
Abstract
Chronic ankle instability can be addressed surgically through direct lateral ligament repair, non-anatomic reconstruction, or anatomic reconstruction. The goal of this study was to assess the radiographic, functional, and clinical results of patients undergoing an anatomic lateral ankle ligament reconstruction using an anterior tibial tendon allograft. Eleven patients (12 feet; mean age, 48.9 ± 11.4 years) undergoing lateral ankle ligament reconstruction were followed at a mean of 3.5 ± 1.7 years after surgery (range, 1.2 to 5.0 years). Indications for surgery were previous failed repair (i.e., Broström; one case), hyperlaxity (seven cases), and high-demand patients (four cases). Subjective outcomes including the Foot and Ankle Outcome Score (FAOS), SF-36, and activity level were assessed. Mortise and lateral ankle stress radiographs were performed. The FAOS daily activity and sports activity subscores were 93.4 (range, 77.9 to 100) and 78.6 (range, 30 to 100), respectively. The SF-36v2 physical health and mental health components were 50.4 (range, 30.6 to 65.7) and 45.0 (range, 24.8 to 68.0), respectively. Four patients (five feet) reported no restriction; six patients reported mild restrictions, and one patient reported moderate activity restrictions. Tibiotalar tilt improved significantly from 20.2° to 4.6° after surgery (p < 0.01). The radiographic anterior displacement of the talus from the tibia was 6.5 mm postoperatively. The technique described restores mechanical stability in patients with chronic lateral ankle instability and may be considered in a select group of patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankle injury is extremely common in sports [1]. Of all ankle injuries, 85% involve the lateral ankle ligament complex [2]. In some cases, chronic instability may result from these acute episodes despite persistent conservative care [3–5]. Chronic instability and repeated ankle sprains can lead to degenerative arthritis if not treated [6, 7]. Between 50 and 80 different techniques to treat ankle instability have been described in the literature [8, 9].
The lateral ankle ligament complex is composed of three main ligaments: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL ligament courses from the inferior oblique segment of the anterior border of the fibula to the lateral malleolar articular surface of the talar body [10]. It is the most often injured during a lateral ankle sprain [11]. The CFL originates from the lower segment of the anterior border of the fibula, just below the ATFL, and inserts onto a tubercle on the lateral face of the calcaneus [10]. The PTFL originates from the medial fibular surface just below the digital fossa and inserts on the posterolateral aspect of the talus [10]. Due to its posterior position, the PTFL is the least affected during an inversion injury [12].
Techniques described to address chronic instability and injury to the lateral ankle ligaments can be categorized into three different groups: anatomic repair, non-anatomic reconstruction, and anatomic reconstruction. Anatomic repair involves the use of endogenous ligamentous tissue to restore the ligament. The most common types are the Broström [13, 14], the Gould modified Broström [15], and the Karlsson modified Broström [5]. This set of techniques can be used in cases when adequate tissue is present. However, reconstruction should be considered when severe attenuation of the ligaments has occurred precluding a simple, strong repair. Non-anatomic reconstruction techniques, including the Chrisman-Snook [16], Watson-Jones [17], and Evans [18] procedures, do not replicate the normal course and anatomy of the ATFL and CFL and may lead to stiffness [7, 19–21]. Methods of anatomical reconstruction of the lateral ligament complex have recently grown in number due, in part, to advancements in allograft preparation. These techniques offer the advantage of restoring the origin and insertion sites of native ligaments, thereby avoiding stiffness and preserving normal motion. Several different procedures have been reported in the literature [7, 8, 22–29].
The senior author has anatomically reconstructed the ATFL and CFL in a cohort of patients with chronic ankle instability using an anterior tibial tendon allograft. Though the technique has been previously described in both a cadaveric model [23] and human subjects[30], clinical results have never been reported. Patients were indicated when heavy demand, prior repair, ligamentous laxity, or inadequate tissue precluded direct repair.
We hypothesize that this reconstructive technique leads to good functional results and significantly improved radiographic measures of ankle instability. The goal of this study was to assess the radiographic, functional, and clinical results of patients undergoing an anatomic lateral ankle ligament reconstruction using an anterior tibial tendon allograft, a technique previously only described in a cadaveric model.
Methods
Eleven patients (12 feet) undergoing a lateral ankle ligament reconstruction by the senior author between February, 2004, and January, 2008, were brought back for a final follow-up visit at a mean of 3.5 ± 1.7 years after surgery (range, 1.2 to 5.0 years). The study was approved by the institutional review board at the investigators’ institution. All participants gave their informed consent prior to participation.
The cohort consisted of four males and seven females with a mean age of 48.9 ± 11.4 years. Indications for surgery were previous failed repair (i.e., Brostrom; one case), hyperlaxity (seven cases), and high-demand patients (four cases). Concomitant procedures were performed in nine cases (Table 1). Hindfoot varus, when present, was addressed with a lateralizing calcaneal osteotomy (seven cases). A dorsiflexion osteotomy of the first metatarsal was used in one patient with a high arch and varus hindfoot that corrected on a Coleman block (patient 8). Peroneal tendon pathology was treated with a peroneal tendon tenosynovectomy when scar was present around the tendons (four cases), peroneal tendon repair when more than 50% of the tendon was normal (five cases), or transfer of the flexor hallucis longus to the base of the fifth metatarsal when both peroneal tendons were markedly diseased (one case).
To perform the procedure, the patient is positioned in a supine or sloppy lateral position with a wedge or bean bag under the ipsilateral hip. Concomitant procedures are carried out as needed. The exposure for the reconstruction is performed through a longitudinal incision along the posterior aspect of the fibula in order to gain access to ATFL and CFL. This also allows exposure and inspection of the peroneal tendons. The decision to use the allograft reconstruction is made when the ATFL and CFL are deemed to be markedly deficient at the time of surgery (Fig. 1).

