair with his left arm along the trunk and the right forearm 90° flexed with respect to the arm. The forearm was in a neutral position (semi pronated) and supported on a table. A belt was fastened around the wrist and connected to a piezoelectric force transducer (Kistler type 9311A, Bern, Switzerland), fixed to the floor.
The subject performed three 5 s maximal voluntary isometric elbow flexions, with 2 min rest in between. The trial resulting in the highest force was considered as the MVC. After 5 min rest, the subject exerted a 3 min right elbow isometric flexion at 30% MVC (Fig. 1) corresponding to approximately 50% of the endurance time [24]. The subjective score of fatigue was indicated by the subject after the sustained contraction on a 10 cm visual analogue scale, where 0 cm indicated ‘no fatigue’ and 10 cm ‘exhaustion’.

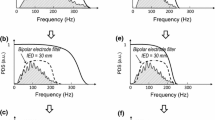
Example of MMGMIC and MMGACC signals and power spectral density (PSD) at the beginning and end of a 3 min sustained isometric contraction at 30% maximum voluntary contraction
2.4 Data processing
The RMS value of the MMG signals from the three MVC trials was computed over 1 s epochs with 100 ms overlap. The maximum RMS value was used for normalisation. RMS, first-, second-, and third-order spectral moments were computed over non-overlapping 1 s long epochs from the MMG signals recorded during the sustained contractions. The power spectral density (Fig. 1) was computed with Welch periodogram with Hanning window and zero-padding to 1,024 samples [23]. The first-order moment (MNF) is defined as
where PSD i is the ith line of the power spectral density and N is the highest harmonic considered.
The second-order central moment (Mc2), that is, the variance of the power spectral density, and the normalised third central moment (μ3), that is, the skewness, are defined as
Absolute RMS values and normalised (with respect to MVC) RMS values were used for further analysis. Spectral moments were analysed as absolute values and as values normalised to the initial value. To decrease variability and reduce the amount of data, mean and standard deviation of absolute and normalised RMS, MNF, Mc2, and μ3 values were computed over sets of 10 consecutive values (without overlapping). The coefficient of variation of RMS, MNF, Mc2, and μ3 values were obtained as the ratio between the standard deviation and the mean.
2.5 Statistical analysis
Two-way repeated measures analysis of variance (ANOVA) with Student-Newman-Keuls (SNK) post-hoc test for pair-wise comparisons was applied for MMG absolute and normalised RMS, MNF, Mc2, and μ3 values. The factors were contraction time (time) and transducer type (microphone and accelerometer). P<0.05 was considered significant. Data are presented as mean and standard error (SE) of the mean.
3 Results
All subjects were able to maintain the required force level for 3 min. At the end of the contraction, the mean rating of perceived exertion was 6.4±0.3 cm.
3.1 Comparison of MMGMIC and MMGACC descriptors
For normalised values, contraction time had a significant effect on RMS, MNF, Mc2, and μ3 values of both MMGMIC and MMGACC signals (respectively, F 17,13=5.27 P<0.001, F 17,13=2.84 P<0.001, F 17,13=7.99 P<0.001, and F 17,13=2.08 P<0.001; Figs. 2, 3). Normalised μ3 values were lower for MMGMIC (125.7±15.4%) than for MMGACC (173.8±15.4%) signals (F1,13=4.86, P<0.05).

Mean (±SE) absolute root mean square (RMS), mean power frequency (MNF), second-order central moment (Mc2) and third-order central moment (μ3) values of MMGMIC and MMGACC signals during sustained isometric contraction at 30% maximum voluntary contraction (n=14)

Mean (±SE) normalised root mean square (RMS), mean power frequency (MNF), second-order central moment (Mc2) and third-order central moment (μ3) values of MMGMIC and MMGACC signals during sustained isometric contraction at 30% maximum voluntary contraction (n=14)
There was a significant positive correlation (R 2=0.37, P<0.001) between RMS slopes estimated from MMGMIC and MMGACC signals. However, MNF (R 2=0.02), Mc2 (R 2=0.19), and μ3 (R 2=0.02) slopes estimated from the two sensors were not correlated.
3.2 Variability of estimates of MMG descriptors
The coefficient of variation of RMS values was significantly higher for MMGMIC than for MMGACC (0.249±0.007 vs. 0.220±0.007, respectively; P<0.05, Fig. 4 and Table 1). The coefficient of variation of μ3 values was significantly lower for MMGMIC compared with MMGACC (0.427±0.021 vs. 0.521±0.021; P<0.05, Table 1).

Mean (±SE) coefficient of variation of root mean square (RMS), mean power frequency (MNF), second-order central moment (Mc2) and third-order central moment (μ3) of MMGMIC and MMGACC signals during sustained isometric contraction at 30% maximum voluntary contraction (n=14)
4 Discussion
Higher order spectral moments of the MMG signal change over time, indicating a complex variation of the shape of the power spectrum with sustained contraction at 30% MVC. Moreover, despite similar trends of the time- and frequency-domain signal descriptors, the rates of change of spectral variables computed from signals of the two sensors were not correlated. There were also differences in the coefficient of variation of the estimates of RMS and third-order spectral moments obtained with the two transducers.
