
Abstract
This study uses a national child welfare dataset to examine the profile of young parents who are the subject of maltreatment-related investigation and to identify which factors determine service provision from the child welfare system at the conclusion of the investigation. Specifically, it examines how workers in the child welfare system decide which young parents require ongoing services the conclusion of a maltreatment related investigation where other risk factors are also being assessed. It found that young parents are struggling with a number of issues including poverty, housing, mental health, violence and children who are exhibiting functioning concerns. Workers in the child welfare system provide ongoing services to young parents particularly in investigations where they have noted concerns around drug/solvent use, cognitive impairment, mental health issues, physical health issues and few social supports. The opportunity to target interventions for the specific concerns for this very vulnerable population is evident.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
There is ample evidence in the maltreatment literature that children of young parents are at increased risk of maltreatment (Connelly and Straus 1992; Lee and George 1999; Stier et al. 1993). Having children in adolescence and young adulthood may impact identity development with the resultant adjustment issues negatively impacting parenting and parent–child relationships whereby child maltreatment is a possible outcome (Afifi 2007). Young parents are more likely to lack caregiving skills, live in poverty, drop out of secondary school education, and misuse substances (Zuravin and DiBlasio 1996; Afifi 2007). Although children of young parents are commonly identified as at-risk for child maltreatment, little information exists about the characteristics of young parents who are identified to child welfare services for maltreatment-related concerns.
In order to address this dearth in the literature, this study uses a national child welfare dataset to examine the profile of young parents who are the subject of maltreatment-related investigation and to identify which factors determine service provision at the conclusion of the investigation. Specifically, it examines how workers in the child welfare system decide which young parents require ongoing services at the conclusion of a maltreatment related investigation where other risk factors in addition to being a young parent are also assessed. This study provides an opportunity to understand the needs of this population by describing some of the challenges that young parents are coping with while caring for their children. Early interventions in key areas could improve the outcomes for young parents and their children.
Background
In Canada, a decline in the rate of teenage pregnancy has been observed over the past two decades (McKay 2006; Statistics Canada 2006). According to data collected by Statistics Canada (2010), in 2005 the rate of teenage pregnancy was 29.2 pregnancies per 1,000 women aged 15 to 19. The pregnancy rates for older teenagers was much higher than younger teenagers as the reported rates were 15.8 pregnancies per 1,000 women aged 15 to 17 in comparison to 49 per 1,000 women aged 18 to 19. Among women aged 20 to 24, the rate was higher than the rate of teenage pregnancies at 79.4 pregnancies per 1,000 women. This rate continued to increase among women aged 25 to 29 with the rate at 118.9 pregnancies per 1,000 women. The average age among women who gave birth for the first time in Canada in 2003 was 28 years (Statistics Canada 2006).
There is some evidence adolescent mothers may be over represented in reporting and investigating child maltreatment due to the presence of other risk factors such as poverty, low academic achievement, drug abuse (Lee and George 1999). Higher unemployment among adolescent parents, unequal division of household labour, low income, lower levels of education, and cultural beliefs regarding corporal punishment are all conditions that are more likely to occur for adolescent parents (Afifi 2007). Zuravin and DiBlasio (1996) conducted a study comparing non-maltreating adolescent mothers and adolescent mothers who maltreated their children. The authors found that adolescent mothers who abused their children were more likely to have a mother with emotional problems, preferred to be alone during their childhood, lived with a family that received social assistance, and were less likely to have had a positive attachment to their primary mother figure. Preferring to be alone was the strongest correlate for abusive behaviour followed by having a mother with emotional problems, receiving social assistance, and having two or more children by the time they turned 19. Zuravin and DiBlasio (1996) also found that adolescent mothers who neglected their children were more likely to have been sexually abused, run away from home, had gotten in trouble with the law, resided with different caregivers, had their first child at a younger age, and had a premature or low birth weight first child. Having two or more children by the age of 18 was found to be the strongest predictor of child neglectful parenting behaviour followed by trouble with the law, different caregivers during their childhood, completion of fewer grades at school, an abortion or miscarriage prior to the birth of their first child, and experiencing depression after the birth of their first child.
Maternal age and poverty have been found to be significant predictors of substantiated reports of child maltreatment (Lee and George 1999). The risk of substantiated child maltreatment is compounded when the two factors are present as “a child born to a very young mother living in a high-poverty area has a substantially higher risk of a substantiated report of child maltreatment than a child who possesses only one of the two risk factors” (Lee and George 1999, p. 775). This finding was equally significant among all types of child maltreatment allegations including, sexual abuse, other abuse and neglect. A study in the United Kingdom examining the risk of maltreatment in young children found that young parents with low academic achievement and a history of mental illness or childhood abuse were more likely to be investigated for child maltreatment or to have a child placed on the child protection register (Sidebotham and Heron 2006). Overall, young parents represented approximately 30% of children investigated and placed on the child protection register.
