
Abstract
In recent years, mindfulness meditation has shown to be a promising approach for alleviating disability and dysfunction associated with a wide range of medical and psychiatric conditions. To date, there have been no controlled clinical studies of mindfulness for problem gambling (beyond case studies) despite the well-established presence of irrational beliefs and cognitive distortions which would suggest that mindfulness interventions would be particularly suitable. In the present study, a group, five-session, mindfulness intervention was integrated into an empirically-effective cognitive-behavioral therapy for problem gamblers. Compared to a wait list control the mindfulness intervention significantly reduced the severity of gambling, gambling urges and psychiatric symptoms at end-of-treatment. At the 3-month follow-up combining the results of both groups the results were maintained. In addition, a significant decrease in the proportion of the sample meeting criteria for pathological gambling was found. Those individuals who reported some mindfulness practice post-treatment showed significantly better clinical outcomes than did those who did not report any mindfulness practice suggesting that mindfulness did play a role in the outcomes observed. Taking into consideration the multiple methodological limitations of this pilot study there is sufficient evidence to further investigate the potential efficacy of mindfulness interventions for problem gambling.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Treatment of Problem Gambling
With prevalence estimates of pathological gambling ranging between 1 and 2 % of the population (Shaffer et al. 1999) and with an additional 5–6 % experiencing significant gambling problems, effective treatments for this increasingly common psychiatric disorder are clearly necessary. Recent critical reviews of the controlled gambling research (Toneatto and Ladouceur 2003; Pallesen, Mitsem, Kvale, Johnsen, and Molde 2005; Hodgins and Holub 2007) have concluded that cognitive-behavioral treatments show the greatest therapeutic benefits. These reviews have demonstrated that the most effective gambling treatments typically include a behavioral component, directed at reducing the stimulus cue properties of gambling activities and venues, and a cognitive component to target the maladaptive beliefs frequently held by gamblers. While cognitive-behavioral therapies for problem gambling are relatively effective a substantial proportion of treated gamblers do not make significant clinical progress (cf. review by Petry 2005). Petry’s (2005) review of randomized cognitive therapy trials demonstrated that outcomes were rather modest, with substantial improvements achieved by less than half of the sample. Daughters et al. (2003) have identified irrational beliefs and negative affect as two factors that are particularly predictive of treatment failure among problem gamblers.
Cognitive Characteristics of Problem Gambling
A major challenge to the development of effective treatments for problem gambling is the rigid and dysfunctional nature of the gamblers’ beliefs. Gambling-related cognitive psychopathology in particular is a well-substantiated characteristic of this disorder (e.g., Joukhador, Blaszczynski, and Maccallum 2004; Toneatto 1999; Hodgins and el-Guebaly 2004; Petry 2005; Toneatto and Nguyen 2007). Due to the ambivalence that often characterizes problem gambling, it is often difficult to directly modify these beliefs using conventional, content-focused techniques such as Socratic dialogue, logical analysis and empirical verification or to substantially diminish the conviction in their validity (Toneatto and Gunaratne 2009). Unless treated, however, such beliefs may reduce the impact of treatment and present potent triggers for relapse (e.g., Hodgins and el-Guebaly 2004). Since traditional cognitive-behavioral interventions may be limited in effectively modifying core beliefs about gambling outcomes (i.e., their predictability or controllability), alternative conceptualizations of problem gambling, gambling-related cognition, and effective intervention must be considered.
