
Abstract
It is frequently hypothesized that feelings of social isolation are detrimental for an individual’s mental health, however standard statistical models cannot estimate this effect due to reverse causality between the independent and dependent variables. In this paper we present endogeneity-corrected estimates of the mental health consequences of isolation (based on self-assessed loneliness scores) using Australian panel data. The central identification strategy comes from a natural source of variation where some people within our sample are required by work or study commitments to move home. This relocation may break individuals’ social ties, resulting in significantly higher reported feelings of loneliness and consequently may lower mental health scores. The method gives results that are significant, robust and pass a battery of diagnostic tests. Estimates indicate that feelings of isolation have large negative consequences for psychological well-being, and that the effects are larger for women and older people. The results suggest that at current levels, a 10 % reduction applied to all individuals would reduce annual expenditure on mental illness in Australia by approximately $3B AUD, or around $150 AUD per person.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is a broad scientific consensus that strong interpersonal relationships are good for a person’s mental health and well-being (Almedom and Glandon 2007; Bassett and Moore 2013; De Silva et al. 2005). Sociological and psychological literature has argued, for example, that social ties can provide a buffer against stress or anxiety (Bolger and Eckenrode 1991; Cohen and Wills 1985; Schwarzer et al. 2013), bolster self-esteem (Cobb 1976; Hoffman et al. 1988) and inhibit mental illnesses such as schizophrenia (Boydell et al. 2002; Kirkbride et al. 2008) and depression (Tomita and Burns 2013). Similarly, associations have been found between geographic regions with low social capital (implying a lack of social connectedness within a community) and various adverse behavioral tendencies including suicide (Helliwell 2003), alcohol abuse (Weitzman and Kawachi 2000) and crime (Buonanno et al. 2009; Kennedy et al. 1998).
A well-recognized difficulty with these lines of research however, is that an individual’s mental health is also likely to affect their social interactions. For example persons with low mental health scores are less likely to marry or cohabitate (Murstein 1967; Pevalin and Ermisch 2004), tend to withdraw from labor markets (Ettner et al. 1997; Frijters et al. 2010) and be disproportionately shy (Heiser et al. 2003). Consequently, feelings of social isolation are plausibly both a symptom and a cause of poor mental health. For this reason, regular statistical estimates of the relationship between these variables are likely to be biased, as any observed correlation implicitly conflates these two opposing but mutually reinforcing effects.
The goal of this paper is to disentangle these factors and estimate the causal effect of feelings of social isolation (i.e., self-assessed loneliness) on mental health. Using individual-level data from the Australian HILDA (Household Income and Labour Dynamics in Australia) survey, we follow a similar path to a newly emergent economic and public health literature that tackles this problem with the use of Instrumental Variable (IV) estimators (D’Hombres et al. 2010; Fiorillo and Sabatini 2011; Folland 2007; Kim et al. 2011; Ronconi et al. 2010). However as these works have focused on general or physical outcomes rather than mental health, there is a need to extend econometric research to cover this specific health concept.
Distinguishing between correlation and causation presents a challenge, which the above strand of literature tackles by determining sources of variation that affect an individual’s social ties, without directly influencing their health status (Durlauf and Fafchamps 2005; Folland 2007). These papers have employed ecological (i.e., geographic) instruments based on factors such as religiosity (D’Hombres et al. 2010; Folland 2007; Kim et al. 2011), variations in income inequality and education (D’Hombres et al. 2010), corruption and population density (Kim et al. 2011), and localized averages of the number of daily conversations and interest in politics (Fiorillo and Sabatini 2011). However as with all such studies (including ours) the results depend upon the assumption that the instruments are truly exogenous. Since there is no way to empirically verify this assumption (Deaton 2010; Parente and Silva 2012) the validity of the findings rests on the plausibility of the identification strategy.
Rather than using group-level instruments, our central identification strategy acts at the individual level and involves following individuals who have been pressured by external circumstances to move house within the last year. The intuition is that being required to move provides appropriate identifying variation if it is determined by either (i) work or study requirements or (ii) changing rental availability. As these factors are not initiated by the individual (and are not easily resisted) they are plausibly exogenous determinants of social contact. Relocation causes individuals to have their social ties temporarily diminish, as neighbors, friends and family that could once offer companionship will become less available (Cattan 2009). By focusing only on the deterioration of social interactions due to enforced geographic remoteness, the response of our mental health indices can be estimated without having to worry about reverse causality biasing the results.