There is evidence of intergenerational transmission of child maltreatment among young parents (Dixon et al. 2005a; Kim 2009). According to Dixon et al. (2005a), being a parent under the age of 21, having a history of mental illness or depression, and living with a violent adult accounted for 53% of intergenerational transmission of child maltreatment, with age being the most significant risk factor. The authors found that the presence of these three risk factors among parents who were physically and/or sexually abused as a child, increased the odds by 17 times that parents would maltreat their own children in comparison to parents with those risk factors and no childhood history of victimization. Poor parenting styles combined with the aforementioned risk factors increased the total effect to 62% (Dixon et al. (2005b). Moreover, a national study of mother’s age and the risk of physical abuse found that the younger the mother is at the time of her first child, the higher the probability of child abuse, however mother’s age at the time of the abuse was not a significant factor (Connelly and Straus 1992).
Felix et al. (2003) examined the influence of cross-generational parenting on psychosocial functioning among adolescents in state care. Young mothers in state wardship who reported that their primary parenting figure had been an adolescent parent exhibited significantly higher total parenting stress, experienced less satisfaction from interactions with their child, and faced greater feelings of depression and role restriction than young mothers in state wardship whose primary parenting figure was not an adolescent parent (Felix et al. 2003). Similarly, Budd et al. (2000) examined the psychosocial factors of child maltreatment risk among adolescent mothers who were wards of the child protection system. Adolescent mothers in state wardship, and considered at risk for perpetuating child abuse reported significantly greater global emotional distress and lower social support satisfaction than adolescent mothers not at risk (Budd et al. 2000). Adolescent mothers at risk were also found to have lower academic achievement and fewer years of completed education.
Researchers examining childhood history of abuse and the risk abusive behaviour among mothers found that adolescent mothers who reported experiencing physical abuse are at higher risk for physically abusing their children during the first 18 months after the birth of their child in comparison to adult mothers who experienced physical abuse (De Paul and Domenech 2000). Romano et al. (2006) also found that a history of experiences of child maltreatment was prevalent among high-risk pregnant adolescents. In a study by Kim (2009) young parents who reported childhood victimization are more likely to exhibit the same problematic parenting behaviour towards their own children. More than half of the young parents interviewed reported experiencing neglect, physical abuse, or sexual abuse during their childhood. Young parents who report experiencing neglect in their childhood are 2.6 times more likely to report their own neglectful parenting behaviour and twice as likely to report physically abusive parenting. Young parents who report experiencing physical victimization in their childhood are five times more likely to report physically abusive parenting and 1.4 times more likely to report neglectful parenting. A study comparing three generations of sexually abused women demonstrated that children born to mothers who experienced sexual abuse were more likely to be born prematurely, have an adolescent mother, and be involved with child welfare services (Noll et al. 2009).
There are few studies that specifically examine teen biological fathers. Bolton (1987) examined young fathers in relationships with young mothers considered to be at risk of child maltreatment and found that young fathers are more likely to be ethnic minorities, live in poverty, have completed less years of education, experienced barriers to employment and unstable financial support. Young fathers were also found to have alcohol and substance use issues, involvement with the criminal justice system, and difficultly controlling their temper. These factors were found to affect young fathers’ relationships with young mothers and their parenting.
A study of interpartner conflict and child abuse risk among minority adolescent couples found that interpartner violence prior to childbirth was significantly associated with physically punitive parenting among fathers (Moore and Florsheim 2008). Young parents observed as “more warmly engaged” with one another prior to the birth of their child reported lower rates of physically punitive parenting 2 years after the birth of their child. Conversely, hostile interactions between young parents prior to the birth of their child were associated with fathers’ hostility toward the child during play 2 years later.
Children raised by teen parents are at risk for a range of detrimental trajectories, including poor educational, vocational, and health-related outcomes (Maynard and Hoffman 2008), and are at increased risk of maltreatment (Connelly and Straus 1992; De Paul and Domenech 2000). A study comparing risk of child maltreatment among younger mothers and older mothers demonstrated that children of mothers under the age of 18 experienced child maltreatment, which included definite and probable physical abuse, sexual abuse, and neglect, twice as often than children of mothers over the age of 18 (Stier et al. 1993).