Mindfulness Interventions for Addictive Behavior
Recent years have witnessed the emergence of mindfulness interventions as an effective component of treatment for a wide number of clinical conditions (cf. Keng, Smoski and Robins 2011). Mindfulness meditation, unlike traditional psychological treatment, emphasizes the sustained, non-judgmental, accepting awareness of mental content, rather than the direct modification of mental events (Grabovac, Lau, and Willett 2011). For this reason, mindfulness approaches are often considered to be metacognitive in nature, targeting the attitudes and beliefs that are held about cognition. A popular mindfulness program, Mindfulness-Based Stress Reduction (MBSR), has been shown to reduce psychological morbidity associated with chronic illnesses as well as emotional and behavioral disorders (Kabat-Zinn 1990). A number of recent comprehensive reviews of the literature have demonstrated the efficacy of a number of mindfulness-based approaches for a wide range of clinical disorders (Keng et al. 2011). However, the poor quality of their research methodologies prevents firm conclusions about the efficacy of these approaches. Furthermore, a critical review of nine studies that evaluated mindfulness interventions for addiction concluded that the existing data do not strongly support mindfulness interventions for any substance use–related condition (Toneatto 2013). While some studies showed positive effects of mindfulness practice compared to baseline, these effects were not always found, were usually short-term, and tended to apply to non-substance related variables. Only a very limited direct benefit on substance use was found. While the promise of mindfulness meditation as an efficacious treatment for substance use disorders remains a potential at present, there is sufficient evidence to recommend continued investigation of this modality.
Mindfulness Interventions for Problem Gambling
Shonin, Van Gordon, and Griffiths (2013a) has recently written on the potential for mindfulness interventions (as one of a number of Buddhist- derived interventions) that held promise in the treatment of problem gambling. However, recent reviews of the mindfulness and problem gambling literature did not identify a single controlled study that evaluated the clinical effectiveness of mindfulness for problem gambling (Toneatto 2012; de Lisle et al. 2012) apart from three case studies (i.e., de Lisle et al. 2011; Toneatto et al. 2007; Shonin, Van Gordon, and Griffiths 2013b). In a non-clinical study, an inverse relationship between trait mindfulness and gambling pathology (Lakey, Campbell, Brown and Goodie 2007) suggesting mindfulness may attenuate severity of gambling. Shonin et al. (2013b) found that an 8-week mindfulness intervention embedded within a cognitive-behavioral treatment significantly ameliorated gambling symptoms that were maintained at a 3-month follow-up assessment. Despite the paucity of research investigating mindfulness among problem gamblers, the highly cognitive nature of problem gambling suggests that mindfulness may hold potential for managing gambling problems for several reasons. Given the relative difficulty in modifying gambling-related cognitive distortions (Toneatto and Gunaratne 2009), restructuring specific beliefs may be less beneficial than modifying the gambler’s response towards their own subjectivity. Mindfulness practice also encourages an attitude of skepticism towards gambling-related beliefs and provides the gambler a choice as to how to best respond, rather than react, to such beliefs (de Lisle, Dowling and Allen 2011). In addition, mindfulness meditation, through concentration on the breath as an anchor for awareness, can enhance the ability to focus attention and diminish distraction and ruminative thinking (Grabovac et al. 2011).
Mechanisms of the Clinical Effects of Mindfulness
The core skill defining mindfulness has been described as the capacity to respond to cognitive events (which can include thoughts, beliefs, imagery, perceptions, sensations, memories) with an attitude of acceptance, non-judgment, and present-focused awareness. Mindfulness may assist the individual to “recognize and disengage [de-center] from mind states characterized by self-perpetuating patterns of ruminative, negative thought” (Segal, Williams, and Teasdale 2002, p.75). Through sustained practice, the mindfulness practitioner can learn to discern between the stream of mental events that characterizes waking consciousness and the ‘observer’ of such cognitions. This discriminative skill allows the individual to disrupt automatic, conditioned, or impulsive responses to such mental events (Breslin et al. 2002). To the degree that one is able to observe mental events one is no longer embedded in or fused with its content. The result is a profound shift in one’s relationship to thoughts and emotions, along with concomitant clarity, perspective, objectivity, equanimity, and reduced ruminative reactivity. This fundamental shift has been labelled reperceiving (Shapiro, Carlson, Astin, and Freedman 2006), deautomatization (Deikman 1982), and cognitive defusion (Hayes, Strosahl, and Wilson 1999).
This pilot study represents the first controlled study of the benefit of integrating a mindfulness component into a cognitive-behavioral treatment for problem gambling, and had two goals: (i) to develop a mindfulness-enhanced cognitive-behavioral treatment for problem gamblers and, (ii) to test its feasibility and initial efficacy. This study was approved by the Research Ethics Board of the Centre for Addiction and Mental Health (CAMH).
