
Abstract
Gambling has become increasingly popular among minors and is easily accessible to them. This is alarming since research has indicated that minors are more susceptible to gambling pathology than adults. Additionally, gambling has devastating effects on minors that gamble as well as their families and communities. The Illinois Institute for Addiction Recovery (IIAR) developed a gambling awareness prevention program called “Don’t Gamble Away our Future ™” to educate minors about gambling and the dangers associated with it. The IIAR started collecting data for the purpose of evaluation in 2005. The purpose of the current study was to evaluate the program’s effectiveness at changing knowledge about gambling and to assess the frequencies of problem and pathological gambling among participants at program implementation (year one). The program was evaluated with a sample of 8,455 Midwestern youth. Findings indicated that 10% of the participants were probable pathological gamblers and that the program was successful at increasing knowledge of gambling and the negative effects it can have, over the short term. Teaching minors about the risks of gambling and the effects it can have is an important preventative measure that can help protect youth from the dangers associated with problem and pathological gambling.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although gambling is technically illegal for minors, it does not stop them from engaging in gambling activities. Gambling may seem like a harmless activity for youth to become involved in, but research shows that while most youth only gamble occasionally, up to 14% gamble more frequently, to the point of it being a problem (American Psychological Association 1998; Jackson et al. 2008; Jacobs 2000). In fact, problem gambling is one of the biggest issues facing youth today as minors participate in gambling activities more than they do any other addictive behavior (Gupta & Derevensky 1998a). This is alarming for at least three reasons. First, research has shown that minors are at a higher risk for problem gambling than adults (Derevensky and Gupta 2000; Jacobs 2000). Secondly, minors are often introduced to gambling by family members, who portray it as harmless and who often have gambling problems of their own. Finally, gambling among minors has been linked to a number of negative outcomes. The increased risk of gambling pathology and the consequences of it for minors provided sufficient incentive for the development of a preventative gambling program, called “Don't Gamble Away Our Future ™,” which was designed by the Illinois Institute for Addiction Recovery (IIAR). The purpose of the program was to educate minors about gambling, including the dangers affiliated with it. Data has been collected on a yearly basis from the participants in the program since 2005. The current study evaluated the effectiveness of the “Don't Gamble Away Our Future ™” program on students' knowledge about gambling, in its first implementation stage.
Negative Consequences of Gambling for Minors
The bulk of the research regarding gambling among minors has focused almost exclusively on adolescents. The lack of research on younger children is of serious concern because adolescents that have reported problems with gambling often indicate that they started gambling around the age of 10, sometimes even younger (Gupta and Derevensky 1998a; National Research Council [NRC] 1999; Stinchfield 2004). Youth also tend to start gambling before they engage in other risky behaviors like cigarette smoking and substance abuse (Stinchfield 2004). While gambling among children under 12 warrants further attention, the research cited in this manuscript concentrated on adolescent gambling due to its availability.
Gambling among adolescents is quite common. In 1987, Lesieur and Klein surveyed 892 New Jersey high school students about their gambling and found that 91% of the students had gambled at least once and that a third gambled at least once a week. More recently, multiple large-scale self-report studies conducted in the United States, Canada, Australia, Europe, England, and New Zealand have shown high rates of problematic gambling behaviors among adolescents (Derevensky and Gupta 2004a; Stinchfield 2000; Turchi and Derevensky 2006). Approximately 60–80% of adolescents under the age of 17 have admitted to gambling at least once over the previous 12 months (Delfabbro et al. 2005; Jacobs 2000; Turchi and Derevensky 2006), and up to 35% gamble at least once a week (Delfabbro et al. 2005; Gupta and Derevensky 1998a). In regards to gender, male adolescents gamble more often than female adolescents, but they are both engaging in this risky behavior (Jacobs 2000; Stinchfield 2000; Stinchfield et al. 2006).
Perhaps more alarming are the high frequencies of problem and pathological gambling among youth. Research demonstrates that 10–15% of youth are at risk for developing serious problems with gambling and 3–8% evidence serious gambling pathology (Jackson et al. 2008; Jacobs 2000; Turchi and Derevensky 2006), which is defined as “chronic and progressive failure to resist impulses to gamble” (NRC 1999, p. 2). In comparison, the National Council on Problem Gambling (NCPG 2006) reports on their website that around the same proportion (70%) of adults admit that they have gambled at least once over the previous year, but only 2% are classified as pathological gamblers. The increased risk for problematic gambling among adolescents could be attributed to starting at a very young age, being introduced to gambling activities by family members, and the developmental vulnerability of adolescents (Gupta and Derevensky 1998a).