Ongoing Services
The decision to provide ongoing services after a child maltreatment investigation has serious resource implications. In a fiscally-constrained child welfare service environment, decisions regarding which families and children receive scarce services needs to be understood. Generally, substantiation is highly correlated with the decision to provide ongoing services (DePanfilis and Zuravin 2001; Freeman et al. 1996; Winefield and Bradley 1992). However, DePanfilis and Zuravin (2001) found that families with a previous substantiated report were 22% less likely to receive ongoing services than families with no previous substantiated maltreatment. Referrals made by a professional and prior case opening were a predictor of case opening (Rossi et al. 1999; Zuravin et al. 1995). Non-compliance or a lack of cooperation from the caregivers was associated more with the decision to open the case than to close it (Wolock 1982). Other predictor variables which have been found to be associated with the decision to provide ongoing services include mother’s age (younger mothers are more likely to be provided ongoing services) as well as type and severity of maltreatment; childhood history of abuse or neglect by a parent; the number of children in the home; caregiver impairments; and level of social support (DePanfilis and Zuravin 2001; English et al. 1999). A referral for ongoing services was mostly likely made in cases where both maternal drug and alcohol issues were noted by the child protection worker (DePanfilis and Zuravin 2001).
DePanfilis and Zuravin (2001) found that substantiated cases of neglect were 20% less likely to receive ongoing services than substantiated cases of physical abuse. Jonson-Reid (2002) examined the decision to provide services among children reported for maltreatment. Children between the ages of seven and ten who were reported for physical abuse and those reported for neglect were equally likely to be referred for ongoing services. Children under the age of 14 who were reported for sexual abuse were more likely to be referred for ongoing services than children who were reported for physical abuse or neglect. Early adolescents (aged 11 to 14) were more likely to be referred for ongoing services than children between the ages of seven to ten and 15 to 17.
Research Questions
-
1)
How many adolescent parents are the subject of a maltreatment investigation? What proportion of child maltreatment related investigations involve primary caregiver 30 years of age and under?
-
2)
What are the characteristics of young parents identified to the child welfare system?
-
3)
Given that young parenthood is a risk factor for child maltreatment, how do workers in the child welfare system decide which young parents require ongoing services at the conclusion of a maltreatment related investigation?
Methodology
To address the research questions a secondary analysis of the Canadian Incidence Study of Reported Child Abuse and Neglect CIS-2008 (PHAC 2010) dataset was conducted. This unique dataset contains information about key clinical factors collected during the course of a child maltreatment investigation (Trocmé et al. 2010a). The CIS-2008’s primary objective was to produce a national estimate of the incidence of child maltreatment in Canada in 2008 (Trocmé et al. 2010b). Using a multi-stage sampling design, a representative sample of 112 child welfare sites was selected from 412 child welfare service areas in Canada (Trocmé et al. 2010c). A stratified cluster sampling design is used first to select a representative sample of child welfare offices and then to sample cases within these offices. Cases opened for service at the randomly selected sites between October 1st and December 31st Footnote 1 were eligible for inclusion (Trocmé et al. 2010d). Three months was considered to be the optimum period to maintain participation and compliance with study procedures. The final sample selection stage involved identifying children who had been investigated as a result of concerns related to possible maltreatment. Maltreatment related investigations that met the criteria for inclusion in the CIS include situations where there are concerns that a child may have already been abused or neglected as well as situations where there is no specific concern about past maltreatment but where the risk of future maltreatment is being assessed.
In most jurisdictions cases are open at the level of a family, which meant that procedures had to be developed to determine which specific children in each family had been investigated for maltreatment related reasons. In jurisdictions outside of Québec, children eligible for inclusion in the final study sample were identified by having child welfare workers indicate on the data collection instrument which children were being investigated because of maltreatment-related concerns (i.e., investigation of possible past incident(s) of maltreatment or assessment of risk of maltreatment). In Québec, the identification of maltreatment-related investigations was done by including all “retained”Footnote 2 cases with maltreatment-related case classification codes.
Sample
These procedures yielded a final sample of 15,980 children investigated because of maltreatment related concerns. There was missing data about the age of the primary caregiver in 236 investigations. This study focused on biological caregivers, 30 years of age and under (n = 5,222) and whether or not they were transferred to ongoing services at the conclusion of the investigation. The sample was further divided into four categories of investigations involving primary caregivers who were: biological fathers 30 years of age and younger, biological mothers less than 16 to 18 years, biological mothers 19–21 years, and biological mothers 22–30. The derivation of these categories was driven by practical as well as theoretical considerations. The sample of non biological caregivers in these age categories was too small to analyze (n = 6). The sample of biological fathers who were considered primary caregivers was too small to divide into more specific age groups. Although children of young teen parents are at higher risk for maltreatment, the sample of investigations involving biological mothers under the age of 16 was too small to analyze separately; therefore, it was combined with 16–18 year olds. The 22–30 years of age category could not be disaggregated. As the average age of women giving birth in Canada in 2007 was 29.3 years (Statistics Canada 2008), the biological mothers between 22 and 30 years of age were included in the analysis as a category of young mothers.