Method
Participants
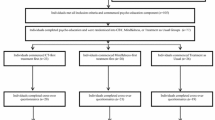
Eighteen pathological gamblers were recruited from the community using advertisements placed in local newspapers. The primary inclusion criterion was a current diagnosis of pathological gambling and the willingness to practice mindfulness meditation. Primary exclusion criteria included substance abuse/dependence (except nicotine) and concurrent attendance at any treatment in which gambling was addressed (including Gamblers Anonymous).
Baseline and Post-Intervention Assessment
All subjects completed the standard CAMH Intake Assessment for Problem Gamblers, which gathers data on gambling behavior, history, and patterns. In addition, gambling urges (Raylu and Oei 2004), current emotional distress (i.e., Brief Symptom Inventory, Derogatis 1983), and trait mindfulness (i.e., Kentucky Inventory of Mindfulness Skills; Baer, Smith, and Allen 2004) were also assessed.
Procedure
Following the baseline assessment, subjects were randomized to one of two conditions based on the order in which participants were admitted into the study (i.e. participant 1 assigned to M-CBT; participant 2 assigned to the wait-list control, etc.). The experimental group received a five-session, manual-guided, mindfulness-enhanced group cognitive-behavioral therapy for problem gambling (Mindfulness-enhanced Cognitive-Behavioral Treatment; M-CBT). A wait list group formed the control condition and received the active intervention following post-treatment assessment.
Each of the five sessions consisted of two distinct components: a 45-min cognitive-behavioral therapy session followed by a CD-guided mindfulness instruction (15-min) and a practice session (30-min). There were opportunities in each session for participants to discuss any difficulties encountered in their practice. Participants were asked to practice for 30 min per day at home. Descriptions of mindfulness by Kabat-Zinn (1990) and subsequent adaptations by Segal et al. (2002) provided a basis for the interventions utilized in the present study. The primary features of the mindfulness intervention included instruction in awareness of breathing as an anchor for present-focused attention, awareness of cognitive processes, especially thoughts about gambling, and shifting of attention from such thoughts to the breath without engaging in discursive engagement. The cognitive-behavioral component of the treatment, which was delivered in the first part of each session, instructed participants in traditional content-focused techniques such as behavioral problem-solving and cognitive restructuring. The mindfulness practice always followed the cognitive-behavioral instruction and was presented as an additional practice to assist the participant in managing their problem behavior by becoming aware of gambling-related thoughts and feelings in order to interrupt them from becoming threats to their treatment goals. Additional details regarding M-CBT can be obtained by contacting the first author (TT).
The first three treatment sessions were scheduled weekly, and the last two sessions scheduled every other week. The therapist (TT) delivering the therapy also guided the mindfulness and relaxation exercise. Both groups were re-assessed 2 weeks following the 5th treatment session, after which the wait list control group received M-CBT. All subjects were assessed 3-months post-treatment. At the follow-up, participants were asked to indicate the frequency of their mindfulness practice since completion of treatment.
Results
Description of Participants
The sample was middle-aged with an equal number of men and women. Most were non-partnered, unemployed, and modestly educated, with a mean duration of 12 years of problem gambling. The most common gambling behaviors were lottery and scratch tickets, followed by card games, slot machines, and sports betting. No statistical differences between the two groups were found (Tables 1 and 2).
Group Comparisons at Post-Treatment and Follow-Up
There were no significant group differences in gambling severity, psychiatric symptoms, gambling urges, or trait mindfulness at baseline.Footnote 1 However, at post-treatment, the M-CBT group reported significantly fewer DSM gambling symptoms than did the wait list control group (Table 3). Significant reductions between baseline and the 3-month follow-up on gambling severity, psychiatric symptoms, and gambling urges were also found indicating maintenance of the therapeutic gains (Table 4). Additionally, the proportion of participants who met diagnostic criteria for pathological gambling was also significantly reduced at the 3-month follow-up (21 %) compared to baseline (95 %) (Tables 3 and 4).