The majority of adolescents that gamble first did so with parents and other family members, who portrayed it as an exciting and safe way to have fun (NRC 1999). Gambling is already attractive to adolescents because they perceive it as an adult activity, similar to smoking or alcohol use. When parents and siblings promote the activity to adolescents as fun and harmless, it increases the likelihood that adolescents will partake in gambling activities (Problem Gambling Foundation of New Zealand 2008). Unfortunately, parents tend to be in the dark about the age at which gambling starts for youth. For example, Ladouceur et al. (1999) interviewed 279 parents in the Quebec, Canada region and found that most of the parents overestimate the age at which most children begin gambling, believing that children are much older when they start to gamble. It may be the case that when parents allow their children to “play” with scratch off tickets or wager on card games, they do not see it as gambling.
Compounding the issue, many of the parents that promote gambling to their children gamble themselves. For instance, Ladouceur et al. (1999) found that 74% of the parents they interviewed gambled themselves more than once a week and Delfabbro et al. (2005) reported that of the 900 Australian youth they surveyed, 72% revealed that their parents gambled. These figures in and of themselves are not alarming, but there is a significant relationship between the frequency of parental gambling and adolescent gambling (Delfabbro et al. 2005). Additionally, having a parent with a gambling problem increases the risk of gambling pathology for the child (Problem Gambling Foundation of New Zealand, 2008). This can result in issues of denial that interfere with problem gambling treatment for adolescents (Fong 2006; Hardoon et al. 2004; Langhinrichsen-Rohling et al. 2004). For instance, Ladouceur et al. (1999) reported that only 5% of the parents interviewed would try to prevent their child from engaging in gambling. At the very least, family members' acceptance of gambling makes it easier for minors to gain access to this seductive activity.
Research has shown that there is a strong correlation between the accessibility of gambling and the prevalence of pathological gambling (Pavalko 2004). Gambling among minors is no longer limited to activities like throwing dice or rolling marbles on the playground; minors can also bet on games of personal skill (e.g., pool or bowling), purchase lottery tickets, wager on card games (e.g., Texas hold 'em), bet on horse, dog, or cock fighting, gamble in arcades, at midway games at the fair, on board games, bingo, and electronic gambling machines (Buchta 1995; Jacobs 2000; Turchi and Derevensky 2006).
The Internet also offers 24-h gambling access and the allure of sophisticated technologies (i.e., real-time audio and visual games and races). Internet gambling is particularly risky for minors because underage gambling is difficult to prevent on-line. Mobile gambling (gambling using a cell phone) has also become popular with adolescents as it is discreet and easy to do (Turchi and Derevensky 2006). The most popular forms of gambling for youth are card games, scratch cards/tickets, and sports pools (Adlaf et al. 2006). The bottom line is, if youth want to gamble, there are many venues available to them. The ease at which adolescents can gamble is troubling since they already face a higher risk for pathological gambling problems (NCPG 2006). Compounding this situation is the fact that children and adolescents are not developmentally advanced enough to understand the potential negative consequences of their gambling behavior.
According to Piaget (Atherton 2005), children do not develop the ability to think critically about issues until they reach the “formal operational stage,” which extends from about the age of 11 into adulthood. It is at this point that some, but not all, children are able to think about issues in an abstract manner. Such abstract thinking includes the ability to foresee the consequences of behavior. Not all children progress into formal operational thinking at the age of 11. Many children do not reach the formal operational stage in cognitive development until their late teens, if at all (Siegler 1991). Although Piaget's theory has been criticized, other research has shown that adolescent brain development is not complete until about the age of 25 (Giedd 2004) and that adolescents are more susceptible to risky behavior (Winters 2008a).
Adding to the developmental liability of youth is the egocentrism and invincibility characteristic of adolescents (Problem Gambling Foundation of New Zealand 2008; Winter 2008a, b). Most adolescents believe that they are immune from the negative consequences associated with risky behavior (Fong 2006). These factors make minors more vulnerable to gambling, particularly when they are brought into it by family members. This is worrisome as young problem gamblers are more likely to hold superstitious beliefs about gambling, like being able to beat the odds of winning, or that betting more money equals a bigger pay out (Moore and Ohtsuka 1999). Even worse, most adolescents are not aware that gambling has a downside (Haubrich-Casperson 1993). But the research is very clear on this issue; gambling has serious negative consequences for individuals, families, schools, and society.
