
Abstract
Child sexual abuse (CSA) lead to short-term sequelae and long-lasting pervasive outcomes. Research has started addressing CSA as a potential risk factor for later addictions, including pathological gambling. Among Aboriginal peoples, it is plausible that the legacy of residential schooling and other historical traumas have led to unresolved grief that contribute to social problems, such as pathological gambling. The purpose of this brief paper is to report on the few available studies examining the connection between CSA and later pathological gambling. Results show that gambling is more prevalent among Aboriginal than non-Aboriginal populations. Although no causal relationship has been confirmed, experiences of CSA may be related to the later development of pathological gambling among the general population as well as among Aboriginal peoples. However, this link appears complex and indirect and future researches are highly needed. Recommendations based on the implications of this link are proposed for prevention, treatment, and research.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recently, the Prime Minister of Canada made a statement of apology in the name of the Canadian population to all former students of the Residential Schools, acknowledging the harm and injustices caused to them by these schools, which were developed to assimilate Aboriginal children (Truth and Reconciliation Commission 2008). The Indian Residential Schools Truth and Reconciliation Commission was created to document the residential schools legacy and to start a healing process and reconciliation movement embedded in mutual recognition and respect between Aboriginal and non-Aboriginal Canadians.
Many Aboriginal children sent to the residential schools system suffered from childhood maltreatment. Approximately 20% of Aboriginal peoples have been sent to residential schools, and among them, 32.6% reported sexual abuse (RHS National Team 2007b). According to Abadian (1999), the social and political violence inflicted to children, their families and their communities through the residential school system has led to the development of patterns of violence and other behaviours that impede their collective recovery. Residential school legacy and other traumas, including suffering many losses across generations (e.g., losses of family members through alcohol-related accidents, homicides, and suicide) have been responsible for a history of unresolved grief. The impact of these traumas across generations may explain the roots of the current social pathology among Aboriginal communities (Brave Heart and De Bruyn 1998). For example, historical loss is strongly associated with alcohol abuse among Aboriginal Americans (Whitbeck et al. 2004).
One of these traumas, child sexual abuse (CSA), is a significant risk factor that contributes to the development of a host of negative adult outcomes (Brown and Finkelhor 1986; Jumper 1995; Neumann et al. 1996; Polusny and Follette 1995). According to Jacobs (2008), early childhood experiences are a major causal factor of addictions. Research has started addressing the link between CSA experienced by Aboriginal peoples and current addictions. More precisely, a history of sexual abuse has been related to the subsequent development of pathological gambling (Boughton and Falenchuk 2007; Kausch et al. 2006). Thus, addictions, such as pathological gambling and substance abuse, may serve as a means of coping with the suffering of past CSA. The present paper proposes that a history of CSA may contribute to the development of later pathological gambling among Aboriginal peoples. More specifically, it reviews the studies available on gambling among Canadian Aboriginal communities to acknowledge the scope of this problem, and then explores the link between sexual abuse and gambling. Furthermore, it proposes recommendations for prevention, treatment, and future directions for research.
Prevalence of Gambling
Gambling has been a part of human history across cultures and societies (Abbott and Volberg 1999; Belanger et al. 2006; Walker 1992), thereby including Aboriginal cultures as well (Gabriel 1996; Williams et al. 2005). In Aboriginal communities, the earliest evidence of gambling dates 1,000 years before Europeans first arrived in North America. Many games of chance were played at the time, such as the bone, stick or hand games, in which guessing correctly would lead to winning. These games were usually played recreationally and ceremonially, i.e. to please the spirits in order to receive otherwise uncontrollable benefices, such as rain, fertility, or healing (Culin 1973; Williams et al. 2005). During the past 15 years, western style casinos were introduced to Aboriginal communities in hopes of economic renewal. As such, ceremonial gambling was replaced by commercial gambling and traditional forms of gambling were replaced by western forms (Williams et al. 2005).
The occurrence of gambling behaviours has increased worldwide during this century, including in Aboriginal communities (First Nations Inuit and Aboriginal Health Branch 1998; National Council of Welfare 1996), because of its higher accessibility, acceptability, and legalisation (Abbott and Volberg 1999; Cox et al. 2005; Ladouceur et al. 1999; Shaffer et al. 1999; Volberg 1994). In general, people enjoy gambling as it may be their way of daydreaming, relaxing or socializing. However, for some individuals, gambling may become an addiction of varying severity and duration, which is then referred to as “pathological gambling” (Abbott and Volberg 1999; Ladouceur 2000, 2004). Pathological gambling is a psychiatric diagnosis classified in the impulse and control disorders of the DSM-IV-TR (American Psychiatric Association [APA] 2000). An individual is considered to have a pathological gambling disorder when he presents persistent and recurrent maladaptive gambling behaviours (which must be expressed by 5 or more indicators such as being preoccupied with gambling, lying to cover the extent of gambling, failure to control or stop gambling). Pathological gambling is a serious problem which can lead to various consequences for individuals, their families and communities (Wardman et al. 2001). It has been associated with concurrent problems, such as other addictive behaviours and mental health problems like depression and anxiety (Abbott and Volberg 1999; Shaffer and Korn 2002), which renders the profile of the pathological gambler more complex.