Two sets of weights are applied in order to derive national annual estimates. First, results are annualized to estimate the volume of cases investigated by each study site over the whole year. To account for the non-proportional sampling design, regional weights are then applied to reflect the size of each site relative to the child population in the region from which the site was sampled. CIS estimates cannot be unduplicated because annualization weights are based on unduplicated service statistics provided by the study sites. Therefore, estimates for the CIS refer to child maltreatment investigations. The final weighted sample for child maltreatment investigations where the primary age of the caregiver was indicated was 77,183 biological caregivers 30 years of age and under.
Measures
The information was collected using a three-page data collection instrument. Data collected by this instrument included the following: type of investigation (maltreatment or risk only); functioning concerns for the children and their caregivers; whether the household runs out of money; household hazards, and information about short-term service dispositions. Key clinical variables were included in the model in order to reflect an ecological theory and to determine the relative contribution of clinical variables to the decision to provide ongoing services which are considered in the young parenting and child welfare literature and available in the dataset.
Outcome Variable
Transferred to Ongoing Services
Workers were asked to indicate whether the investigation would be opened for ongoing child welfare services at the conclusion of the investigation. The decision to transfer a case to ongoing services is a dichotomous variable.
Predictor Variables
Primary Caregiver Functioning
Workers could note up to nine functioning concerns for the primary caregiver. Concerns were: alcohol abuse, drug/solvent abuse, cognitive impairment, mental health issues, physical health issues, few social supports, victim of domestic violence, perpetrator of domestic violence, and history of foster care/group home. Caregiver functioning variables were dichotomous variables with a suspected or confirmed concern coded as noted and no and unknown coded as not noted.
No Second Caregiver in the Home
Workers were asked to describe up to two caregivers in the home. If there was only one caregiver described there was no second caregiver in the home.
Household Hazards
Workers were asked to note if the following hazards were present in the home at the time of the investigation: accessible weapons, accessible drugs, production/trafficking of drugs, chemicals/solvents used in drug production, other home injury hazards, and other home health hazards. The presence of at least one household hazard is a dichotomous variable.
Household Regularly Runs Out of Money
Workers were asked to note if the household regularly runs out of money.
Number of Moves
Number of moves reflects the number of moves the household had experienced in the past 6 months. Number of moves was a categorical variable: no moves, one move, two or more moves and unknown moves.
Child Functioning
Workers could note up to 18 functioning concerns for the investigated child, indicating whether the concern had been confirmed, suspected, was not present or it was unknown to the worker. Child functioning variables were dichotomous variables with a suspected or confirmed concern coded as noted and no and unknown coded as not noted. Since the mean age of the children in investigations involving young parents was 3.8 years, analyses focused on five possible child functioning issues related to young children: attachment, intellectual/developmental disability, FAS/FAE, positive toxicology at birth, and physical disability.
Risk Related Investigations
Workers indicated whether the focus of the investigation was on a past incident or allegation of maltreatment or a future concern of maltreatment. Investigations were coded as either a risk only investigation or a maltreatment investigation.
Type of Maltreatment
Workers could indicate up to three forms of investigated maltreatment on the data collection instrument from 32 possible maltreatment codes as defined in the CIS-2008 Study Guidebook (Trocmé et al. 2010a). This analysis focused on the primary maltreatment concern of the investigation. The maltreatment typology used five key categories of maltreatment: physical abuse, sexual abuse, neglect, emotional maltreatment and exposure to intimate partner violence.
Data Analysis
A first set of descriptive bivariate analyses were conducted to explore the characteristics of investigations involving young biological primary caregivers. Bivariate analyses were also conducted to determine the relationship between the outcome variable and each theoretically relevant predictor variable. All bivariate analyses tests of significance were done using the sample weight which adjusts for inflation of the chi-square statistic by the size of the estimate by weighting the estimate back down to the original sample size. An independent t-test was conducted for child age.