In addition to estimating this effect, we test the strength of our findings by performing various diagnostic tests upon the models. Since econometric estimates are often sensitive to certain implicit assumptions, it has become customary to explore the influence of such assumptions upon the final results. We test the coherency of our identification approach by generating (in our own data) some of the same instruments employed in related works on social capital and health (D’Hombres et al. 2010; Fiorillo and Sabatini 2011; Kim et al. 2011). If results are found to be consistent between our individual-level instrument and the ecological approaches used in these papers, this would have desirable implications for both methods, as it is well known that all appropriate instruments should identify the same causal effect. Once this has been carried out, a further robustness check is provided by ensuring that the findings are not unduly influenced by the choice of control variables. Numerous authors have noted that estimates from regression models are often sensitive to this choice (e.g., Leamer 1983; White and Lu 2010), and hence it is possible for researchers to produce results that are misleading by including only very specific sets of covariates in their models. By systematically altering our control variables we can determine whether the results are highly model-dependent (and thus lack robustness) or if they hold over a wide range of specifications.
After performing these diagnostics, we apply our models to address two issues related to mental health policy. Firstly, a debate remains in the literature whether a subjective sense of social integration merely aids health in times of stress or anxiety (the buffering effect) or if it is beneficial for all individuals (the direct effect) regardless of stress levels (Cohen and Wills 1985). By searching for unspecified structural breaks in our regressions we can test for the possibility of differing effects of social isolation across the mental health distribution, and also locate the points at which any such change occurs. The same method can be used to test for structural differences in age and education levels, while related methods can be used to distinguish between the estimated effects between men and women. This approach allows us to identify segments of society for whom the consequences of isolation are likely to be the most severe.
Finally, we also provide a policy interpretation for our results by estimating the sensitivity of expenditure on mental health problems to marginal changes in isolation. By considering a counterfactual scenario where each individual within our data receives a small improvement in their social situation, we can simulate the effect of such an improvement on total expenditure. Our results suggest that expenditure on mental health could be curtailed significantly if feelings of social isolation could be reduced.
Data
Data are taken from the Australian HILDA survey which is an approximately nationally representative sample that has followed around 20,000 individuals since 2001. The data set is frequently used for health economics research and forms the Australian analogue of the US Panel Study of Income Dynamics (PSID), the British Household Panel Survey (BHPS) and the German Socioeconomic Panel (SOEP). Although our data are limited to only one developed country, it is argued that the relationship between social experiences and mental health is of fundamental importance to all humans. Therefore results are unlikely to be highly country specific and should be informative in a broad range of circumstances.
For our main measure of mental well-being we use Kessler psychological distress (K10) scores (Kessler, et al. 2002), which are an extensively validated and widely employed health assessment tool (Donker et al. 2010). The K10 index is an aggregation of 10 questions on respondent anxiety and depressive symptoms experienced in the 4 weeks prior to undertaking the survey. Each question is scored on a five point scale such that the total ranges between 10 and 50 where higher scores indicate greater levels of distress. The HILDA data records K10 data in three waves (2007, 2009 and 2011) and hence these are the years employed for the analysis. We also employ the SF36 mental health as a secondary measure. Like the K10 this is a highly validated multi-item scale (Bowling 1997; Jenkinson et al. 1993), where responses are aggregated to give an overall score (Ware et al. 2000). In the case of the SF36, scores range between 0 and 100 where higher values imply greater mental well-being, and hence the measure has the reverse interpretation of the K10. Although this variable appears in more waves than the K10, to retain consistency across variables we only use observations from the three aforementioned years.
To measure perceived isolation we take individual level observations on subjective social satisfaction. The question asks each respondent to rate how much they agree or disagree with the statement “I sometimes feel very lonely” on a seven point scale where higher values indicate a greater level of agreement. We are thus concerned with subjective feelings of isolation rather than objective measures of social distance. This subjective approach is desirable in that it will implicitly capture idiosyncratic factors such as differences in desired levels of interpersonal contact, and hence will better represent the most harmful elements of social isolation. Thus we are effectively employing a cognitive concept of social capital, as opposed to a structural concept which measures behavior (Bain and Hicks 1998; Harpham et al. 2002).
For instruments, we identify individuals who have been forced to relocate during the last year due to (i) work requirements, (ii) study commitments, or (iii) the property they are renting becoming unavailable. All three variables are in binary form and are aggregated to form a single dummy variable. There are a number of other indicators for different reasons for moving (e.g., to follow a partner or start a business) however as they represent decisions initiated by the individual they are potentially endogenous and are therefore excluded from the analysis. It is noted that the validity of this instrument is dependent upon the assumption that mental strain from moving dissipates quickly after successfully relocating. Several authors have noted that the process of moving home can be stressful (Raviv et al. 1990), however as our data identifies individuals who have already occupied their new premises for up to a year, it is argued that any remnant stress will have subsided by the time the survey is completed. To be exogenous our method also requires that individuals either (i) are unable to resist pressure to relocate, or (ii) if they do, this is unrelated to their future mental health. While it is possible that individuals with better mental health may respond differently to pressure to relocate, it is assumed that the effect is small enough not to bias estimates.