Although gambling has been longstanding in many regions of the world, systematic investigation of the prevalence of pathological gambling is more recent. Most studies worldwide have used a psychometric tool, the South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987), to evaluate prevalence rates. According to this instrument, two types of individuals with gambling issues are identified: likely pathological gamblers and problem gamblers, i.e., who have problems with gambling but not pathologically. Therefore, prevalence is also frequently reported as a combination of probable pathological gamblers and problem gamblers. Internationally, combined rates of both types of gambling issues vary between 0.6 and 6.6% (Abbott and Volberg 1999; Cox et al. 2005; Dickerson et al. 1997; Philippe and Vallerand 2007; Shaffer et al. 1999; Shaffer and Hall 2001; Smith and Wynne 2002; Wardman et al. 2001; Wynne 2002). Results of a meta-analysis of a large sample of North American adults (including 66 studies) indicate a mean current probable pathological gambling rate of 1.46% (0.92–2.01 CI), and a mean current problem rate of 2.54% (1.72–3.37) (Shaffer and Hall 2001). Pathological gambling is significantly more prevalent among males, youth, less educated people, individuals with other mental health issues, and ethnic minorities (Lesieur and Rosenthal 1995; Petry 2005; Shaffer et al. 1999; Shaffer and Korn 2002; Westermeyer et al. 2005; Volberg 1994). Wardman et al. (2001) found that Aboriginal peoples were 4 to 16 times more likely to develop pathological gambling than individuals of the general population, and 2 to 5 times more likely to develop gambling problems based on a literature review of 5 North American studies. Other studies have replicated these high prevalence rates of pathological gambling among Aboriginal peoples in United states (Polzin et al. 1998; Volberg 2001; Westermeyer et al. 2005), Australia (Young et al. 2007) and New Zealand (Volberg and Abbott 1997), indicating combined prevalence rates of pathological and problem gambling varying between 2 and 29%.
In Canada, the First Nations Regional Longitudinal Health Survey began investigating this question in 2002/03 (phase 1 of the survey), when some provinces (Manitoba and Quebec) included specific questions about gambling, although no data were collected regarding prevalence of pathological gambling. All of Canada is including these questions in phase 2, which is currently underway (RHS National Team 2007a, b; Reading et al. 2000). Although the existing evidence suggests that the scope of problematic gambling among Aboriginal peoples is large, there is presently an absence of broad-based prevalence studies researching this issue among Aboriginal communities in Canada.
In Canada, all ten provinces have estimated the prevalence of gambling problems, although only two report specific rates for Aboriginal peoples, Alberta (Smith and Wynne 2002) and Saskatchewan (Wynne 2002). Both studies used the Canadian Problem Gambling Index (CPGI, Ferris and Wynne 2001), a public health oriented instrument whose highest rating category is problem gamblers, which roughly corresponds to the probable pathological gambling category of the SOGS. Results of these two studies indicate rates of problem gambling for Aboriginal peoples of 9.6 and 12%, and rates of moderate risk for developing gambling problems of 7.7 and 12% respectively (Smith and Wynne 2002; Wynne 2002). The corresponding rates for the general population in both studies are 1.3 and 1.2% and 3.9 and 4.7% respectively (Smith and Wynne 2002; Wynne 2002).
Other prevalence studies have specifically targeted Aboriginal peoples living on and/or off reserves in Canada. Within Canadian Aboriginal communities, the prevalence of gambling problems, according to the CPGI, or probable pathological gambling, according to SOGS, varies between 5.2 and 19.3%. Problem gamblers (SOGS) and moderate risk gamblers (CPGI) are reported to be prevalent at rates ranging from 7 to 24.7%. The combined rates therefore vary between 16.2% and 44% (Auger and Hewitt 2000; Wynne and McCready 2005a, b). The combined rates approximate the findings of a community-based study conducted in Northwestern Ontario (n = 192), in which 45% of the participants identified themselves as problem gamblers (Oakes and Currie 2004). Furthermore, in a reserve of Southern Alberta, the blood tribe survey (n = 90) results, which are based on the CPGI, indicate that just over 20% are problem gamblers and roughly 30% are at moderate risk of being so, estimating that over half of the population has some issues with gambling (Williams et al. 2005). Recent research with a convenience sample found that almost three quarters of the volunteered respondents were problem gamblers (CPGI) (Currie and Stevens 2007). Nevertheless, problem gambling does not seem to affect the population randomly. Through a participatory action study in Ontario, four out of five communities surveyed reported that over 60% of problem gamblers are female (Wynne and McCready 2005a, b). Similar results were found among Aboriginal Americans in North Dakota in the United States, where women were more likely to develop gambling problems (Cozzetto and Larocque 1996); unlike in the non-Aboriginal population, where gambling is significantly more prevalent among males (e.g., Volberg 1994).
Several factors might explain these higher prevalence rates, including non-cultural risk factors, such as poverty and younger age (Petry 2005; Shaffer and Korn 2002). Actually, low education, poverty, young age, greater exposure to gambling, higher rates of unemployment, addictions, depression, and stress, grief over the loss of a loved one, and preference for and access to continuous forms of gambling such as bingo (Hewitt 1994, 1995; Hewitt and Auger 1995; Moore and Jadlos 2002; Volberg 2001; Volberg and Abbott 1997; Wardman et al. 2001; Zitzow 1996a, b) are all non-cultural risk factors that have been found to be more highly prevalent among Aboriginal communities than in the general population. According to some researchers, other risk factors among some Aboriginal communities would include sensation-seeking behaviour, gambling activity preferences, lack of recreational opportunities, and historical trauma (Wardman et al. 2001; Zitzow 1996b). However, recent research shows no significant differences in gambling behaviour between Aboriginal Americans and non-Aboriginal Americans on sensation-seeking indices, payback percentages of slot machines, and sensibility to the actions and/or ethnicity of a confederate. Therefore, differences in prevalence rates may not be caused by genetic predispositions of Aboriginal peoples but rather to external factors (Gillis et al. 2008; McDougall et al. 2007).
According to Raylu and Oei (2004), cultural variables, such as values and beliefs, help-seeking attitudes, and effects of acculturation, might influence rates of pathological gambling among certain cultural groups, including Aboriginal peoples.