One of the most disturbing consequences of gambling for individuals is the effect it has on their mental health. Adolescent gambling has been found to be associated with major depression, anxiety, attention-deficit/hyperactivity disorder, low self-esteem, and personality disorders (Dickson et al. 2002; Ellenbogen et al. 2007; Fong 2006, Gupta and Derevensky 1998b; Gupta and Derevensky 2000). Research has also demonstrated that adolescent gamblers abuse substances at a rate greater than non-gamblers (Gupta and Derevensky 1998a; Gupta and Derevensky 2000; Jacobs 2000; Ladouceur et al. 1999). Even social gamblers, defined as those that gamble but do not appear to have a problem with gambling, abuse substances (Ellenbogen et al. 2007). Although these issues are serious enough, adolescent pathological gamblers report more frequent suicide ideation and attempts than adolescents who do not gamble (Derevensky and Gupta 2004b; Gupta and Derevensky 1998a; Langhinrichsen-Rohling et al. 2004). It is possible that adolescents view suicide and abusing substances as viable options for coping with the problems associated with gambling. These types of behaviors have negative long-term effects on the physical health and mortality of youth, making gambling even more dangerous for young players.
Gambling also complicates family and peer relationships. Adolescents that gamble spend less time with family members, steal from family members to fund gambling activities, fight more with family members, and experience emotional problems as a result of gambling (Derevensky et al. 2004; Fong 2006; NRC 1999; Problem Gambling Foundation of New Zealand 2006; Westphal et al. 2000). Adolescents sometimes do not have the money to finance a gambling problem, so the entire family may have to suffer a financial loss when parents have to “bail their children” out of financial debt due to gambling (Fong 2006). Peer relationships are not immune from the effects of problem gambling. Friendships can disintegrate when friends of gamblers are replaced with gambling contemporaries (Derevensky et al. 2004; Louisiana Department of Health and Hospitals, n.d.). These findings suggest that gambling diminishes adolescent social networks over time. Without a strong social network, it is far more difficult to end destructive behaviors (Russell et al. 1997). The effects of adolescent gambling are not limited to mental health and relationships, school performance is also impacted.
Gambling can lead to poor grades for young gamblers due to the amount of time dedicated to gambling, which often leaves little time for academic work (Fong 2006). This makes sense as adolescents that gamble report negative views of school, a loss of interest in school activities, more truancy and tardiness, and a tendency to steal from classmates (Derevensky et al. 2004; National Gambling Impact Study Commission 1999; Problem Gambling Foundation of New Zealand 2006; Westphal et al. 2000). These findings are particularly distressing as educational aspirations can serve as buffers against gambling, like they do with other illegal activities, like drug use (Pettit et al. 1997).
The effects of adolescent gambling can also severely impact the community in which they reside due to increases in crime. Adolescent gambling has been linked to theft, burglary, aggressiveness, the possession and sale of illegal drugs, prostitution, and problems with the police (Fong 2006; Jacobs 2000; Problem Gambling Foundation of New Zealand 2008; Westphal et al. 2000). According to the Problem Gambling Foundation of New Zealand (2006), 42.4% of adolescent problem/pathological gamblers indicated that they stole or borrowed money in order to cover their gambling related debts. Regardless of the reasons for the crimes, it is clear from the research that communities are negatively affected by adolescent gambling.
Purpose of the Study
While not all of the youth that engage in gambling will end up problem gamblers, the negative effects of gambling on adolescents are serious enough to warrant attention. Messerlian et al. (2005) presented a Youth Gambling Risk Prevention model that supports a public health intervention approach as part of a prevention effort. Messerlian et al. point out that even though the majority of youth (80%) can be considered “low-risk” gamblers, a large percentage of youth gamble, creating the potential for problems. Furthermore, Messerlain et al. stated that “Primary prevention objectives include increasing knowledge and awareness of the risks and consequences of at-risk gambling for not only the adolescents themselves, but for their parents, professionals, and the general public” (p. 73). Currently there is no streamlined prevention, problem identification, and treatment referral system for minors that engage in gambling. This is troubling given the developmental vulnerability of minors (Siegler 1991; Winters 2008b). It seems imperative that prevention efforts be directed towards youth, parents, school personnel, and the general public to help prevent gambling problems among minors.