Finally a number of auxiliary variables are taken to generate alternative instruments and to control for extraneous determinants of mental health. Data on incomes, education, age, sex, physical health, household size, geographic area, marital status and employment status are used, alongside life-event variables that indicate a major change within the last year. These include becoming married, separating from one’s spouse, births, death of a spouse or child, death of a relative or friend, losing one’s job, retiring, and being a victim of violence. This represents a large set of variables that can account for most of the typical social determinants of anxiety or depression (Mirowsky and Ross 2003).
Modeling Social Isolation and Mental Health
Given the hypothesized association between perceptions of social isolation and diminished mental health status, we begin by depicting their relationships below. Longitudinal averages of the mental health indices and loneliness scores are taken for each individual, and we apply kernel regressions to extract the underlying dependencies. Both sets of estimates are presented alongside 99 % confidence intervals based upon bootstrap standard errors. The left panel of Fig. 1 shows the anticipated result that individuals who felt lonelier had considerably higher levels of psychological distress according to the K10 index; while the right panel shows that these individuals also exhibit lower scores on the SF-36 MCS. The slopes of the depicted lines indicate that a one unit increase in loneliness coincides with an increase of around four K10 units, while for the SF-36 this is about 7 units. These estimates imply linearity in both relationships, which appears to be approximately correct, although there is some sign of a slight increase in sensitivity occurring beyond a loneliness score of six. However the increased confidence intervals around these endpoints suggest that sampling variation may be a partial explanation.

Subjective loneliness scores and mental health - K10 and SF36 MCS. Note: The left panel shows the association between loneliness and the K10 Psychological Distress score while the right panel gives the association for the SF-36 Mental Health Index
The results depicted in Fig. 1 only show binary associations rather than causal relationships. In order to identify causality, a fixed-effects estimator would be the most appropriate econometric model due to its ability to remove time-invariant heterogeneity, however owing to limited within-individual variation the method is insufficient to obtain meaningful results. Instead the waves are pooled and differences over time are accounted for with annual dummies. A two-stage least squares estimator is then employed where the endogenous right-hand variable is first regressed against the exogenous control variables and the instruments, and the fitted values are then inserted into the structural equations. The structural equation is
where MH denotes the mental health measure, L is the loneliness score, and ϕ captures the effect on mental health. Further α w refers to annual intercept terms and α 1 … α j are coefficients on the control variables x 1 … x j . The reduced form equation is
where the β terms have the same interpretations as the α terms in Eq. (1) and γ is the coefficient on instrument z.
The estimates for both the first stage regression and the 2 s stage regressions (for the two mental health indices) are given in Table 1. Standard errors that account for (i) increased uncertainty due to the two-stage estimation procedure, (ii) clustering by individual, and (iii) heteroskedasticity are employed. Further pseudo R 2 terms are provided based upon the squared correlation between the actual and predicted values, while Kleibergen and Paap (2006) and Cragg and Donald (1993) F statistics for underidentification and weak identification are also given.
Examining the first stage regression in column 1, we observe that feelings of isolation are well predicted, with the model explaining around 69 % of the variation in scores. Most importantly, the instrument of home relocation in row 1 is significant and of the expected sign, implying that individuals that have recently moved are more lonely. Furthermore the control variables are generally in line with expectations. Older persons and those experiencing notable life events (pregnancies, births, separations from spouse, changing jobs, retiring, deaths of family members or relatives) felt more isolated, while individuals who were married, had high incomes, high education levels and lived in larger households had significantly lower scores.
Estimates of the second stage regressions are given in columns 2 and 3. Both models explain about 50 % of the variation in mental health, while the Kleibergen-Paap statistics reject the null of underidentification (p = .0245) implicit in both models. However weak identification tests show that the instrument is not particularly strong, with the Cragg-Donald F statistic falling below 10. Thus the approach may not be strong enough to remove all the potential bias, although we revisit this issue in the next section and show that the results are consistent with more strongly identified approaches.
The key coefficients are listed in row 5, which give the effect of the loneliness scores after instrumentation. When the K10 is used as the mental health variable we see that over the seven point scale, a single unit increase in an individual’s loneliness results in an increase in their psychological distress score of around 4.78 units. This is significant at 5 % and indicates that loneliness acts causally to increase distress. Turning to the second stage regression for the SF-36 the parameter estimate of −6.13 indicates that increased isolation lowers the mental health score by this amount. This also implies an adverse effect on mental health (due to the reverse interpretation of the SF-36 relative to the K10), although the result is only significant at 10 %.
Instrumentation Tests and Robustness
The results presented in Table 1 rely upon the assumption that being forced to relocate is truly exogenous, and that its association with feelings of isolation is sufficiently strong to identify our parameters. If either of these is untrue, then the effect of loneliness we estimate will still suffer from endogeneity bias and thus cannot be interpreted as a true causal impact. While there is no way to explicitly test this hypothesis, an alternative is to test for consistency across differing identification strategies. The intuition is that all suitable instruments should yield similar estimates, and thus if alternative approaches give the same result, this suggests the identifying variables are either sound, or all create the same form of bias. As Parente and Silva (2012) emphasize it is desirable to employ a variety of conceptually different instruments such that the likelihood of a mutual bias is minimized.