Although Western values and beliefs, such as individualism and fate control, are said to promote gambling behaviours through the promotion of economic success (Anjoul 2003 in Walker et al. 2008) and of individual’s power over their future (Hobbs 2007), values and beliefs concerning mental health may set different standards for gambling problem identification (Cauce et al. 2002; Zangeneh et al. 2004). Considering the extended existence of gambling in Aboriginal communities, social norms about gambling behaviours may render the identification of at-risk and problem gamblers more difficult in some communities, therefore increasing the chances of having higher rates of pathological gambling.
Consequently, Aboriginal peoples’ help-seeking attitudes are affected by problem identification, but also by cultural and historical factors. As such, although they frequently receive services from Western resources and traditional healers for addictions (Beals et al. 2006) or trauma-induced problems (Evans-Campbell et al. 2006), factors such as value conflict, the legacy of colonialism, language barriers, and concerns about confidentiality at times prevent the use of mainstream services (De Coteau et al. 2006; Hamby 2008). These barriers hindering the use of services may therefore impact the prevalence of gambling problems among Aboriginal communities as they go untreated.
Finally, acculturation to Western culture is seen as potentially affecting gambling problems in minority groups with different cultural codes. Although no study has researched this association among Aboriginal peoples, some studies have explored if low or high acculturation to Western culture is related to more gambling problems among immigrants (Chui 2008; Ellenbogen et al. 2007). However, as the results are not consistent across gender, age and ethnic groups, no firm conclusion as to if and how acculturation affects gambling behaviours can be drawn.
In brief, although there are a certain number of studies reporting elevated rates of problem and/or pathological gambling among Aboriginal communities, the lack of validation for either of the two main instruments used (SOGS & CPGI), in addition to small sample sizes limit the confidence in and generalizability of the results. However, these numbers still point to variability in the prevalence rate of gambling problems, and to exceptionally high prevalence in some specific communities. Cultural as well as non-cultural factors might all explain these higher prevalence rates.
Sexual Abuse and Pathological Gambling
Empirical reviews have demonstrated that CSA can produce numerous short-term effects (Kendall-Tackett et al. 1993; Putnam 2003) as well as long-term intense and pervasive consequences that can persist throughout the victims’ life course (Brown and Finkelhor 1986; Jumper 1995; Neumann et al. 1996; Polusny and Follette 1995). Moreover, the long-term effect of CSA on mental health problems might be stronger than those for child physical abuse, even following adjustment for confounding covariates (Fergusson et al. 2008). Results of several studies have focused on drug and alcohol addictions and mental health issues as correlates or consequences of traumatic life events (Scherrer et al. 2007). In Aboriginal communities, CSA is also an important predictor of the utilisation of mental health and addiction treatment services (Robin et al. 1997). Compared to Canadian women, Aboriginal women show significantly higher levels of mental health problems following CSA (Barker-Collo 1999). CSA is prevailing in the general population as well as in Aboriginal communities (Collin-Vézina et al. 2009; Muckle and Dion 2008), yet very little is known about its relationship with pathological gambling.
CSA may lead to long-term sequelae through emotional (experiential) avoidance, which is a symptom of post traumatic stress disorder (PTSD) (Polusny and Follette 1995).
Experiential avoidance is the phenomenon that occurs when a person is unwilling to remain in contact with particular private experiences (e.g., bodily sensations, emotions, thoughts, memories, behavioral predispositions) and takes steps to alter the form or frequency of these events and the contexts that occasion them […]. The immediate effects of experiential avoidance are often positive, and short-term consequences are much more important than long-term ones […]. Thus, experiential avoidance appears to work, even when it does not. (Hayes et al. 1996, p. 1154 and 1156).
According to Polusny and Follette (1995), addictive behaviours may be used to avoid CSA memories or affective responses characteristic of PTSD among victims. However, experiential avoidance is negatively reinforced because it provides short-term relief from negative internal experiences. In the General Theory of Addiction developed by Jacobs (1986, 1989, 2008), the predisposing causes of addictions include a biological state, i.e., an abnormal resting arousal state, as well as a psychological state that may be developed following serious childhood traumatic experiences. Gambling may represent the “escape vehicle” chosen by the addicted person to transform stressors into a rewarding experience or into a dissociative-like state of consciousness.
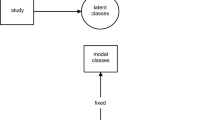
Thus, sexual abuse may be a distal stressor increasing the likelihood of developing maladaptive coping strategies in order to avoid unpleasant abuse-traumatic memories. For such individuals, these strategies may in turn lead to the development of behavioral problems (Freeman and Morris 2001), such as pathological gambling. Pathological gambling may then serve as a learned defence for unresolved trauma-related anxiety (Henry 1996), a mechanism used to escape or dissociate, and to relieve the stress caused by childhood traumatic experiences (Jacobs 2008). Gambling thus can become a high-interest distracter from negative affect (in the present paper, negative abuse-related internal experiences). Fig. 1 presents a conceptual model summarizing the possible connection between CSA and pathological gambling.

Conceptual model of the connection between CSA and pathological gambling
Results of the few studies conducted on the link between sexual abuse and gambling among the general population (see Table 1) indicate various rates of sexual abuse among pathological gamblers, ranging from 6 to 56% (Black and Moyer 1998; Boughton and Falenchuk 2007; Jacobs 2008; Kaplan and Davis 1997; Kausch et al. 2006; Moore and Jadlos 2002; Scherrer et al. 2007). Other studies, that did not distinguish physical, sexual and/or emotional abuse, also report rates of abuse among pathological gamblers, ranging between 16 and 82% (Ciarrocchi and Richardson 1989; Henry 1996; Specker et al. 1996).