In response to this issue, the Illinois Institute for Addiction Recovery (IIAR) at Proctor Hospital in Peoria, Illinois, United States of America, developed a preventative gambling awareness program called “Don't Gamble Away Our Future ™” (funded by the Office of Juvenile Justice and Delinquency Prevention) to educate youth, their families, and school administrative personnel about gambling and the dangers associated with it. The program was designed specifically for children and adolescents ages 8–18 and was first implemented in four school systems in the Midwestern United States in 2005. This evaluation is a preliminary analysis of the program as part of a larger longitudinal evaluation design.
The primary objectives of the prevention program are threefold: a) to disseminate information and raise awareness about gambling, b) to change faulty or problematic beliefs about gambling, and c) to reduce the gambling rates among participants and overall prevalence rates of adolescent gambling in the communities the program serves. The purpose of the current study was to evaluate whether the “Don't Gamble Away Our Future ™” program was successful in meeting the first and second goals of the program: raising awareness and reducing faulty beliefs about gambling. More specifically, did participants improve their knowledge about gambling, the consequences of gambling, and the myths about gambling following program implementation? In addition we looked at whether there were differences in improvement among the four locations (which are described below) or by gender. Finally, the initial prevalence of problem gambling at the first data collection was also assessed and differences by location and gender for problem gambling were analyzed.
Methods
In the first time wave for the longitudinal evaluation design, the “Don't Gamble Away our Future ™” gambling awareness program was administered to a convenience sample of 8,455 students from four Midwestern school settings (i.e., primary schools, junior high schools, high schools, and a juvenile detention center). Pre-tests were administered to participants before the program began and post-tests after the program was completed. The 45-min preventative program consisted of lecture, activities, and discussion. Participants were provided a CD-ROM that contained several interactive components designed to support the program objectives following program completion. Information packets were also given to parents, teachers, and school administrators prior to program implementation.
Procedures
School administrators were contacted and apprised of the issue of problem gambling among minors to generate support for the “Don't Gamble Away our Future ™” program. Once permission was granted to enter the four school locations, teachers were given a training manual that showed them how to use the “Don't Gamble Away our Future ™” interactive CD-ROM as well as other training materials. Before the program was administered, gambling pathology was assessed among students ages 12 years and older. All of the students received a self-report pre-test that measured their knowledge of gambling behavior and associated risks prior to the program.
Following pre-tests, students participated in the 45-min program which consisted of lectures, discussion, and activities. Students also received a copy of the CD-ROM upon completion of the program. The CD-ROM was designed to reinforce the education from the program in a fun and interactive manner. Parents were invited to presentations that were free and open to the general public. The presentations were advertised through parent education packets and the media (e.g., radio announcements). Parent education packets were provided to each family prior to the program's implementation and included information about the project and an interactive website they could visit to access additional information regarding the project and problem and pathological gambling among minors.
Measures
Gambling pathology was assessed prior to the program's administration by using the Modified South Oaks Gambling Screen for Teens (MSOGST; Taylor 2008), a modified version of the original 20-item South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987). Individual items from the SOGS were reworded to better reflect the experiences of children and adolescents. The MSOGST contains 37 items and measures pathological gambling among children and adolescents (e.g., “Have you ever felt like you would like to stop betting money or gambling but didn't think you could?” “Have money arguments ever centered on your gambling?”). Like the SOGS, scores on the MSOGST range from 0–20, with higher numbers indicating more severe gambling pathology. Participants indicate “yes” or “no” for the majority of the scored items; two of the items assess the frequency of the behavior under question (i.e., never, some of the time, most of the time). The MSOGST identifies “non-problem gamblers,” “at-risk gamblers,” and “problem gamblers.” In a separate study (see Taylor 2008), the MSOGST demonstrated effective reliability and validity. In the current study, Cronbach's alpha was.87 for the scored MSOGST items, which indicated strong reliability. The program's effect on gambling behavior was not evaluated at the first time wave. Follow-up studies will be conducted to evaluate the effectiveness of the program at reducing gambling behavior and reported separately.