To perform this test we combine our approach with some of the identification strategies employed in earlier works on social capital and health. We take three ecological level indicators corresponding to those employed by D’Hombres et al. (2010), Fiorillo and Sabatini (2011) and Kim et al. (2011). The first alternative instrument we use is based upon geographic averages of the dependent variable; the second is the degree of local income inequality (measured by the coefficient of variation of household incomes) and the third is a measure of religious fractionalization (the entropy of the population shares of various religious groups). Each of these instruments is evaluated for all Australia’s states and territories, giving eight alternative values. The idea behind these instruments is that social capital varies substantially from place to place (Wilkinson and Pickett 2009) and hence be more or less conducive to promoting social relationships. Given that a person’s state of residence is largely determined by factors beyond that person’s control (such as where they were born, where their family lives, or job availability) geographic factors may then exogenously drive the social states of individuals. We will refer to the enforced relocation variable as instrument I and thus regional averaged loneliness scores, income inequality and religious fractionalization will be labeled instruments II, III and IV respectively.
Once these alternative instruments are established, we re-estimate the regression models given in Eqs. (1) and (2), but now also include the extra identifying variables. Table 2 reports the new parameter estimates alongside results of the Hansen (1982) test (second and third columns for each mental health variable) and the Cragg-Donald F test for weak identification (fourth column). Row 1 gives estimates based upon all four instruments, while rows 2 and 3 give other relevant estimations based upon restricted sets of identifiers.
Parameter estimates from Table 2 reinforce the previous finding of significant effects of the appropriate signs and magnitudes, however the central finding is concerned with the test statistics and p-values given in the central two columns. Examining the p-values for the Hansen test in first row, it is evident that for both the K10 and SF-36 we are unable to reject the null hypothesis and hence find no evidence of inconsistency in parameter estimates across the four alternative methods. This result is attractive in several respects. Firstly, the consistency found between the individual-level approach and the ecological methods employed elsewhere adds considerable robustness to our results, as the two identification strategies are entirely unrelated. Secondly, as both sets of instruments appear exogenous (at least within our data), this suggests that they may well be exogenous with respect to other health variables and for other data sets as well. This in turn reinforces the validity of the findings reported by other authors who use these approaches.
The second and third rows of Table 2 show similar results to the first row. When the instrument set is restricted to enforced relocation and averaged loneliness scores (row 2), there is still little sign of inconsistency across estimates (p = 0.114 and p = 0.887 for the K10 and SF-36) although the results for the K10 are marginal. Attractively however these regressions were the most strongly identified, with the Cragg-Donald F statistics for underidentification easily exceeding the standard threshold of 10. This is in contrast to results reported elsewhere which show Cragg-Donald F statistics ranging from 5 to 9, suggesting that weak identification may be a minor issue for other models. Turning to row 3, we see that when the alternative set of regional income inequality and religious fractionalization are used, the coefficient magnitudes are still relatively similar. Again the Hansen test fails to find inconsistency between these approaches over the two mental health measures (p = 0.835 and p = 0.764) although there is again some sign of weak identification for these models.
Given the slight differences in parameter estimates from Tables 1 and 2 we consider which set of instruments offers the best performance. This may be determined by using the approach outlined by Breusch et al. (1999) which tests each instrument separately to determine if it is significantly contributing to the model. In our case, instruments III and IV (religious fractionalization and household annual income inequality) were redundant in the presence of our other identifying variables and thus can be omitted to retain efficiency, implying that the best results are obtained with instruments I and II combined. However we note that instruments III and IV were not redundant when the enforced relocation variable and geographic loneliness averages were excluded.
Robustness of Results
A further assumption implicit within these results is that the chosen set of covariates control appropriately for extraneous determinants of mental health. However it is often the case that estimates are sensitive to this choice of control variables, and hence seemingly innocuous assumptions concerning model specification can strongly influence findings. To examine the robustness of our results, we re-estimate our equations using various alternative configurations of controls (Barslund et al. 2007; White and Lu 2010). We choose five typical control variables (income, geographic remoteness, number of household members, gender and marital status) and systematically omit all combinations, giving 32 alternative results. If these alternative estimates cluster around the values already presented we can conclude that the results are robust, while a great variation in coefficient size (particularly if there are frequent changes in sign) would reduce their persuasiveness.
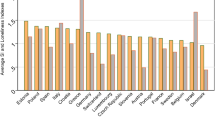
To illustrate the clustering of parameter values we treat these alternative coefficients as if they were random draws and estimate their densities using adaptive Gaussian kernels. These are depicted in Fig. 2 for both the K10 and SF-36.