For the multivariate model, the goal was to understand which predictors of the decision to transfer a case were significant. Logistic regression was used to predict the outcome variable ongoing service provision. Logistic regression is suited to the type of data that is consistently found in social and behavioural research, where many of the dependent variables of interest are dichotomous and the relationships among the independent and dependent variables are not necessary linear (Walsh and Ollenburger 2001). Logistic regression uses maximum likelihood estimation after the dependent variable has been transformed into a logit variable. The logit variable is the log of the odds of the dependent variable occurring. Through this means, logistic regression can estimate the probability of an event occurring (Walsh and Ollenburger 2001). In a marginal model, the regression of the outcome on the predictor variables is estimated separately from the within-level correlations and the variances of the regression coefficients. In the CIS-2008 dataset, there are multiple children investigated in one family. In order not to violate the assumption of independence, one child was randomly selected from each investigation.
A two-step analysis procedure was used. All analyses were conducted using SPSS, version 17.0. Unweighted data were used in all models. Only significant predictor variables at the bivariate level (p < .05) were included in the multivariate model. The choice of cutoff point for the decision to provide ongoing services was set at 0.3 which reflects the proportion of investigations transferred to ongoing services for this population. From the first model were extracted predictors with a significant relationship (p < .05) to the decision to transfer the case to ongoing child welfare services. The model was then run with this smaller set of predictors, only retaining significantly associated predictors (p < .05). This last set of independent variables finally leads to a model where all regression coefficients were significantly different from zero (p < .01). There is no universal strategy to dealing with missing data (Menard 2002). In this analysis, missing data was not included in the bivariate or mutilvariate analysis.
Results
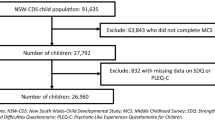
Biological parents are the primary caregivers in 93% of the total CIS sample (see Fig. 1). One third of all caregivers identified in the CIS sample are biological caregivers 30 years of age and under (33%). The smallest group of young biological caregivers are biological mother less than 16 years of age to 18 (3% of biological parents, 30 years of age and under), while the largest age category of young primary caregivers are biological mothers, age 22–30 years (81% of biological caregivers, 30 years of age and under) (see Table 1).

Age of primary caregivers in child maltreatment-related investigations in Canada in 2008
The characteristics of young primary caregivers investigated by child welfare for a maltreatment related concern are reported in Table 2. All caregiver risk factors are significantly different between groups of caregivers by age (X 2 = 20.45). Alcohol (an estimated 923 investigations; 28%) and drug/solvent abuse (1,025 investigations; 31%) are noted mostly for investigations involving young biological fathers. Mental health issues are most commonly noted for young biological mothers ages 18 and under (27%). Few social supports (38%), victim of domestic violence (39%), and history of foster care (23%) were most frequently reported for biological mothers 19 to 21 years of age. Only two child functioning issues were statistically significant: attachment issues (X 2 = 13.59), and intellectual/developmental disabilities (X 2 = 14.90). These child functioning concerns were more likely to be reported in investigations involving biological mothers 22 to 30 years of age (both 7%).
Biological mothers 18 years and under had moved most frequently in the past year (54%): 35% moved once in the past 12 months, and 19% moved 2 or more times in the last 12 months (X 2 = 88.53). The concern of ‘household regularly runs out of money’ was documented for investigations involving biological mothers 22 to 30 years (15%) (X 2 = 27.42).
Investigations for risk only were most common for biological mothers 18 years and under (44%). Of the maltreatment types, physical abuse was most common for investigations involving biological fathers (22%); sexual abuse (7%) and neglect (35%) were highest among biological mothers 19 to 21 years. Emotional maltreatment was similar across age groups and exposure to intimate partner violence the primary focus of the investigation for biological mothers 22 to 30 years (24%) (X 2 = 65.40).
Investigations transferred to ongoing services and those investigations closed at the conclusion of the investigation were compared. All caregiver risk factors and child functioning issues were more frequently reported in investigations transferred to ongoing child welfare services. Other risk factors were also more likely to be significantly related to the decision to provide services such as the household regularly runs out of money for basic necessities: 27% of investigations kept open for ongoing child welfare services compared to 9% of those that closed after the initial investigation (X 2 = 301.48). Two or more moves was most frequently noted for investigations kept open (20% compared to 9%). At least one household hazard in the home was noted for 18% of investigations kept open compared to only 6% of those closed (X 2 = 147.85) (See Table 3).
The final regression model can be found in Table 4 (R2 = .30). Only the significant predictors at the bivariate and multivariate levels were entered into this model (see methods section). The model correctly classified 71% of the investigations.
The presence of primary caregiver risk factors significantly increases the odds of service provision. Even when controlling for all statistically relevant predictors, investigations involving biological mothers 18 years and under were more than twice as likely to be kept open for ongoing child welfare services compared to biological mothers 22 to 30 years of age. Investigations involving young biological fathers, and biological mothers 19 to 21 years of age were almost 1.5 times more likely to be kept open compared to investigations involving biological mothers 22 to 30 years.