Association Between Mindfulness Practice During Follow-up and Outcomes
Of the 14 participants available for the 3-month follow-up, nine reported at least some mindfulness practice following the treatment while five did not practice at all. Participants who did practice mindfulness reported a M (SD) of 20.36 (25.20) days (out of a maximum of 90 days). The M (SD) duration of mindfulness practice was 14.64 (16.81) minutes per day for an approximate average of 5 h of mindfulness practice post-treatment. As Table 5 reveals, those who reported some mindfulness practice reported significantly fewer DSM symptoms, gambling urges, and psychiatric symptoms than those who did not report any mindfulness practice. The number of minutes of mindfulness practice was significantly correlated with a reduction in psychiatric symptoms as measured by the BSI (r = -.61, p < .05) (Table 5).
Discussion
Process-focused interventions, such as mindfulness meditation, may have the potential to improve the treatment efficacy for problem gambling (e.g., Shonin, Van Gordon, and Griffiths 2013a). Teaching gamblers to modify their responses to their own mental content rather than to directly modify what are often very recalcitrant and rigid beliefs has shown promise in a number of case studies (i.e., de Lisle et al. 2011; Toneatto et al. 2007; Shonin, Van Gordon, and Griffiths 2013b). As there is some evidence that gambling distortions do not always respond to direct treatment (e.g., Toneatto and Gunaratne 2009; Petry 2005) mindfulness intervention may enhance gambling treatment outcomes.
To date, however, no studies have examined the efficacy of mindfulness in the treatment of pathological gambling in a controlled study. The present study found that a 5-session intervention integrating mindfulness into cognitive-behavioral therapy was more effective than a wait list control in reducing the severity of gambling and associated urges and psychiatric symptoms. These gains were maintained at the 3-month follow-up.
Of course, these results cannot be conclusively attributed to the mindfulness intervention since it was an adjunct to CBT, an established empirically effective treatment. However, the finding that those who continued to practice mindfulness to some degree (i.e., about 1–2 times per week @ 15 min per session) during the follow-up performed better on the outcome variables than those who did not report any practice at all suggests that mindfulness practice likely did play a significant role.
The results of the study, albeit modest, suggest that mindfulness interventions for problem gambling should be further explored. However, any conclusion must be tempered by the significant methodological limitations of this study. The primary limitation of the study involves the nature of the control group. A wait list does not allow any definitive conclusion about the unique efficacy of the mindfulness intervention as none of the possible mediators for the benefits of the experimental treatment were controlled for. In addition, the small number of subjects, the absence of mindfulness data post-treatment, lack of corroboration of the dependent measures, and absence of direct measures of gambling behavior severely limit any conclusions that can be made for including mindfulness practice in gambling treatment. Additional research will be necessary to rectify these weaknesses and to better evaluate the efficacy of this modality. This first empirical study of the efficacy of a mindfulness enhancement of an empirically effective cognitive-behavioral treatment suggests that mindfulness interventions merit further research.
Notes
Statistical assumptions for the use of non-parametric tests were met; hence, t-tests were used to test for mean differences.
References
Baer, R. A., Smith, G. T., & Allen, K. B. (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11, 191–206.
Breslin, F. C., Zack, M., & McMain, S. (2002). An information-processing analysis of mindfulness: Implications for relapse prevention in the treatment of substance abuse. Clinical Psychology: Science and Practice, 9, 275–299.
Daughters, S. B., Lejuez, C. W., Lesiur, H. R., Strong, D. R., & Dolvensky, M. J. (2003). Towards a better understanding of gambling treatment failure: implications of translational research. Clinical Psychology Review, 23, 573–586.
de Lisle, S. M., Dowling, N. A., & Allen, J. S. (2011). Mindfulness-based cognitive therapy for problem gambling. Clinical Case Studies, 10, 210–228.
de Lisle, S. M., Dowling, N. A., & Allen, J. S. (2012). Mindfulness and problem gambling. Journal of Gambling Studies, 28, 719–739.
Deikman, A. J. (1982). The observing self. Boston: Beacon.
Derogatis, L.R. (1983). SCL-90-revised version manual-1. Johns Hopkins University School of Medicine.
Grabovac, A. D., Lau, M. A., & Willett, B. R., (2011). Mechanisms of mindfulness: A Buddhist psychological model. Mindfulness.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: An experiential approach to behavior change. New York: Guilford Press.