Coefficient magnitudes - relative frequencies. Note: The left panel shows the clustering of parameter estimates when the K10 is the dependent variable, while the right panel does the same for the SF-36. All estimates are obtained using adaptive Gaussian kernels. I, II, III and IV refer to instruments based on relocation, geographically averaged loneliness, income inequality and religious fractionalization respectively
The left panel shows the clustering of coefficients for the effect of loneliness on the K10, while the right panel does so for the SF-36. Results from the left panel indicate that when instrument I is used, the effect size ranged between 3.5 and 5 K10 units per unit change, while instruments III and IV gave slightly smaller estimates ranging from about 0.5 to 2.5. The majority of estimates however clustered between 2 and 3 for both when I and II are used, and when the full set of four instruments is employed. In no instances did the coefficient change size, and thus we can conclude that the sign is highly robust. For the SF-36 depicted in the right panel there is more consistency across the models, but a greater degree of variation in effect sizes for differing sets of controls. Estimates were mostly clustered between −8 and −3 SF-36 MCS units, and again there were no cases of parameters changing signs.
Structural Break Testing
Having verified that loneliness does act causally to impair mental health, and that the results are largely insensitive to both the choice of instruments and the specific set of controls, we now use the models to address two important questions related to mental health policy. One point of particular relevance is that the consequences of feelings of isolation are unlikely to be uniform across all Australians, and hence there is some interest in identifying segments of the population for which the effect may be particularly strong. For example the buffering effect hypothesizes a non-linearity in effect size, where a lack of social support is particularly damaging for individuals already experiencing high levels of stress. Conversely the direct effect hypothesizes that isolation is damaging for all persons regardless of their mental condition (Cohen and Wills 1985). It is also possible that nonlinearities exist for other variables as well, such as for men and women, and over differing ages and education levels.
To test for these potential differences we employ the preferred model from the previous section (employing instruments I and II) and use the Quandt-Andrews (Andrews 1993) method to test for structural breaks. This allows for a single change in the effect of isolation to occur, but considers every observation point as a potential location for this point of change. Results are reported in Table 3, alongside coefficient estimates evaluated at each side of the structural break.
Estimates presented in the first two rows show that significant structural breaks exist in all regressions, implying that the effect of isolation is not stable over our chosen variables of interest. Over the distributions of the K10 and SF-36 there are significant structural breaks at points 20 and 72 respectively. In persons with K10 psychological distress scores already exceeding 20, the effect is estimated at 4.03 per unit (on the seven point scale), while those with lower distress have the lesser impact of 0.813 per unit. This suggests that individuals who are already highly distressed are much more sensitive to increased loneliness than those who are not. Nonetheless the coefficient size for individuals with a score less than 20 on the K10 is still positive, albeit relatively small when compared to highly distressed persons. Similarly for the SF-36 the estimated effect of −6.07 applies to persons with relatively poor mental health scores (i.e., below 72) while healthier individuals have the lesser effect size of −3.47. Thus both sets of results imply that the effect of a subjective sense of isolation is much greater for those with already poor mental health states. This non-linearity lends support to the buffering hypothesis, although the effect size is still of the expected sign for those with better health scores.
Turning to the other estimates we see that for both health variables, there is a structural break over the distribution of age, where older individuals are more sensitive. The remarkable feature of this result is that the breaks both occur at the age of 64, which is very close to the average retirement age in Australia, of 64.9 for men and 62.9 for women (OECD 2012). Such a result may plausibly be due to a changing in life goals that coincides with leaving the labor force (e.g., Freedman 1999), where social factors become more important as paid employment finishes. This result is of further importance as it is likely that retirement and subsequent old age are periods of life when some individuals experience intense feelings of isolation. For example persons beyond 65 will typically lose contact with colleagues, are more likely to have their mobility constrained (and hence be less able to undertake social activities) and are at greater risk of bereavement through losses of friends, relatives and partners.
Surprisingly, more highly educated people were found to have a greater sensitivity to feelings of isolation. Both mental health measures are more sensitive to loneliness for individuals with over 11 years of formal education, although for the SF-36 this differential in effect size is small. Lastly, women are also more affected than men, however the coefficients were in some cases of unrealistic magnitudes. Such a result is similar to the general health effects of social capital and general health reported by Kim and Kawachi (2006, 2007). There are a number of potential explanations for this phenomenon, including asymmetries in the self-reporting of feelings of isolation (Borys and Perlman 1985) or differences in social needs across the sexes (Eagly 1987).
The Marginal Economic Benefit of Decreased Isolation
The second policy issue we consider is the economic benefit that may be obtained through policies that mitigate social isolation in Australians. To evaluate these economic benefits, we conduct some simulations employing (i) our parameter estimates, and (ii) recent aggregates of expenditure supporting individuals with mental illness in Australia. Our approach involves attributing the sum of expenditures to individuals that may be considered to be suffering from mental disorders, and simulating the relative improvement in health of these individuals that would occur if they were to benefit from a small decrease in feelings of isolation. The reduction in expenditure is then taken as proportional to the improvement in mental health that would occur for these persons.