Gambling knowledge was measured using a pre-and-post-test designed by the IIAR. The pre-and-post-test contained the exact same items to avoid an instrumentation threat to internal validity. The primary school's pre- and post-tests consisted of items that assessed respondents' knowledge about gambling and the dangers associated with it. Item examples include “Which of the following are common gambling activities” (answers included “sports betting,” “bingo,” “lottery,” “video games,” and “all of the above”) and “A gambling addiction is a lot less serious than a drug or alcohol addiction” (respondents indicated “true” or “false”). Pre-and post-test scores ranged from 1–9, with higher scores signifying more accurate knowledge about the dangers of gambling. IIAR consulted a panel of experts in the discipline when creating the pre-and post-tests to establish their validity. Cronbach's alpha was computed and indicated that the pre-and post-tests demonstrated acceptable reliability (α = .58). The only demographic variables that were collected in the current study were gender, grade, and location.
Results
Demographics
The sample consisted of 8,455 students from four different types of schools: primary, junior high, high school, and a detention center. Fifty-two percent of the sample was female and the majority (56.7%) of the sample were high school students (n = 4,782); 30.6% from junior high schools (n = 2,585), 10.7% came from primary schools (n = 905), and 1.9% came from a detention center school setting (n = 163). The average pre-test score for the whole sample was 6.11 (SD = 2.09) and the average post-test score was 7.43 (SD = 1.95).
Effectiveness of Program on Changing Faulty Beliefs About Gambling
A paired-samples t test was conducted to determine the effectiveness of the program at teaching minors about gambling and the dangers associated with it. Results showed that the differences between test scores were significant. More specifically, post-test scores were higher than pre-test scores, t (8,454) = −50.89, p = .000, indicating that the participants did improve their knowledge about gambling and its negative effects after the program was administered.
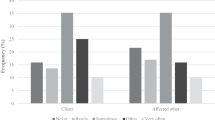
A mixed model analysis of variance was conducted to investigate whether there were differences in the amount of improvement in gambling knowledge following program administration by school type. The independent variable was school type and the dependent variable was the mean difference in scores on the pre-test and post-test. Results indicated that the main effect of time was significant, Λ = .91, F (1, 8431) = 796.1, p = .000, as was the interaction of time x location, Λ = .99, F (3, 8431) = 37.8, p = .000. Post-hoc comparisons established that the primary school experienced the most improvement in pre-to-post-test scores and that the high school experienced the least (see Fig. 1).

Profile plot of mean differences in pre- and post-test scores by school setting type (N = 8,455)
A mixed model analysis of variance was used to see if there were significant differences by gender for mean differences between the pre-and post-test scores. The independent variable was gender and the dependent variable was the mean difference in scores on the pre-test and post-test. Results indicated that males improved more on the post-test scores than females Λ = 1.00, F (3, 8433) = 20.8, p = .000 (see Fig. 2).

Profile plot of mean differences in pre- and post-test scores by gender (N = 8,455)
Prevalence of Problem Gambling at First Data Collection
MSOGST scores were used to determine gambling pathology in the sample. Scores among participants aged 12 years and older ranged from 0 to 20 and the mean was 1.37 (SD = 2.60) for the current sample. The majority of participants (60.3%) indicated that they did not have any problems with gambling (MSOGST score = 0), 29.7% reported “some” problems with gambling (MSOGST score = 1–4), and 10% had a score of 5 or higher, which represented “probable pathological gamblers.” Statistical tests to see if there were differences in the number of pathological gamblers by gender or by school type were not significant (the detention center was slightly more likely than the other locations to have pathological gamblers, but an effect size indicated that the effect was very small, Φ = .04).
Discussion
Research has indicated that adolescents are more susceptible to probable pathological gambling than adults (Messerlian et al. 2005). Up to 35% of adolescents gamble at least once a week (Delfabbro et al. 2005; Gupta and Derevensky 1998a) and 10–15% are at risk for developing serious problems (Turchi and Derevensky 2006). Consistent with existing research, results of the current study on adolescent gambling revealed that almost 40% of the participants revealed that they had at least some problems with gambling, and 10% fit the profile for probable pathological gamblers. No one likes to admit that their children gamble, but the results from the current study, as well as other research effectively demonstrate that gambling is accessible to and used by youth. These numbers are especially distressing when the negative consequences associated with gambling for adolescents and families are considered (Fong 2006; Jacobs 2000; National Gambling Impact Study Commission 1999; Problem Gambling Foundation of New Zealand 2006; Westphal et al. 2000). Although not all of the youth that engage in gambling will end up pathological gamblers (Messerlian et al. 2005), adolescent gambling is a serious issue that should not be taken lightly.