Discussion
The CIS-2008 dataset provides a unique opportunity to examine the profile of young parents reported to child welfare organizations and the predictors of the decision to provide ongoing services. Almost one third of primary caregivers reported to the child welfare system in Canada are 30 years of age or under. Young parents reported to the child welfare system for a maltreatment-related concern were facing a number of challenges and concerns. Workers in investigations involving all young parent age groups frequently noted concerns around housing (stability and the presence of hazards), poverty, few social supports, drug use, alcohol abuse and mental health. Some important differences emerged between the age categories of young parents for both parents and their children. Not surprisingly, the age groups with the most number of caregiver risk factors are biological mothers less than 16 years of age to 18 years of age and biological mothers 19 to 21 years of age. These two age categories were more likely to have experiences a move than biological fathers and biological others. Almost one quarter of biological mothers 21 years if age and under had a history of foster care or group home.
Risk factors noted for the primary caregiver are the most important considerations for workers when deciding to transfer the case to ongoing services. Caregiver risk factors explained most of the variance described in the model (approximately 25% of the total variance). The risk factors which remained significant in the final model were drug/solvent use, cognitive impairment, mental health issues, physical health issues and few social supports. The type of investigation (whether it was focused on a specific allegation or concern of past maltreatment, or a concern for future maltreatment) was not a predictor of the decision to provide services even when controlling for specific maltreatment types. This is likely an indication that workers are clinically more concerned about parenting skills than the type of event experienced by the investigated child.
It is interesting to note which risk factors were not statistically significant when controlling for all predictors, primarily history of foster care group home. Although the literature points to both childhood maltreatment and history of foster care as a risk factor for a maltreating parent, when controlling for other concerns of the investigation it did not remain significant. This suggests that young parents who have their own histories of child welfare involvement may be over-identified to the child welfare system for a maltreatment related concern but only the parents with functioning concerns that present risks to their children are opened for service provision.
Adolescent mothers are more likely to experience intimate partner violence than adult mothers (Gielen et al. 1994). In almost 40% of investigations involving young parents, workers noted that the caregiver was a victim of intimate partner violence. Although intimate partner violence is an issue for all age groups, it did not remain significant either as a risk factor for the young parent or as a maltreatment type. This is consistent with Black et al. (2008) who found that investigations involving intimate partner violence were less likely to be transferred to ongoing services.
Although approximately half of the young biological mothers (less than 16 to 18 and 19 to 21 years) were reported to have moved one or more times during the past year, housing was not found to be a significant risk factor in predicting the decision to provide ongoing services. This may be an indication that since a high proportion of investigations involve transiency this predictor does not necessarily factor into a clinical concern or possible intervention for the child welfare system. In contrast, households that regularly ran out of money for monthly expenses were almost twice as likely to be transferred to ongoing services as households that did not run out of money. This finding is consistent with the existing literature identifying young parents’ vulnerability to unemployment and poverty and its potential detrimental impact on their parenting.
Several child functioning issues noted in investigations were found to be significant predictors of ongoing services. The child functioning concerns which remained significant in the final model were attachment issues, failure to meet developmental milestones, FAS/FAE and positive toxicology at birth. Poor attachment is consistent with a study conducted by Bailey et al. (2007) who found that unresolved attachment and childhood experiences of maltreatment were prevalent among at-risk adolescent mothers. The researchers posit that the teen mothers’ unresolved attachment may affect their ability to develop a positive and functional relationship with their own child. FAS/FEA and positive toxicology at birth as significant predictors of ongoing service are consistent with research indicating that mothers with drug or alcohol issues are more likely to be referred for ongoing services (DePanfilis and Zuravin 2001; Lee and George 1999).
Although all age groups demonstrated has a significant number of risk factors, it is interesting to note that the age of young biological mothers (less than 16–18 and 19–21 years) was a statistically significant predictor of the decision to provide child welfare services when compared to 22–30 year old mothers. Age of biological fathers did not remain significant. Very young parents remained a concern for the investigating worker even when controlling for all other clinical variables because of a dual vulnerability: very young mothers have young children and the potential for harm requires the child welfare system to be vigilant.
Limitations
Data from the CIS-2008 are collected directly from the investigating worker and are not independently verified. These data only represent the concerns that present during an average 6 week investigation period. Additional concerns for the child and the caregiver could arise after the initial investigation. The analysis used a proxy measure of poverty. No educational data was collected in the CIS-2008. Even though the age of the caregiver of the time of the birth of their first child is an important consideration in the literature, a limitation of this study is that it cannot be derived from these data.