Sexual abuse is significantly more prevalent among women within the general population (Putnam 2003), as well as within the gambling population (Ciarrocchi and Richardson 1989; Kaplan and Davis 1997; Kausch et al. 2006; Moore and Jadlos 2002; Petry and Steinberg 2005). Among gamblers, rates of CSA among females range between 22 and 56% (median = 47%) (Boughton and Falenchuk 2007; Jacobs 2008; Kaplan and Davis 1997; Kausch et al. 2006; Moore and Jadlos 2002) and between 6 and 45% (median = 11%) for males (Jacobs 2008; Kaplan and Davis 1997; Kausch et al. 2006; Moore and Jadlos 2002; Scherrer et al. 2007). Considering that sexual abuse prevalence in the general population is about 13 to 22% for women and 4 to 10% for men (Gorey and Leslie 1997; Macmillan et al. 1997; Hébert et al. in press; Tourigny et al. 2006), it appears to be more prevalent in the problem gambler population.
Two studies included a control group and their results indicate that sexual abuse is more prevalent in pathological gamblers in a sample of males who served in Vietnam (n = 1,675) (16.0% vs 6.3%, Scherrer et al. 2007) and in a sample of pathological gamblers in outpatient treatment (n = 40) compared to controls from the general population with no addiction (n = 64) (32.5% vs 0%, Specker et al. 1996). However, sexual abuse was not found to be more prevalent among gambler twins compared to their co-twins (n = 83 pairs) not affected by gambling (Scherrer et al. 2007). Results of the Kaplan and Davis study (1997), conducted in an addiction treatment center in Manitoba, indicate that females are more likely to report a history of sexual abuse than males. More specifically, 22.3% of the females with gambling problems, 41.9% of those with chemical problems and 49.1% of those with dual problems reported having been sexually abused. However, a control group composed of participants with no gambling or chemical problems was not included.
Only one study evaluated the severity of maltreatment. Results indicate that childhood maltreatment (sexual abuse comprised) is significantly associated with gambling onset, severity and frequency (Petry and Steinberg 2005). Moreover, severity of childhood maltreatment is negatively related to the age of onset of gambling and is positively related to gambling severity and frequency. These results suggest the importance of not only assessing the presence of sexual abuse and gambling problems, but also the severity of the abuse when examining the relationship between sexual abuse and gambling.
No research to date has clearly studied mediating factors between CSA and pathological gambling. Among the studies reviewed here on CSA and gambling, some results may perhaps suggest that experiential avoidance (Polusny & Follette’s theory of CSA correlates) and dissociative process (Jacobs’ theory of addiction) play a role in pathological gambling. For example, some results indicate that stress relief (53%) and escape (49%) may lead to gambling (Boughton and Falenchuk 2007). Moreover, high prevalence rates of dissociation (Jacobs 2008; Moore and Jadlos 2002) and PTSD (12.5%) (Specker et al. 1996) are found among gamblers. However, these variables have not been analysed in relation to CSA. Future research is needed to study mediating factors between CSA and pathological gambling, as well as to improve and/or validate the conceptual model presented in Fig. 1.
Results of a qualitative study conducted in Ontario among 192 members of the First Nations indicate that some participants gamble to numb painful feelings and thoughts (some related to past sexual abuse) (Oakes and Currie 2004). Only two studies have quantitatively investigated the link between gambling and sexual abuse among Canadian Aboriginal communities (see Table 1). Hewitt and Auger (1995) conducted a study on youth gambling among 961 Aboriginal students ranging from Grades 5 through 12 (mean age = 14). Results of their study indicate that almost 20% of participants had experienced some forms of sexual abuse. No significant differences were found among the different types of gamblers on rates of different forms of sexual abuse (exhibitionism, fondling of private parts, intercourse). However, prevalence of more severe sexual abuse (i.e., forced masturbation, raped, sexual intercourse, oral and anal sex) increased with gambling problem severity (9% of the non-gamblers vs 16% of the problem gamblers). Overall, girls were about two times at higher risk than boys for CSA, but no analyses were done to differentiate between gambling severity and gender. Again, no analyses examined the link between possible mediating factors and CSA. Nonetheless, 25% of adolescents reported that they gamble in order to forget their problems (Hewitt and Auger 1995). The Jacobs Neglect and Abuse Protocol, which asks about the incidence of 4 types of trauma: neglect, physical, emotional and sexual abuse, was used in a sample of 15 adult First Nations pathological gamblers (median age = 54 years; Jacobs 2008). Childhood trauma was reported among 88% of the pathological gamblers. Overall, 75% of women reported CSA, compared with 43% of the men (Jacobs 2008).
Limitations of the studies conducted on pathological gambling and sexual abuse preclude firm conclusions about this higher prevalence. Some studies did not specifically investigate sexual abuse, as it was included in the general category of historical trauma or combined with physical and/or emotional abuse (e.g., Ciarrocchi and Richardson 1989; Taber et al. 1987). The majority of the studies did not include a comparison group (e.g., Boughton and Falenchuk 2007). Small (e.g., Black and Moyer 1998), non-random (e.g., Boughton and Falenchuk 2007) and clinical samples, such as gamblers in treatment (e.g., Kausch et al. 2006) were the rule rather than the exception. Apart from these limitations, findings from these studies suggest that a history of sexual abuse may contribute to the subsequent development of pathological gambling, and that this association is more prevalent among women than men and among adults than youths. However, it is important to note that no causal factor can be established between sexual abuse and pathological gambling. Among Aboriginal youths, CSA is not related to gambling, yet severe forms of sexual abuse may be related to gambling severity, as found in Petry and Steinberg’s study (2005). In particular, it is not known if CSA is related to pathological gambling among Aboriginal female youths. On the other hand, CSA is highly related to pathological gambling among Aboriginal adults, and more so among females. Overall, the studies on the relationship between sexual abuse and gambling yield mixed results. The highest quality studies indicate that maltreatment may not be as predictive as more proximal measures (e.g., Scherrer et al. 2007), such as the differences among sexual abuse survivors. Thus, more proximal measures, like experiential avoidance, should be considered as mediating the link between sexual abuse and pathological gambling.