The current study examined the effectiveness of the “Don't Gamble Away our Future ™” preventative program's ability to educate youth about gambling and change faulty beliefs about the process and outcomes. Findings indicated that participants knew more about gambling and the dangers associated with it after the program than they did before the program was administered. Results also showed that younger children (i.e., primary school location) improved their scores more than older children (i.e., junior high, high school, and detention center locations), and males improved their post-test scores more than females. The “Don't Gamble Away our Future ™” preventative program was clearly effective in educating participants about gambling, its myths, and its potential outcomes.
It is essential that youth are educated about the myths associated with gambling (e.g., can beat the odds) because research has demonstrated that youth are more susceptible to faulty beliefs about gambling (Moore and Ohtsuka 1999). In addition, Messerlian et al. (2005) proposed that increasing knowledge and awareness of the risks associated with gambling is an important part of the primary prevention strategies they outlined in their Youth Gambling Risk Prevention model. Proposing and implementing big policy changes is difficult to accomplish and can take years. Incorporating a prevention program that teaches youth and their families about gambling and the dangers associated with it is a key first step in taking action to protect youth from the negative effects of gambling. It is also an affordable first step that is likely to be acceptable to the majority of the stakeholders affected by youth gambling. The “Don't Gamble Away our Future ™” program is relatively easy to implement, targets youth as well as their families, incorporates technology that is enticing to youth, and the current study demonstrated that it is effective in the short-term. Future research will evaluate the long-term effectiveness of the program on knowledge as well as on behavior.
Limitations and Future Directions
Limitations to the current research included the reliance on self-report methodology to determine program effectiveness, the lack of a control group for comparisons, and the short time period between the administration of the pre-test and the post-test. Self-report methodology runs the risk of participants responding with socially desirable answers to the questions, particularly when dealing with an issue like gambling. However, it is unlikely that the self-report methodology skewed the findings in light of the research that indicates most adolescents are brought into the world of gambling by family members who promote gambling as a socially acceptable behavior (Fong 2006; Hardoon et al. 2004). The short time period between pre-and post-test administration was necessary in the current research as permission to go into the school system was difficult to obtain in the first place. Future research should allow for a longer period of time between the pre-and post-tests to rule out repeated testing threats to internal validity. This study is part of a longitudinal research project and the results from additional time series data collections will be reported in the future. Finally, future research should include a control group for comparisons. Control groups help to rule out specific threats to internal validity, such as history and maturation.
In spite of the research regarding the potential negative effects of gambling on adolescents, few, if any, public policies have been developed to protect minors from risks posed by gambling (Pavalko 2004). Policymakers need to consider the developmental vulnerability of youth, as well as the higher risk of pathological gambling, the availability of gambling, and the negative outcomes of gambling for minors. It would be in the best interest of families and society for policymakers to develop policies targeting the risks associated with gambling among minors. Perhaps more importantly, policymakers could incorporate preventative measures to try and circumvent problem and pathological gambling among youth altogether. Preventative programs like IIAR's “Don't Gamble Away our Future ™” program can help protect youth from the negative consequences of gambling by educating them about the issue, the myths and misconceptions, and the dangers associated with gambling. Youth gambling researchers support this type of preventative programming (Messerlian et al. 2005). Incorporating preventative gambling programs is an accessible and affordable important first step in protecting youth and families from the dangers of problem and pathological gambling.
*This work is supported by the Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs, U.S. Department of Justice, under grant number 2004-JL-FX-0162.
References
Adlaf, E. M, Paglia-Boak, A., Beitchman, J. H., Wolf, D. (2006). The mental health and well- being of Ontario students 1991–2005. Centre for addition and mental health research document series, No. 18. Retrieved September 22, 2008 from http://www.camh.net/Research/Areas_of_research/Population_Life_Course_Studies/OSDUS/OSDUS2005_mental_detailed_fnl.pdf
American Psychological Association (1998, August 20). Pathological gambling more prevalent among youths than adults, study finds. Science Daily. Retrieved September 24, 2008, from http://www.sciencedaily.com/releases/1998/08/980820075118.htm
Atherton, J. S. (2005). Learning and teaching: Piaget’s developmental theory. Retrieved May 19, 2008, from http://www.learningandteaching.info/learning/piaget.htm
Buchta, R. M. (1995). Gambling among adolescents. Clinical Pediatrics (Phila), 34, 346–348. doi:10.1177/000992289503400701.