Conclusion
This study described the profile of young parents reported to the child welfare system for a maltreatment related concern. It found that young parents are struggling with a number of issues including poverty, housing, mental health, violence and children who are exhibiting functioning concerns. Workers in the child welfare system provide ongoing services to young parents particularly in investigations where they have noted concerns around drug/solvent use, cognitive impairment, mental health issues, physical health issues and few social supports. The opportunity to target interventions for the specific concerns for this very vulnerable population is evident. Struggling with the demands of adolescence and young adulthood while becoming a parent requires a multi-faceted approach to intervention including drug and alcohol treatment programs, housing.
Notes
In several Aboriginal jurisdictions, this adjustment was made to accommodate late enrolment of some Aboriginal sites.
Agencies in Quebec use a structured phone screening process whereby approximately half of all referrals are “retained” for evaluation. In Québec, the CIS sampled retained maltreatment related reports that involved cases that were not already open.
References
Afifi, T. O. (2007). Child abuse and adolescent parenting: Developing a theoretical model from an ecological perspective. Journal of Aggression, Maltreatment & Trauma, 14(3), 89–105.
Bailey, H. N., Moran, G., & Pederson, D. R. (2007). Childhood maltreatment, complex trauma symptoms, and unresolved attachment in an at-risk sample of adolescent mothers. Attachment & Human Development, 9(2), 139–161.
Black, T., Trocmé, N., Fallon, B., & MacLaurin, B. (2008). The Canadian child welfare system response to exposure to domestic violence investigations. Child Abuse & Neglect, 32, 393–404.
Bolton, F. G., Jr. (1987). The father in the adolescent pregnancy at risk for child maltreatment. I. Helpmate or hindrance? Journal of Family Violence, 2(1), 67–80.
Budd, K. S., Heilman, N. E., & Kane, D. (2000). Psychosocial correlates of child abuse potential in multiply disadvantaged adolescent mothers. Child Abuse & Neglect, 24(5), 611–625.
Connelly, C. D., & Straus, M. A. (1992). Mother’s age and risk for physical abuse. Child Abuse & Neglect, 16, 709–718.
De Paul, J., & Domenech, L. (2000). Childhood history of abuse and child abuse potential in adolescent mothers: A longitudinal study. Child Abuse & Neglect, 24(5), 701–713.
DePanfilis, D., & Zuravin, S. J. (2001). Assessing risk to determine the need for services. Children and Youth Services Review, 23(1), 3–20.
Dixon, L., Browne, K., & Hamilton-Giachritsis, C. (2005a). Risk factors of parents abused as children: a meditational analysis of the intergenerational continuity of child maltreatment (part I). Journal of Child Psychology and Psychiatry, 46(1), 47–57.
Dixon, L., Hamilton-Giachritsis, C., & Browne, K. (2005b). Attributions and behaviours of parents abuse as children: a meditational analysis of the intergenerational continuity of child maltreatment (part II). Journal of Child Psychology and Psychiatry, 46(1), 58–68.
English, D., Marshall, D., Brummel, S., & Orme, M. (1999). Characteristics of repeated referrals to child protective services in Washington State. Child Maltreatment, 4(4), 297–307.
Felix, E. D., Kelly, A. O., Poindexter, L. M., & Budd, K. S. (2003). Cross-generational parenting influences on psychosocial functioning of adolescent mothers in substitute care. Journal of Adolescent Research, 18(2), 154–168.
Freeman, J., Levine, M., & Doueck, H. (1996). Child age and caseworker attention in child protection service investigations. Child Abuse & Neglect, 20(10), 907–920.
Gielen, A. C., O’Campo, P. J., & Faden, R. (1994). Interpersonal conflict and physical violence during childbearing years. Social Science & Medicine, 39, 781–787.
Jonson-Reid, M. (2002). After a child abuse report: Early adolescents and the child welfare system. Journal of Early Adolescence, 22(1), 24–48.
Kim, J. (2009). Type-specific intergenerational transmission of neglectful and physically abusive parenting behaviors among young parents. Children and Youth Services Review, 31, 761–767.
Lee, B. J., & George, R. M. (1999). Poverty, early childbearing, and child maltreatment: A multinomial analysis. Children and Youth Services Review, 21, 755–780.
Maynard, R. A., & Hoffman, S. D. (2008). The costs of adolescent childbearing. In S. D. Hoffman & R. A. Maynard (Eds.), Kids having kids: Economic and social consequences of teen pregnancy (2nd ed., pp. 359–402). Washington: The Urban Institute.