In light of these results, the relationship between sexual abuse and pathological gambling among Aboriginal peoples should be examined as well as how it differs from non-Aboriginal populations. In addition, the elevated estimated prevalence rates of sexual abuse in Aboriginal communities, which varies between 25 and 50% (Collin-Vézina et al. 2009), may lead to a higher prevalence of pathological gambling. The link between sexual abuse and pathological gambling may also reflect several issues that prevail in Aboriginal communities. Thus, future research should include youths, women and longitudinal designs for a better understanding of how sexual abuse may lead to the development of pathological gambling. Researchers, clinicians and Aboriginal communities should focus on developing better strategies to understand the link between sexual abuse and gambling in Aboriginal communities.
Clinical Implications
The empirical literature on sexual abuse as a potential risk factor for pathological gambling is quite limited. Nonetheless, some implications on the treatment of pathological gambling among Aboriginal peoples may be considered. Considering that CSA is reported among a quarter to half of Aboriginal adults (Collin-Vézina et al. 2009) and that it is a potential risk factor for pathological gambling, professionals should assess and address trauma experiences when evaluating and treating gamblers. If gambling is used to cope or to escape from the suffering of CSA, neglecting it may result in relapse or other problems. Moreover, sequential or concurrent co-morbid treatment models may help the recovery of pathological gamblers, as these individuals often present a complex profile that can affect access, retention and treatment outcome (Winters and Kushner 2003).
As Auger and Hewitt (2000) recommend, treatment should focus on the whole individual, not solely on the problematic gambling behaviours. In Aboriginal communities, therapeutic models are recommended to include not only the individual, but also the family and the community, in an ecological approach integrating cultural values (Muckle and Dion 2008). This can be accomplished through awareness of the realities of the Aboriginal communities, including the impact of the historical traumas, such as the residential school legacy and colonization (Morency and Kistabish 2001). As gambling is rising worldwide, prevention and education should be emphasised not only in the general population but among sexual abuse victims as well as among Aboriginal Communities. If pathological gambling is, in adulthood, a correlate of CSA, prevention strategies should also target youths, as they are at higher risk of pathological gambling (Petry 2005).
Conclusion
Compared to the general population, pathological gambling appears to be more prevalent among Aboriginal peoples in Canada as well as in other countries. Knowing risk factors leading to pathological gambling may lead to a better understanding of this problem as well as better prevention and treatment programs. In the current literature review, CSA as a risk factor for pathological gambling was explored. Despite methodological limitations, research results indicate that CSA is related to pathological gambling among the general population. However, this association clearly needs further investigation among Aboriginal peoples from Canada, as the only two studies that have been conducted thus far have found mixed results. As CSA is highly prevalent in a number of Aboriginal communities, a better understanding of its role in the complex picture of pathological gambling would be beneficial. Ultimately, researchers, professionals, and communities need to join their efforts in fertile research and initiatives to enrich practices on preventing and treating pathological gamblers using a sound cultural approach that leads to healing not only the individual, but the community as a whole.
References
Abadian, S. (1999). From wasteland to homeland: Trauma and the renewal of indigenous peoples and their communities. Unpublished Ph.D. Dissertation. Harvard University, Cambridge, MA.
Abbott, M. W., & Volberg, R. A. (1999). Gambling and problem gambling in the community: An international overview and critique. Wellington: Department of Internal Affairs.
American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (DSM-IV-TR). Washington: Author.
Auger, D., & Hewitt, D. (2000). Dream chaser: Alberta Aboriginal adult gambling prevalence study. Edmonton: Nechi Training, Research, & Health Promotions Insitute.
Barker-Collo, S. L. (1999). Reported symptomatology of Native Canadian and Caucasian females sexually abused in childhood: a comparison. Journal of Interpersonal Violence, 14, 747–760.
Beals, J., Novins, D. K., Spicer, P., Whitesell, N. R., Mitchell, C. M., & Manson, S. M. (2006). Help seeking for substance use problems in two American Indian reservation populations. Psychiatric Services, 57, 512–520.
Belanger, Y., Williams, R., Chief, P. D., & Shade, C. (2006). Aboriginal casinos: Who’s cashing in? Retrieved January 15, 2009, from http://www.rsc.ca/index.php?page=forums_aboriginal_casions&lang_id=1&page_id=207.
Bernstein, D. P., Ahluvalia, T., Pogge, D., & Handelsman, L. (1997). Validity of the childhood trauma questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 340–348.
Black, D. W., & Moyer, T. (1998). Clinical features and psychiatric comorbidity of subjects with pathological gambling behavior. Psychiatric Services, 49, 1434–1439.
Boughton, R., & Falenchuk, O. (2007). Vulnerability and comorbidity factors of female problem gambling. Journal of Gambling Studies, 23, 323–334.
Brave Heart, M. Y. H., & De Bruyn, L. (1998). The American holocaust: historical unresolved grief among native American Indians. National Center for American Indian and Alaska Native Mental Health Research Journal, 8, 56–78.
Brown, A., & Finkelhor, D. (1986). Impact of child sexual abuse: a review of the research. Psychological Bulletin, 99, 66–77.
Cauce, A. M., Domenech-Rodriguez, M., Paradise, M., Cochran, B. N., Shea, J. M., Srebnik, D., et al. (2002). Cultural and contextual influences in mental health help seeking: a focus on ethnic minority youth. Journal of Consulting and Clinical Psychology, 70, 44–55.