4.1 Changes in MMG signal properties during sustained contraction
During sustained contractions, the increase in the time-domain and the decrease in the frequency-domain descriptors of the MMG signal are usually attributed to changes in the number and discharge rate of the active motor units as well as to modifications in contractile fibre properties [15, 16]. The relative changes in time and frequency domains are function of the contraction level [6, 10, 15]. The anatomy and muscle fibre distribution also have an effect on the MMG frequency content [25]. Moreover, variations in the muscle intrinsic properties to some extent influence the MMG signal [15]. The changes in both absolute and normalised RMS and MNF values in the present study are similar to those reported in previous studies at similar contraction levels [9, 10, 15].
The second- and third-order central moments of the power spectral density provide information on the width and skewness of the MMG signal spectrum, describing more precisely slow non-stationarities [14]. The decrease in absolute and normalised MNF confirmed that the power spectral density of the MMG signal progressively compressed over time. However, the spectral bandwidth, that is, variance, increased with contraction time highlighting a variation in spectral shape during sustained contraction (Figs. 2, 3). The observed changes in spectral shape of the MMG signal are probably due to recruitment of additional motor units and changes in motor unit discharge rate with fatigue [2, 4, 11]. The effect of these phenomena on the MMG signal properties is difficult to predict due to the non-linear summation of the motor unit contributions [18]. Due to the significant changes in second- and third-order spectral moments observed in this study, it can be concluded that the first-order spectral moment is not sufficient to fully describe the changes in the MMG power spectrum.
4.2 Influence of the transducer type on MMG properties
The physical characteristics of the two transducers analysed differ largely. For condenser microphone, the frequency response declines with decreasing diameter and length of the air chamber. Therefore, it is suggested that air chamber should be at least 10 mm in diameter and 15 mm in length [21]. The microphone used in the present study might therefore not reproduce linear frequency components below 5 Hz. Microphones introduce a rigid mechanical discontinuity on the muscle surface that should be taken into consideration [16]. However, recent results indicate that the specific deformity of skin surface (microphone recordings) is less important than MMG amplitude changes [21].
The weight of the accelerometer used to record MMG signal was below the suggested limit of 5 g for accurate measurement [22]. Furthermore, contrary to other types of sensors, accelerometers record MMG signal in physical units (m s−2) enabling a comparison between different studies [15]. Microphones are probably more reliable than accelerometers to record MMG signal during anisometric contractions [8] while microphones require silent environment.
Despite similar general trends with respect to the development of localised muscle fatigue (Figs. 2, 3), important differences in the MMGMIC and MMGACC signals were observed (Fig. 1). The increase in bandwidth was more marked in MMGMIC recordings (Figs. 2, 3) and the normalised third-order spectral moments were significantly smaller for the microphone compared with accelerometer. Moreover, a lack of correlation was found between the rates of change of all spectral moments for MMGMIC and MMGACC recordings. This most likely cannot be explained by the different location of the two transducers since it has been previously observed that for distances up to 44 mm the location of the transducer does not significantly affect amplitude and spectral MMG features in the biceps brachii muscle [3]. Thus, the observed differences are attributed to different characteristics between the two transducers. During voluntary contractions, the frequency response of the MMGMIC might be affected by skin deformation due to the fact that the microphone is attached to the skin and by skin folds thickness [7].
Accelerometers have been indicated as the most reliable tool for MMG recordings during isometric contractions together with laser distance sensor [16]. Accordingly, in the present study we observed a lower coefficient of variation of RMS when measured from MMGACC than from MMGMIC. On the other hand, the coefficient of variation of normalised third-order spectral moments, not investigated in previous studies, was larger for MMGACC than for MMGMIC signals even though this can partly be explained by the relative low repeatability of skewness [12]. The present results obtained during isometric sustained contraction, confirm that the information contained in microphone- and accelerometer-based MMG signal is different [21], making comparison between studies difficult.
5 Conclusions
Changes in the power spectrum of MMG signals cannot be described exclusively with the first-order spectral moments. Moreover, the temporal and spectral descriptors of MMG signals and their changes over time due to sustained contraction are different when using a microphone or an accelerometer. Thus, comparison of studies that apply the two transducers may be critical.