We begin with total expenditure on support for individuals with mental illnesses, which was estimated at $28.6B AUD in 2012 (Medibank 2013). This figure includes direct spending on items such as public and private mental health services, medication, and related drug and alcohol services. Some non-health expenditure on items such as homelessness, legal fees, education, training and income support is also included.
Once the monetary costs have been established, individuals who suffer from psychological disorders are identified using the discrete classifications for K10 scores, whereby persons with scores of 20 or greater are regarded as likely candidates (Andrews and Slade 2001). By summing the excesses of K10 scores over this threshold we can obtain an equivalency between the aggregate of psychological disorders in our sample, and the mental health expenditures that would accrue to these individuals. Assuming linearity and continuity, the effect of a 10 % decrease in loneliness (relative to the sample average) is then simulated by multiplying this magnitude by the estimated effect sizes in Tables 1 and 2. The relative decrease in excess K10 scores is then applied to the aggregate expenditure, giving the results in Table 4. We also repeat the exercise for the SF-36 MCS, where a threshold value of 60 is used for a mild mental disorder, a figure which corresponds to the same percentile as the benchmark of 20 advocated for the K10 index.
Results from Table 4 show that a 10 % decline in the loneliness scores of individuals would substantially reduce expenditure on mental health. While the estimated expenditure reductions range from around $2B to $5B when different models are used, there is a reasonable degree of congregation around values of approximately $3B, or about $150 per person per year. This figure also lies close to the median of the estimates, with four of the eight values above this point and the other four below. Attractively there is a high degree of consistency across the two mental health measures, and further combinations of instruments and control variables also yield similar results. The findings suggest that small decreases in feelings of isolation are likely to have large positive effects in reducing expenditure on mental health problems.
Conclusion
The principle finding we have outlined is that there is strong empirical evidence that social isolation acts to harm mental health. Much of the paper has been concerned with estimating this effect while disentangling reverse causality between the independent and dependent variables. This has been accomplished with the use of an instrumental variable that identifies individuals who have been forced to relocate from their homes. Enforced relocation was treated as a quasi-random event that separates some individuals from their neighbors, friends and family, and hence increases the subjective sense of isolation of these persons. The identification strategy is novel, and provided results that are consistent with other approaches in an emergent literature on correcting for endogeneity in studies of social capital and public health. The consistency of results across multiple approaches is particularly appealing as it suggests that the instrumental procedures are sound, since valid instruments should produce results that converge to the same value.
Once the basic statistical models were produced, a number of diagnostics were conducted and several applications were presented. Firstly we implemented a battery of robustness checks and showed that our results are quite insensitive to the specification of control variables. Consequently we conclude that the findings are unlikely to be dependent upon some arbitrary modeling assumptions, and hence are more likely to be indicative of the underlying mechanisms that determine an individual’s mental health status. Furthermore, once validated, the models were employed to identify population segments that are unusually sensitive to marginal changes in loneliness. Women, older persons and individuals with greater than 11 years of formal education were found to face a greater degree of sensitivity to feelings of isolation than the rest of the sample. Lastly the models were used to estimate the economic benefit that would occur if loneliness were to decline in Australia due to an across-the-board reduction of 10 % relative to the sample mean. We find that expenditure on mental illness would fall by around $3B AUD in this instance.
The findings have some important implications for policy. The high sensitivity of our mental health indices to perceptions of social isolation suggests that small improvements in the latter should have substantial consequences for the former. Such benefits would be magnified if policies were targeted towards aiding women and persons retiring from the workforce. Furthermore as improvements in mental health are likely to have positive flow-on effects such as greater physical health and improved general well-being, the sum of the desirable medical, social and economic consequences should be even larger again. Given that indicators of social capital such as membership in organizations and interpersonal trust have been mostly declining in Australia over the last few decades (Leigh 2003), our results indicate that implementing programs that may reverse this trend should be considered a priority for policy makers. Therefore ‘local area initiatives’ and other policies such as investments in community programs, increased flexibility in working hours, and relaxed regulations on public gatherings (Productivity Commission 2003) should be effective in combating mental health problems.
Lastly we wish to emphasize some of the caveats that underpin the work and to outline possible directions for future work. As virtually all instrumental variables used in this type of research (including our own) have the potential to be endogenous in one way or another, results presented here and elsewhere still depend on some assumptions that are hard to verify. These include standard assumptions about model specification as well as the more subtle assumptions on exclusion restrictions. Thus further research should be conducted into robustness, as well as on finding other novel identifying variables such that parameter estimates can be refined. Finally as panel data models such as Fixed Effects estimators provide additional scope for controlling for endogeneity, future research should look to reconcile findings from these models with others based on cross-sectional variations such as those presented here.