Christenson, G. A., Faber, R. J., & deZwaan, M. (1994). Compulsive buying: descriptive characteristics and psychiatric comorbidity. Journal of Clinical Psychiatry, 55, 5–11.
Chui, W. H. (2008). True stories: migrant Vietnamese women with problem gambling in Brisbane, Queensland. Journal of Social Work Practice in the Addictions, 8, 276–280.
Ciarrocchi, J., & Richardson, R. (1989). Profile of compulsive gamblers in treatment: update and comparisons. Journal of Gambling Behavior, 5, 53–65.
Collin-Vézina, D., Dion, J., & Trocmé, N. (2009). Sexual abuse in Canadian Aboriginal communities: a broad review of conflicting evidence. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health, 7, 27–47. Retrieved July 24, 2009, from http://www.pimatisiwin.com/online/?page_id=593.
Cox, B. J., Yu, N., Olfrey, T., & Ladouceur, R. (2005). A national survey of gambling problems in Canada. Canadian Journal of Psychiatry, 50, 213–217.
Cozzetto, D. A., & Larocque, B. W. (1996). Compulsive gambling in the Indian community: a North Dakota case study. American Indian Culture and Research Journal, 20, 73–86.
Culin, S. (1973). Games of the North American Indians. New York: AMS.
Currie, C., & Stevens, R. (2007). Gambling research reveals: the placement of casinos in Alberta’s Aboriginal communities: an interview with Cheryl Currie. Alberta Gaming Research Institute Newsletter, 7, 1–4.
De Coteau, T., Anderson, J., & Hope, D. (2006). Adapting manualized treatments: treating anxiety disorders among Native Americans. Cognitive and Behavioral Practice, 13, 304–309.
Dickerson, M., McMillen, J., Hallebone, E., Volberg, R., & Woolley, R. (1997). Definition and incidence of problem gambling, including the socio-economic distribution of gamblers. Melbourne: Victorian Casino and Gaming Authority.
Ellenbogen, S., Gupta, R., & Derevensky, J. L. (2007). A cross-cultural study of gambling behaviour among adolescents. Journal of Gambling Studies, 23, 25–39.
Evans-Campbell, T., Lindhorst, T., Huang, B., & Walters, K. L. (2006). Interpersonal violence in the lives of urban American Indian and Alaska Native women: implications for health, mental health, and help-seeking. American Journal of Public Health, 96, 1416–1422.
Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2008). Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abuse & Neglect, 32, 607–619.
Ferris, J., & Wynne, H. (2001). The Canadian problem gambling index: Final report. Ottawa: Canadian Center on Substance Abuse.
First Nations Inuit, & Aboriginal Health Branch. (1998). National Native alcohol and drug abuse program (NNADAP)—general review 1998—final report. Ottawa: Health Canada.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996). Structured Clinical Interview for DSM-IV Axis I Disorders: Clinician Version (SCID-CV). Washington: American Psychiatric Association.
Freeman, K. A., & Morris, T. L. (2001). A review of conceptual models explaining the effects of child sexual abuse. Aggression and Violent Behaviour, 6, 357–373.
Gabriel, K. (1996). Gambler way: Indian gaming in mythology, history, and archaeology in North America. Boulder: Johnson Books.
Gorey, K. M., & Leslie, D. R. (1997). The prevalence of child sexual abuse: integrative review adjustment for potential response and measurement biases. Child Abuse & Neglect, 21, 391–398.
Gillis, A., McDonald, J., & Weatherly, J. N. (2008). American Indians and non-Indians playing a slot-machine simulation: effects of sensation seeking and payback percentage. American Indian and Alaska Native Mental Health Research, 15, 18–32.
Hamby, S. (2008). The path of helpseeking: perceptions of law enforcement among American Indian victims of sexual assault. Journal of Prevention & Intervention in the Community, 36, 89–104.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996). Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64, 1152–1168.
Hébert, M., Tourigny, M., Cyr, M., McDuff, P., & Joly, J. (in press). Prevalence of childhood sexual abuse and timing of disclosure in a representative sample of adults from the province of Quebec. Canadian Journal of Psychiatry.
Henry, S. L. (1996). Pathological gambling: etiologic considerations and treatment efficacy of eye movement desensitization/reprocessing. Journal of Gambling Studies, 12, 395–405.
Hewitt, D. (1994). Spirit of bingoland: A study of problem gambling among Alberta Native people. Edmonton: Nechi Training, Research, & Health Promotions Institute.
Hewitt, D. (1995). Spirit of bingoland: Problem gambling in two Ontario First Nation communities: Chippewas of Mnjikaning (Rama) & Chippewas of Sarnia. Edmonton: Nechi Training, Research, & Health Promotions Institute.
Hewitt, D., & Auger, D. (1995). Firewatch on Aboriginal adolescent gambling. Edmonton: Nechi Training, Research, & Health Promotions Institute.
Hobbs, M. C. (2007). Culturally-derived values and beliefs as correlates of risk for problem gambling. Unpublished doctoral dissertation, University of Windsor, Ontario.
Jacobs, D. F. (1986). A general theory of addictions: a new theoretical model. Journal of Gambling Behavior, 2, 15–31.
Jacobs, D. F. (1989). A general theory of addictions: Rationale for and evidence supporting a new approach for understanding and treating addictive behaviors. In H. Shaffer, S. Stein, B. Gambino & T. Cummings (Eds.), Compulsive gambling: Theory, research, and practice (pp. 35–64). Lexington: Lexington Books.
Jacobs, D. (1999). Jacobs neglect and abuse protocol. Loma Linda: author.
Jacobs, D. (2002). Jacobs neglect, abandonment, and abuse protocol. Loma Linda: author.