References
Barry DT (1987) Acoustic signals from frog skeletal muscle. Biophys J 51(5):769–773
Bigland-Ritchie B, Furbush F, Woods JJ (1986) Fatigue of intermittent submaximal voluntary contractions central and peripheral factors. J Appl Physiol 61(2):421–429
Cescon C, Farina D, Gobbo M, Merletti R, Orizio C (2004) Effect of accelerometer location on mechanomyogram variables during voluntary, constant-force contractions in three human muscles. Med Biol Eng Comput 42:121–127
De Luca CJ (1984) Myoelectrical manifestations of localized muscle fatigue in humans. Crit Rev Biomed Eng 11:251–279
Frangioni JV, Kwan-Gett TS, Dobrunz LE, McMahon TA (1987) The mechanism of low-frequency sound production in muscle. Biophys J 51(5):775–783
Itoh Y, Akataki K, Mita K, Watakabe M, Itoh K (2004) Time-frequency analysis of mechanomyogram during sustained contractions with muscle fatigue. Syst Comput Japan 35(1):26–36
Jaskólska A, Brzenczek W, Kisiel-Sajewicz K, Kawczyński A, Marusiak J, Jaskólski A (2004) The effect of skinfolds on frequency domain of mechanomyogram depends on muscle force, age and gender. J Electromyogr Kinesiol 14:217–225
Madeleine P, Bajaj P, Søgaard K, Arendt-Nielsen L (2001) Mechanomyography and electromyography force relationships during concentric, isometric and eccentric contractions. J Electromyogr Kinesiol 11:113–121
Madeleine P, Farina D, Merletti R, Arendt-Nielsen L (2002a) Upper trapezius muscle mechanomyographic and electromyographic activity in humans during low force fatiguing and non-fatiguing contractions. Eur J Appl Physiol 87(4–5):327–336
Madeleine P, Jorgensen LV, Sogaard K, Arendt-Nielsen L, Sjogaard G (2002b) Development of muscle fatigue as assessed by electromyography and mechanomyography during continuous and intermittent low-force contractions effects of the feedback mode. Eur J Appl Physiol 87(1):28–37
Maton B, Gamet D (1989) The fatigability of two agonistic muscles in human isometric voluntary submaximal contraction: an EMG study II Motor unit firing rate and recruitment. Eur J Appl Physiol Occup Physiol 58(4):369–374
Merletti R, Castagno F, Prato G, Saracco C, Pisani R (1985) Prorieta’ e ripetibilita’ di misura di parametri spetralli del segnale EMG cutaneo in soggeti normali. Rassegna di Bioingegneria 10(2–3):83–96
Merletti R, Knaflitz M, De Luca CJ (1990) Myoelectric manifestations of fatigue in voluntary and electrically elicited contractions. J Appl Physiol 69:1810–1820
Merletti R, Gulisashvili A, Loconte LR (1995) Estimation of shape characteristics of surface muscle signal spectra from time-domain data. IEEE Trans Biomed Eng 42(8):769–776
Orizio C (1993) Muscle sound: bases for the introduction of a mechanomyographic signal in muscle studies. Crit Rev Biomed Eng 21(3):201–243
Orizio C (2004) Surface mechanomyogram. In: Merletti R, Parker P (eds) Electromyography, physiology, engineeringand noninvasive applications. 21st edn. IEEE Press John Wiley & Sons, Hoboken, pp 305–322
Orizio C, Solomonow M, Baratta R, Veicsteinas A (1993) Influence of motor unit recruitment and firing rate on soundmyogram and EMG characterirics in cat gastrocnemius. J Electromyograph Kinesiol 2(4):232
Orizio C, Liberati D, Locatelli C, De Grandis D, Veicsteinas A (1996) Surface mechanomyogram reflects muscle fibres twitches summation. J Biomech 29:475–481
Orizio C, Baratta RV, Zhou BH, Solomonow M, Veicsteinas A (1999) Force and surface mechanomyogram relationship in cat gastrocnemius. J Electromyogr Kinesiol 9(2):131–140
Sogaard K, Blangsted AK, Jorgensen LV, Madeleine P Sjogaard G (2003) Evidence of long term muscle fatigue following prolonged intermittent contractions based on mechano- and electromyograms. J Electromyogr Kinesiol 13(5):441–450
Watakabe M, Mita K, Akataki K, Itoh Y (2001) Mechanical behaviour of condenser microphone in mechanomyography. Med Biol Eng Comput 39(2):195–201
Watakabe M, Mita K, Akataki K, Ito K (2003) Reliability of the mechanomyogram detected with an accelerometer during voluntary contractions. Med Biol Eng Comput 41(2):198–202
Welch PD (1967) Use of fast Fourier Transform for estimation of power spectra - A method based on time averaging over short modified periodograms. IEEE Trans Audio Electroacoust 15(2):70–73
West W, Hicks A, Clements L, Dowling J (1995) The relationship between voluntary electromyogram, endurance time and intensity of effort in isometric handgrip exercise. Eur J Appl Physiol 71(4):301–305
Yoshitake Y, Moritani T (1999) The muscle sound properties of different muscle fiber types during voluntary and electrically induced contractions. J Electromyogr Kinesiol 9(3):209–217
Acknowledgements
This work was supported by The Danish National Research Foundation and the Danish Centre for International Cooperation and Mobility in Education and Training.
Author information
Authors and Affiliations
Corresponding author
Additional information
Submitted to: Medical and Biological Engineering and Computing
Rights and permissions
About this article
Cite this article
Madeleine, P., Ge, Hy., Jaskólska, A. et al. Spectral moments of mechanomyographic signals recorded with accelerometer and microphone during sustained fatiguing contractions. Med Bio Eng Comput 44, 290–297 (2006). https://doi.org/10.1007/s11517-006-0036-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-006-0036-2