Delfabbro, P., Lahn, J., Grabosky, P. (2005). Adolescent gambling in the ACT. Report to the ACT Gambling and Racing Commission. Retrieved September 22, 2008, from http://www.gamblingandracing.act.gov.au/Documents/AdoGamReport.pdf
Derevensky, J. L., & Gupta, R. (2000). Youth gambling: a clinical and research perspective. eGambling: Electronic Journal of Gambling, 2, 1–18.
Derevensky, J., & Gupta, R. (2004a). The measurement of youth gambling problems: Current instruments, methodological issues, and future directions. In J. Derevensky, & R. Gupta (Eds.), Gambling problems in youth: Theoretical and applied perspectives (pp. 121–144). NY: Kluwer Academic/Plenum Publishers.
Derevensky, J., Gupta, R. (2004b). Adolescents with gambling problems: a synopsis of our current knowledge. eGambling: The Electronic Journal of Gambling, 10. Retrieved on May 2, 2008, from http://www.snsus.org/pdf/ejgi-issue10.pdf
Derevensky, J. L., Gupta, R., & Magoon, M. (2004). Adolescent problem gambling: legislative and policy decisions. Gaming Law Review, 8, 107–117. doi:10.1089/109218804774076385.
Dickson, L. M., Derevensky, J. L., & Gupta, R. (2002). The prevention of gambling problems in youth: a conceptual framework. Journal of Gambling Studies, 18, 97–159. doi:10.1023/A:1015557115049.
Ellenbogen, S., Derevensky, J., & Gupta, R. (2007). Gender differences among adolescents with gambling-related problems. Journal of Gambling Studies, 23, 133–143. doi:10.1007/s10899-006-9048-y.
Fong, T. W. (2006). Pathological gambling in adolescents. Adolescent Psychiatry, 29, 119–147.
Giedd, J. N. (2004). Structural magnetic resonance imaging of the adolescent brain. Annals of the New York Academy of Sciences, 1021, 77–85. doi:10.1196/annals.1308.009.
Gupta, R., & Derevensky, J. L. (1998a). Adolescent gambling behavior: a prevalence study and examination of the correlates associated with problem gambling. Journal of Gambling Studies, 14, 319–345. doi:10.1023/A:1023068925328.
Gupta, R., & Derevensky, J. L. (1998b). An empirical examination of Jacobs' general theory of addictions: do adolescent gamblers fit the theory? Journal of Gambling Studies, 14, 17–49. doi:10.1023/A:1023046509031.
Gupta, R., & Derevensky, J. L. (2000). Adolescents with gambling problems: from research to treatment. Journal of Gambling Studies, 16, 315–342. doi:10.1023/A:1009493200768.
Hardoon, K. K., Gupta, R., & Derevensky, J. L. (2004). Psychosocial variables associated with adolescent gambling. Psychology of Addictive Behaviors, 18, 170–179. doi:10.1037/0893-164X.18.2.170.
Haubrich-Casperson, J. (1993). Coping with teen gambling. New York: The Rosen Publishing Group, Inc.
Jackson, A. C., Dowling, N., Thomas, S. A., Bond, L., & Patton, G. (2008). Adolescent gambling behaviour and attitudes: a prevalence study and correlates in an australian population. International Journal of Health Addiction, 6, 325–352. doi:10.1007/s11469-008-9149-1.
Jacobs, D. F. (2000). Juvenile gambling in North America: an analysis of long term trends and future prospects. Journal of Gambling Studies, 16, 119–152. doi:10.1023/A:1009476829902.
Ladouceur, R., Boudreault, N., Jacques, C., & Vitaro, F. (1999). Pathological gambling and related problems among adolescents. Journal of Child Adolescent Substance Abuse, 8, 55–68. doi:10.1300/J029v08n04_04.