Jacobs, D. F. (2008). Growth of Aboriginal casinos in North America: Future prospects. Paper presented at the Responsible Gambling Council Discovery 2008 Conference.
Jumper, S. A. (1995). A meta-analysis of the relationship of child sexual abuse to adult psychological adjustment. Child Abuse & Neglect, 19, 715–728.
Kaplan, G., & Davis, B. (1997). Gambling, alcohol & others drugs. Prevalence & implications of dual problem clients. Manitoba: Addictions foundation of Manitoba.
Kausch, O., Rugle, L., & Rowland, D. Y. (2006). Lifetime histories of trauma among pathological gamblers. The American Journal on Addictions, 15, 35–43.
Kendall-Tackett, K. A., Meyer William, L., & Finkelhor, D. (1993). Impact of sexual abuse on children: a review and synthesis of recent empirical studies. Psychological Bulletin, 113, 164–180.
Kessler, R. C., Sonnega, A., Evelyn, B., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the national comorbidity survey. Archives of General Psychiatry, 52, 1048–1060.
Ladouceur, R. (2000). Le Jeu excessif : Comprendre et vaincre le gambling. Montreal: Éditions de l’Homme.
Ladouceur, R. (2004). Gambling: the hidden addiction. Canadian Journal of Psychiatry, 49, 501–503.
Ladouceur, R., Jacques, C., Ferland, F., & Giroux, I. (1999). Prevalence of problem gambling: a replication study 7 years later. Canadian Journal of Psychiatry, 44, 802–804.
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144, 1184–1188.
Lesieur, H. R., & Rosenthal, R. J. (1995). Gambler’s Self-Report Inventory (GSRI). Unpublished assessment instrument.
MacMillan, H. L., Fleming, J. E., Trocmé, N., Boyle, M. H., Wong, M., Racine, Y. A., et al. (1997). Prevalence of child physical and sexual abuse in the community: results from the Ontario health supplement. Journal of the American Medical Association, 278, 131–135.
McDougall, C. L., McDonald, J., & Weatherly, J. N. (2007). The gambling behavior of American Indian and non-Indian participants: effects of the actions and ethnicity of a confederate. American Indian and Alaska Native Mental Health Research, 14, 59–74.
McLellan, A. T., Kushner, H., Metzger, D., Peters, R., Smith, I., Grissom, G., et al. (1992). The fifth edition of the addiction severity index. Journal of Substance Abuse Treatment, 9, 199–213.
Moore, T. L., & Jadlos, T. (2002). The etiology of pathological gambling: A study to enhance understanding of causal pathways as a step towards improving prevention and treatment. Wilsonville: Oregon Gambling Addiction Treatment Foundation.
Morency, J., & Kistabish, R. (2001). Intervention en milieu autochtone: Comprendre le passé pour mieux agir aujourd’hui. Psychologie Québec, 18, 14–18.
Muckle, F., & Dion, J. (2008). Les facteurs de résilience et de guérison chez les autochtones victimes d’agression sexuelle. Revue Québécoise de Psychologie. Spécial Jeunes et agressions sexuelles : Modalités et évaluation de l’intervention, 29, 59–72.
National Council of Welfare. (1996). Gambling in Canada. Ottawa: National Council of Welfare.
Neumann, D. A., Houskamp, B. H., Pollock, V. E., & Brière, J. (1996). The long-term sequelae of childhood sexual abuse in women: a meta-analytic review. Child Maltreatment, 1, 6–16.
Oakes, J., & Currie, C. (2004). Gambling and problem gambling in First Nations communities. Guelph: Ontario Problem Gambling Research Center.
Petry, N. M. (2005). Pathological gambling: Etiology, comorbidity, and treatment. Washington: American Psychological Association.
Petry, N. M., & Steinberg, K. L. (2005). Childhood maltreatment in male and female treatment-seeking pathological gamblers. Psychology of Addictive Behaviors, 19, 226–229.
Philippe, F. D. R., & Vallerand, R. J. (2007). Prevalence rates of gambling problems in Montreal, Canada: a look at old adults and the role of passion. Journal of Gambling Studies, 23, 275–283.
Polusny, M. A., & Follette, V. M. (1995). Long-term correlates of child sexual abuse: theory and review of the empirical literature. Applied & Preventive Psychology, 4, 143–166.
Polzin, P. E., Baldridge, J., Doyle, D., Sylvester, J. T., Volberg, R. A., & Moore, W. L. (1998). Gambling-Montana style. Montana Business Quarterly, 36, 2–13.
Putnam, F. W. (2003). Ten-year research update review: child sexual abuse. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 269–278.
Raylu, N., & Oei, T. P. (2004). Role of culture in gambling and problem gambling. Clinical Psychology Review, 23, 1087–1114.
Reading, J., Svenson, K., O’Neil, J., Young, K., Elias, B., MacMillan, H., et al. (eds). (2000). First Nations and Inuit regional health survey. St. Regis: First Nations and Inuit Regional Health Survey National Steering Committee.
RHS National Team (Ed). (2007a). First nations regional health survey phase 2—adult questionnaire. Ottawa: First Nations Information Governance Committee.
RHS National Team (Ed). (2007b). First Nations Regional Longitudinal Health Survey (RHS) 2002/03: Results for adults, youth and children living in First Nations communities. Ottawa: First Nations Information Governance Committee.
Robin, R. W., Chester, B., Rasmussen, J. K., Jaranson, J. M., & Goldman, D. (1997). Factors influencing utilization of mental health and substance abuse services by American Indian men and women. Psychiatric Services, 48, 826–832.
Robins, L., Helzer, J., Cottler, L., & Goldring, E. (1988). NIMH Diagnostic Interview Schedule Version III Revised (DIS-III-R). St. Louis: Department of Psychiatry, Washington University School of Medicine.