Hodgins, D. C., & el-Guebaly, N. (2004). Retrospective and prospective reports of precipitants to relapse in pathological gambling. Journal of Consulting and Clinical Psychology, 72, 72–80.
Hodgins, D. C., & Holub, A. (2007). Treatment of problem gambling. In G. Smith, D. C. Hodgins, & R. Williams (Eds.), Research and Measurement Issues in Gambling Studies (pp. 372–391). New York: Elsevier.
Joukhador, J., Blaszczynski, A., & Maccallum, F. (2004). Superstitious beliefs in gambling among problem and non-problem gamblers: Preliminary data. Journal of Gambling Studies, 20, 171–180.
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Delacorte.
Keng, S.-L., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: A review of empirical studies. Clinical Psychology Review, 31, 1041–1056.
Lakey, C. E., Campbell, W. K., Brown, K. W., & Goodie, A. S. (2007). Dispositional mindfulness as a predictor of the severity of gambling outcomes. Personality and Individual Differences, 43(7), 1698–1710.
Pallesen, S., Mitsem, M., Kvale, G., Johnsen, B. H., & Molde, H. (2005). Outcome of psychological treatments of pathological gambling: a review and meta-analysis. Addiction, 100, 1412–1422.
Petry, N. M. (2005). Pathological gambling: Etiology, comorbidity and treatment. Washington, DC: American Psychological Association.
Raylu, N., & Oei, T. P. (2004). The gambling related cognitions scale (GRCS): development, confirmatory factor validation and psychometric properties. Addiction, 99, 757–769.
Segal, Z., Williams, & Teasdale, J. (2002). Mindfulness-based cognitive therapy for depression. New York: Guilford Press.
Shaffer, H., Hall, M. N., & Bilt, J. V. (1999). Estimating the prevalence of disordered gambling behavior in the United States and Canada: A Research Synthesis. American Journal of Public Health, 89, 1369–1376.
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62, 373–386.
Shonin, E., Van Gordon, W., & Griffiths, M. D. (2013a). Buddhist philosophy for the treatment of problem gambling. Journal of Behavioural Addictions, 2, 63–71.
Shonin, E., Van Gordon, W., & Griffiths, M. D. (2013b). Cognitive behavioral therapy (CBT) and meditation awareness training (MAT) for the treatment of co-occurring schizophrenia and pathological gambling: A case study. International Journal of Mental Health and Addiction. doi:10.1007/s11469-013-9460-3. Published online 06 December 2013.
Toneatto, T. (1999). Cognitive psychopathology of problem gambling. Substance Use and Misuse, 34, 1593–1603.
Toneatto, T. (2012). Gambling. In S. C. Hayes & M. Levin (Eds.), Acceptance, mindfulness, values, and addictive behaviors: Counseling with contemporary cognitive behavioral therapies. Oakland: New Harbinger Publications.
Toneatto, T. (2013). Mindfulness. In P. M. Miller (Ed.), Encyclopedia of Addiction. London: Elsevier.
Toneatto, T., & Gunaratne, M. (2009). Does the treatment of cognitive distortions improve clinical outcomes for problem gambling? Journal of Contemporary Psychotherapy, 38, 221–229.
Toneatto, T., & Ladouceur, R. (2003). The treatment of pathological gambling: A critical review of the literature. Psychology of Addictive Behaviors, 284–292.
Toneatto, T., & Nguyen, L. (2007). Does mindfulness meditation improve anxiety and mood symptoms? A review of the controlled research. Canadian Journal of Psychiatry, 52, 260–266.
Toneatto, T., Vettese, L., & Nguyen, L. (2007). The role of mindfulness in the cognitive-behavioral treatment of problem gambling. Journal of Gambling Issues, Issue, 19, 91–100.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Toneatto, T., Pillai, S. & Courtice, E.L. Mindfulness-Enhanced Cognitive Behavior Therapy for Problem Gambling: A Controlled Pilot Study. Int J Ment Health Addiction 12, 197–205 (2014). https://doi.org/10.1007/s11469-014-9481-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-014-9481-6