References
Almedom, A., & Glandon, D. (2007). Social capital and mental health: an updated interdisciplinary review of primary evidence. In I. Kawachi, S. Subramanian, & D. Kim (Eds.), Social capital and health (pp. 191–238). New York: Springer.
Andrews, D. (1993). Tests for parameter instability and structural change with unknown change point. Econometrica, 61, 821–856.
Andrews, G., & Slade, T. (2001). Interpreting scores on the Kessler psychological distress scale (K10). Australian and New Zealand Journal of Public Health, 25, 494–497.
Bain, K. & Hicks, N. (1998). Building social capital and reaching out to excluded groups: the challenge of partnerships. Paper presented at CELAM meeting on The Struggle against Poverty towards the Turn of the Millennium, Washington.
Barslund, M., Chiconela, J., Rand, J., & Tarp, F. (2007). Understanding victimization: the case of mozambique. World Development, 35, 1237–1358.
Bassett, E., & Moore, S. (2013). Mental health and social capital: Social capital as a promising initiative to improving the mental health of communities. In A. Rodriguez-Morales (Ed.), Current Topics in Public Health.
Bolger, N., & Eckenrode, J. (1991). Social relationships, personality, and anxiety during a major stressful event. Journal of Personality and Social Psychology, 61, 440–449.
Borys, S., & Perlman, D. (1985). Gender differences in loneliness. Personality and Social Psychology Bulletin, 11, 63–76.
Bowling, A. (1997). Measuring health: A review of quality of life measurement scales. London: Open University Press.
Boydell, J., McKenzie, K., & van Os, J. (2002). The social causes of schizophrenia: an investigation into the influence of social cohesion and social hostility. Schizophrenia Research, 53–264.
Breusch, T., Qian, H., Schmidt, P., & Wyhowski, D. (1999). Redundancy of moment conditions. Journal of Econometrics, 9, 89–111.
Buonanno, P., Montolio, D., & Vanin, P. (2009). Does social capital reduce crime? Journal of Law and Economics, 52, 145–170.
Cattan, M. (2009). Loneliness, interventions. In The encyclopedia of human relationships. London: Sage.
Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine, 38(5), 300–314.
Cohen, S., & Wills, T. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310–357.
Cragg, J., & Donald, S. (1993). Testing identfiability and specification in instrumental variables models. Econometric Theory, 9, 222–240.
D’Hombres, B., Rocco, L., Suhrcke, M., & McKee, M. (2010). Does social capital determine health? Evidence from eight transition countries. Health Economics, 19, 56–74.
De Silva, M., McKenzie, K., Harpham, T., & Huttly, S. (2005). Social capital and mental illness: a systematic review. Journal of Epidemiology and Community Health, 59, 619–627.
Deaton, A. (2010). Instruments, Randomization, and Learning about Development. Journal of Economic Literature, 48, 424–455.
Donker, T., Comijs, H., Cuijpers, P., Terluin, B., Nolen, W., Zitman, F., & Penninx, B. (2010). The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research, 176, 45–50.
Durlauf, S., & Fafchamps, M. (2005). Social capital. In S. Durlauf & P. Aghion (Eds.), Handbook of economic growth (pp. 1639–1699). Amsterdam: North Holland.
Eagly, A. (1987). Sex differences in social behavior: A social role interpretation. Hillsdale: N.H: Earlbaum.
Ettner, S., Frank, R., & Kessler, R. (1997). The impact of psychiatric disorders on labor market outcomes. Industrial and Labor Relations Review, 51, 64–81.
Fiorillo, D., & Sabatini, F. (2011). Structural social capital and health in Italy. The University of York: Health Economics and Data Group Working Paper 11/23.
Folland, S. (2007). Does “community social capital” contribute to population health? Social Science and Medicine, 64, 2342–2354.
Freedman, M. (1999). Prime time: How baby-boomers will revolutionize retirement and transform America. New York: Public Affairs.
Frijters, P., Johnston, D., & Shields, M. (2010). Mental health and labour market participation: Evidence from IV panel data models. IZA Discussion Papers 4883, Institute for the Study of Labor (IZA).
Hansen, L. (1982). Large sample properties of generalized method of moments estimators. Econometrica, 50(3), 1029–1054.
Harpham, T., Grant, E., & Thomas, E. (2002). Measuring social capital within health surveys: Key issues. Health Policy and Planning, 17, 106–111.
Heiser, N., Turner, S., & Beidel, D. (2003). Shyness: relationship to social phobia and other psychiatric disorders. Behaviour Research and Therapy, 41, 209–221.
Helliwell, J. (2003). Well-being and social capital: does suicide pose a puzzle? Social Indicators Research, 81, 455–496.
Hoffman, M., Ushpiz, V., & Levy-Shiff, R. (1988). Social support and self-esteem in adolescence. Journal of Youth and Adolescence, 17, 307–316.