McKay, A. (2006). Trends in teen pregnancy in Canada with comparisons to U.S.A and England/Wales. The Canadian Journal of Human Sexuality, 15(3–4), 157–161.
Menard, S. (2002). Applied logistic regression analysis, second edition. Thousand Oaks, CA: Sage.
Moore, D. R., & Florsheim, P. (2008). Interpartner conflict and child abuse risk among African American and Latino adolescent parenting couples. Child Abuse & Neglect, 32, 463–475.
Noll, J. G., Trickett, P. K., Harris, W. W., & Putnam, F. W. (2009). The cumulative burden borne by offspring whose mothers were sexually abused as children: Descriptive results from a multigenerational study. Journal of Interpersonal Violence, 24(3), 424–449.
Public Health Agency of Canada. Canadian incidence study of reported child abuse and neglect—2008: Major findings. Ottawa, 2010.
Romano, E., Zoccolillo, M., & Paquette, D. (2006). Histories of child maltreatment and psychiatric disorder in pregnant adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 45(3), 329–336.
Rossi, P. H., Schuerman, J., & Budde, S. (1999). Understanding decisions about child maltreatment. Evaluation Review, 23(6), 579–598.
Sidebotham, P., & Heron, J. (2006). Child maltreatment in the “children of the ninties”: A cohort study of risk factors. Child Abuse & Neglect, 30, 496–522.
Statistics Canada. (2006). Health indicator: Canada. Catalogue no. 82–211. Retrieved November 18, 2010, from http://www.statcan.gc.ca/pub/82-221-x/82-221-x2006001-eng.htm.
Statistics Canada. (2008). Births. Catalogue no. 84F0210XWE. Retrieved June 13, 2011, from http://www.statcan.gc.ca/pub/84f0210x/84f0210x2008000-eng.pdf.
Statistics Canada. (2010, October 25). Pregnancy outcomes by age group: Canada. Retrieved November 11, 2010, from http://www40.statcan.gc.ca/l01/cst01/hlth65a-eng.htm.
Stier, D. M., Leventhal, J. M., Berg, A. T., Johnson, L., & Mezger, J. (1993). Are children born to young mothers at increased risk of maltreatment? Pediatrics, 91(3), 642–648.
Trocmé, N., Fallon, B., MacLaurin, B., Sinha, V., Black, T., Fast, E. et al. (2010a). Chapter 3: Rates of maltreatment-related investigations in the CIS-1998, CIS-2003, and CIS-2008. In Public Health Agency of Canada, Canadian Incidence Study of Reported Child Abuse and Neglect-2008: Major Findings. Ottawa, 2010.
Trocmé, N., Fallon, B., MacLaurin, B., Sinha, V., Black, T., Fast, E. et al. (2010b). Chapter 5: Characteristics of children and families. In Public Health Agency of Canada, Canadian Incidence Study of Reported Child Abuse and Neglect-2008: Major Findings. Ottawa, 2010.
Trocmé, N., Fallon, B., MacLaurin, B., Sinha, V., Black, T., Fast, E. et al. (2010c). Chapter 1: Introduction. In Public Health Agency of Canada, Canadian Incidence Study of Reported Child Abuse and Neglect-2008: Major Findings. Ottawa, 2010.
Trocmé, N., Fallon, B., MacLaurin, B., Sinha, V., Black, T., Fast, E. et al. (2010 d). Chapter 2: Methodology. In Public Health Agency of Canada, Canadian Incidence Study of Reported Child Abuse and Neglect-2008: Major Findings. Ottawa, 2010.
Walsh, A., & Ollenburger, J. C. (2001). Essential statistics for the social and behavioral sciences. Upper Saddle River, NJ: Prenice-Hall.
Winefield, H. R., & Bradley, P. W. (1992). Substantiation of reported child abuse or neglect: Predictors and implications. Child Abuse & Neglect, 16(5), 661–671.
Wolock, I. (1982). Community characteristics and staff judgments in child abuse and neglect cases. Social Work Research & Abstracts, 18(2), 9–15.
Zuravin, S. J., & DiBlasio, F. A. (1996). The correlates of child physical abuse and neglect by adolescent mothers. Journal of Family Violence, 11(2), 149–166.
Zuravin, S., Orme, J., & Hegar, R. (1995). Disposition of child physical abuse reports: Review of the literature and test of a predictive model. Children and Youth Service Review, 17(4), 559–580.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fallon, B., Ma, J., Black, T. et al. Characteristics of Young Parents Investigated and Opened for Ongoing Services in Child Welfare. Int J Ment Health Addiction 9, 365–381 (2011). https://doi.org/10.1007/s11469-011-9342-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-011-9342-5