Langhinrichsen-Rohling, J., Rohde, P., Seeley, J. R., & Rohling, M. L. (2004). Individual, family, and peer correlates of adolescent gambling. Journal of Gambling Studies, 20, 23–46. doi:10.1023/B:JOGS.0000016702.69068.53.
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144, 1184–1188.
Louisiana Department of Health and Hospitals (n.d.). Don’t throw your chances away. Retrieved May 14, 2008, from http://www.thegamble.org/f_facts.htm
Messerlian, C., Derevensky, J., & Gupta, R. (2005). Youth gambling problems: a public health perspective. Health Promotion International, 20, 69–79. doi:10.1093/heapro/dah509.
Moore, S. M., & Ohtsuka, K. (1999). Beliefs about control over gambling among young people, and their relation to problem gambling. Psychology of Addictive Behaviors, 13, 339–347. doi:10.1037/0893-164X.13.4.339.
National Council on Problem Gambling (2006). Problem gambling resource and fact sheet. Retrieved on September 7, 2007, from https://www.themunsey.com/media/pdf/eapa_flyer.pdf
National Gambling Impact Study Commission (1999). Gambling impact and behavior study. Report to the National Gambling Impact Study Commission. Washington, DC: National Gambling Impact Study Commission.
National Research Council (1999). Pathological gambling: A critical review. Washington, DC: National Academy.
Pavalko, R. M. (2004). Gambling and public policy. Public Integrity, 6, 333–348.
Pettit, G. S., Bates, J. E., & Dodge, K. A. (1997). Supportive parenting, ecological context, and children’s adjustment: a seven-year longitudinal study. Child Development, 68, 908–923.
Problem Gambling Foundation of New Zealand (2006). Crime and gambling. [Brochure]. Auckland, NZ: Problem Gambling Foundation of New Zealand.
Problem Gambling Foundation of New Zealand (2008). Is the risk really worth it? Youth and problem gambling. [Brochure]. Auckland, NZ: Problem Gambling Foundation of New Zealand.
Russell, D. W., Booth, B., Reed, D., & Laughlin, P. R. (1997). Personality, social networks, and perceived social support among alcoholics: a structural equation analysis. Journal of Personality, 65, 649–692. doi:10.1111/j.1467-6494.1997.tb00330.x.
Siegler, R. (1991). Children’s thinking. Englewood Cliffs, NJ: Prentice Hall.
Stinchfield, R. (2000). Gambling and correlates of gambling among Minnesota public school students. Journal of Gambling Studies, 16, 153–173. doi:10.1023/A:1009428913972.
Stinchfield, R. (2004). Demographic, psychosocial, and behavioral factors associated with youth gambling and problem gambling. In J. Derevensky, & R. Gupta (Eds.), Gambling Problems in Youth: Theoretical and Applied Perspectives. New York: Kluwer Academic.
Stinchfield, R., Hanson, W. E., & Olson, D. H. (2006). Problem and pathological gambling among college students. New Directions for Student Services, 113, 63–72. doi:10.1002/ss.196.
Taylor, L. (2008). Evaluating an adolescent measure of gambling pathology. Paradigm, 13(1), 12–13 16–17 Winter.
Turchi, R. M., & Derevensky, J. L. (2006). Youth gambling: not a safe bet. Current Opinion in Pediatrics, 18, 454–458. doi:10.1097/01.mop.0000236398.17699.0d.
Westphal, J. R., Rush, J. A., Stevens, L., & Johnson, L. J. (2000). Gambling behavior of Louisiana students in grades 6 through 12. Psychiatric Services, 51, 96–99.
Winters, K. (2008a). Likelihood of developing an alcohol and cannabis use disorder during youth: association with recent use and age. Drug and Alcohol Dependence, 92, 239–247. doi:10.1016/j.drugalcdep.2007.08.005.
Winters, K. (2008b). The developing brain, adolescence, and vulnerability to drug abuse. Teaching Resource from the Mentor Foundation. University of Minnesota: The Mentor Foundation. Retrieved September 22, 2008 from http://www.mentorfoundation.org/uploads/Adolescent_Brain_Booklet.pdf
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Taylor, L.M., Hillyard, P. Gambling Awareness for Youth: An Analysis of the “Don’t Gamble Away our Future™” Program. Int J Ment Health Addiction 7, 250–261 (2009). https://doi.org/10.1007/s11469-008-9184-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-008-9184-y