Jenkinson, C., Coulter, A., & Wright, L. (1993). Short form 36 (SF-36) health survey questionnaire: normative data for adults of working age. British Medical Journal, 306, 1437–1440.
Kennedy, B., Kawachi, I., Prothrow-Stith, D., Lochner, K., & Gupta, V. (1998). Social capital, income inequality, and firearm violent crime. Social Science and Medicine, 47, 7–17.
Kessler, R., Andrews, G., & Colpe, L. (2002). Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32, 959–956.
Kim, D., & Kawachi, I. (2006). A multilevel analysis of key forms of community - and individual - level social capital as predictors of self - rated health in the United States. Journal of Urban Health, 83, 813–826.
Kim, D., & Kawachi, I. (2007). US state level social capital and health related quality of life: multilevel evidence of main, mediating, and modifying effects. Annals of Epidemiology, 17, 258–269.
Kim, D., Baum, C., Ganz, M., Subramanian, S., & Kawachi, I. (2011). The contextual effects of social capital on health: a cross-national instrumental variable analysis. Social Science and Medicine, 73, 1689–1697.
Kirkbride, J., Boydell, J., Ploubidis, G., Morgan, C., Dazzan, P., McKenzie, K., Murray, R., & Jones, P. (2008). Testing the association between the incidence of schizophrenia and social capital in an urban area. Psychological Medicine, 38, 1083–1094.
Kleibergen, F., & Paap, R. (2006). Generalized reduced rank tests using the singular value decomposition. Journal of Econometrics, 133, 97–126.
Leamer, E. (1983). Let’s take the Con Out of econometrics. American Economic Review, 73, 31–43.
Leigh, A. (2003). Trends in social capital”. In K. Christensen & D. Levinson (Eds.), Encyclopedia of community: From the village to the virtual world. Thousand Oaks: Sage.
Medibank Private (2013). The case for mental health reform in Australia: A review of expenditure and system design (Technical Report), Retrieved from http://www.medibank.com.au/Client/Documents/Pdfs/.
Mirowsky, J., & Ross, C. (2003). Social causes of psychological distress. New York: Aldine De Gruyter.
Murstein, B. (1967). The relationship of mental health to marital choice and courtship progress. Journal of Marriage and the Family, 29, 447–451.
OECD (2012). Average effective age of retirement versus the official age in 2012 in OECD countries Retrieved 3rd Feb 2014, from www.oecd.org/els/emp/Summary_2012_values.xls.
Parente, P., & Silva, S. (2012). A cautionary note on tests of overidentifying restrictions. Economics Letters, 115, 314–317.
Pevalin, D., & Ermisch, J. (2004). Cohabiting unions, repartnering and mental health. Psychological Medicine, 34, 1553–1559.
Productivity Commission. (2003). Social capital: reviving the concept and its policy implications. Canberra: Research Paper, AusInfo.
Raviv, A., Keinan, G., Abazon, Y., & Raviv, A. (1990). Moving as a stressful life event for adolescents. Journal of Community Psychology, 18, 130–140.
Ronconi, L., Brown, T., & Scheffler, R. (2010). Social capital and self-rated health in Argentina. Health Economics, 21, 201–208.
Schwarzer, R., Bowler, R., & Cone, J. (2013). Social integration buffers stress in New York police after the 9/11 terrorist attack. Anxiety, Stress, and Coping, 1, 18–26.
Tomita, A., & Burns, J. (2013). A multilevel analysis of association between neighborhood social capital and depression: evidence from the first South African National Income Dynamics Study. Journal of Affective Disorders, 10, 101–105.
Ware, J., Snow, K., Kosinski, M., & Gandek, B. (2000). SF-36 health survey: Manual and interpretation guide. Lincoln: QualityMetric Inc.
Weitzman, E., & Kawachi, I. (2000). Giving means receiving: the protective effect of social capital on binge drinking on college campuses. American Journal of Public Health, 90, 1936–1939.
White, H., & Lu, X. (2010). Robustness checks and robustness tests in applied economics UCSD Department of Economics discussion paper.
Wilkinson, R., & Pickett, K. (2009). The spirit level: Why greater equality makes societies stronger. New York: Bloomsbury Press.
Acknowledgements
Nicholas Rohde and Kam Ki Tang are supported by the ARC Discovery grant DP120100204.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper uses unit record data from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. The HILDA Project was initiated and is funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) and is managed by the Melbourne Institute of Applied Economic and Social Research (Melbourne Institute). The findings and views reported in this paper, however, are those of the author and should not be attributed to either FaHCSIA or the Melbourne Institute.
Any errors are the responsibility of the authors.
Rights and permissions
About this article

Cite this article
Rohde, N., D’Ambrosio, C., Tang, K.K. et al. Estimating the Mental Health Effects of Social Isolation. Applied Research Quality Life 11, 853–869 (2016). https://doi.org/10.1007/s11482-015-9401-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-015-9401-3