Scherrer, J. F., Xian, H., Kapp, J. M., Waterman, B., Shah, K. R., Volberg, R., et al. (2007). Association between exposure to childhood and lifetime traumatic events and lifetime pathological gambling in a twin cohort. Journal of Nervous and Mental Disease, 195, 72–78.
Shaffer, H. J., & Hall, M. N. (2001). Updating and refining meta-analytic prevalence estimates of disordered gambling behaviour in the United States and Canada. Canadian Journal of Public Health, 92, 168–172.
Shaffer, H. J., & Korn, D. A. (2002). Gambling and related mental disorders: a public health analysis. Annual Review of Public Health, 23, 171–212.
Shaffer, H. J., Hall, M., & Vander Bilt, J. (1999). Estimating the prevalence of disordered gambling behavior in the United States and Canada: a research synthesis. American Journal of Public Health, 89, 1369–1376.
Smith, G. J., & Wynne, H. (2002). Measuring gambling and problem gambling in Alberta using the Canadian problem gambling index. Edmonton: Alberta Gaming Research Institute.
Specker, S. M., Carlson, G. A., Edmonson, K. M., Johnson, P. E., & Marcotte, M. (1996). Psychopathology in pathological gamblers seeking treatment. Journal of Gambling Studies, 12, 67–81.
Taber, J. I., McCormick, R. A., & Ramirez, L. F. (1987). The prevalence and impact of major life stressors among pathological gamblers. Substance Use & Misuse, 22, 71–79.
Tourigny, M., Gagné, M.-H., Joly, J., & Chartrand, M.-È. (2006). Prévalence et cooccurrence de la violence envers les enfants dans la population québécoise. Canadian Journal of Public Health, 97, 109–113.
Truth and Reconciliation Commission (2008). Indians residential schools. Retrieved January 15, 2009, from http://www.trc-cvr.ca/.
Volberg, R. A. (1994). The prevalence and demographics of pathological gamblers: implications for public health. American Journal of Public Health, 84, 237–241.
Volberg, R. A. (2001). Gambling and problem gambling in North Dakota: A replication study, 1992 to 2002. Northampton: Gemini Research, Ltd.
Volberg, R. A., & Abbott, M. W. (1997). Gambling and problem gambling among indigenous peoples. Substance Use & Misuse, 32, 1525–1538.
Walker, M. (1992). The psychology of gambling. New York: Pergamon.
Walker, M., Schellink, T., & Anjoul, F. (2008). Explaining Why People Gamble. In M. Zangeneh, A. Blaszczynski & N. E. Turner (Eds.), In the pursuit of winning: Problem gambling theory, research and treatment (pp. 11–31). New York: Springer Science and Business Media.
Wardman, D., El-Guebaly, N., & Hodgins, D. (2001). Problem and pathological gambling in North American Aboriginal populations: a review of the empirical literature. Journal of Gambling Studies, 17, 81–100.
Westermeyer, J., Canive, J., Garrard, J., Thuras, P., & Thompson, J. (2005). Lifetime prevalence of pathological gambling among American Indian and Hispanic American veterans. American Journal of Public Health, 95, 860–866.
Whitbeck, L. B., Chen, X., Hoyt, D. R., & Adams, G. W. (2004). Discrimination, historical loss and enculturation: culturally specific risk and resiliency factors for alcohol abuse among American Indians. Journal of Studies on Alcohol, 65, 409–417.
Williams, R., Wynne, H., Nixon, G., & Frank, L. (2005). Using participatory action research to study Canadian Aboriginal gambling. Paper presented at the 6th European Conference on Gambling Studies and Policy Issues. Malmo, Sweden.
Winters, K. C., & Kushner, M. G. (2003). Treatment issues pertaining to pathological gamblers with a comorbid disorder. Journal of Gambling Studies, 19(3), 261–277.
Winters, K., Stinchfield, R., & Fulkerson, J. (1993). Toward the development of an adolescent gambling problem severity scale. Journal of Gambling Studies, 9, 63–84.
Wynne, H. (2002). Gambling and problem gambling in Saskatchewan. Ottawa: Canadian Centre on Substance Abuse.
Wynne, H., & McCready, J. (2005a). Examining gambling and problem gambling in Ontario Aboriginal communities: Final summary report. Guelph: Ontario Problem Gambling Research Centre.
Wynne, H., & McCready, J. (2005b). Examining gambling and problem gambling in Ontario Aboriginal communities: Five community final research reports. Guelph: Ontario Problem Gambling Research Centre.
Young, M., Barnes, T., Stevens, M., Paterson, M., & Morris, M. (2007). The changing landscape of indigenous gambling in Northern Australia: current knowledge and future directions. International Gambling Studies, 7, 327–343.
Zangeneh, M., Sageghi, N., & Littman-Sharp, N. (2004). Perceptions and attitudes about gambling, problem gambling and help-seeking behavior among Iranians in Toronto- A small qualitative study. Shiraz E-Medical Journal, 5.
Zitzow, D. (1996a). Comparative study of problematic gambling behaviors between American Indian and non-Indian adolescents within and near a northern plains reservation. American Indian and Alaska Native Mental Health Research, 7, 14–26.
Zitzow, D. (1996b). Comparative study of problematic gambling behaviors between American Indian and non-Indian adults in a northern plains reservation. American Indian and Alaska Native Mental Health Research, 7, 27–41.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dion, J., Collin-Vézina, D., De La Sablonnière, M. et al. An Exploration of the Connection between Child Sexual Abuse and Gambling in Aboriginal Communities. Int J Ment Health Addiction 8, 174–189 (2010). https://doi.org/10.1007/s11469-009-9234-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-009-9234-0