Schematic drawing of reconstruction. The tendon, after being fixed to the talus, is first passed through the superior fibular bone tunnel. It is then passed in an anti-parallel fashion through the inferior fibular bone tunnel before being passed lateral to medial through the calcaneal bone tunnel

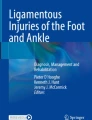
Mortise radiograph stress test. The amount of talar tilt, measured as the angle (in degrees) between the superior surface of the talus and the tibial plafond, was assessed using a mortise radiograph of the ankle. Maximal manual pressure was used to exert an inversion/varus force across the ankle joint. The talar tilt improved 43.1° preoperatively (a) to 5.6° postoperatively (b)
The tunnels are created by drilling over a Beath pin, and pin position is confirmed radiographically. A 5-mm tunnel is created in the talus at the isometric point of the insertion of the ATFL (Fig. 1). The isometric points are determined by identifying the insertion points of the indigenous ligaments. Two 5 mm tunnels are then made in the fibula: the more anterior starts at the origin of the ATFL on the anterior and distal fibula and exits proximally at the posterior fibular cortex while the second replicates the CFL by beginning at the inferior/anterior fibular tip, exiting the posterior fibula approximately 1 cm distal to the first hole. A final tunnel is then created at the insertion point of the CFL on the calcaneus and exits out the medial and posterior aspect of the calcaneus through a small counter incision. Care must be taken to assure that the pin used to guide this hole does not cross the subtalar joint as seen on an internal rotation view of the ankle. The path of the reconstructed ATFL is oriented approximately 130° with respect to the CFL. An anterior tibial tendon allograft is fashioned to a 5 mm diameter and tagged on either side with non-absorbable suture. Its approximate length is determined by measuring a vicryl suture run along its expected course. The graft is first fixed in the talus with a biotenodesis screw. It is then passed through the more superior fibular tunnel representing the ATFL, advanced distally across the posterior aspect of the fibula, and brought through the lower fibular hole representing the CFL. The graft is laid directly against bone along the posterior aspect of the fibula, deep to the peroneal tendons. It is then passed through the calcaneal tunnel. The ankle is brought into a position of slight eversion, with the talus in neutral in terms of anterior displacement. The graft is maximally tensioned and fixed into the calcaneus with a second biotenodesis screw. Early in the study, the ends of the suture were then tied around a 3.5-mm screw post on the medial calcaneal wall to add additional fixation. The senior author now only uses the biotenodesis screw to reduce the possibility of discomfort over the medial screw site. The wound is closed in layers after the ATFL and CFL are formally repaired in a pants-over-vest fashion with whatever tissue is available.

Lateral radiograph stress test. Radiographic anterior translation of the talus was assessed by measuring the nearest distance from the posterior edge of the distal tibial plafond (a) to the posterior edge of the joint surface on the talar dome (b). Maximal manual pressure was used to exert anterior translation of the talus
Functional outcomes were assessed by administering the Foot and Ankle Outcome Score (FAOS; 100-point maximum for each subscale), Short Form Health Status Survey (SF-36v2), and Visual Analog Scale for pain (VAS; ten point scale) were administered at the single, follow-up visit as noted above by an attending orthopedic surgeon with foot and ankle fellowship training (SJE). The reliability and validity of the FOAS have previously been shown in patients undergoing lateral ankle ligament reconstruction [31]. The survey consists of 42 questions concerning the foot and ankle, divided among six subscales: (1) symptoms, (2) stiffness, (3) pain, (4) function/daily living, (5) function/sports/recreational activities, and (6) quality of life. A postoperative Karlsson score survey was also administered [8, 32, 33]. Generalized ligamentous laxity was tested with the Beighton and Horan Joint Mobility Index (BHJMI; ten point scale with 10 being the most ligamentously lax) [34] at the single, follow-up visit as noted above by an attending orthopedic surgeon with foot and ankle fellowship training (SJE). A previously designed satisfaction survey was used to determine the overall satisfaction after ankle reconstruction (Table 2) [8, 35]. Preoperative and postoperative activity levels were compared using a previously described scale (Table 3) [8, 35]. Patients were asked about their ability to return to high level of sports of interest. The use of any ankle brace or orthotic use was also recorded.
Manual mortise stress radiographs were available for all patients preoperatively. Both lateral and mortise stress radiographs were taken at the final follow-up visit. Tibiotalar tilt was measured on the mortise stress view of the ankle (Fig. 2). A tibiotalar tilt of more than 10° was considered abnormal [36]. Anterior displacement of the talus with respect to the tibia was assessed on the lateral stress radiograph (Fig. 3) [37]. Any displacement more than 10 mm from normal was considered abnormal [36]. All radiographs were read independently and blindly by a board-certified, musculoskeletal radiologist.
Physical exam findings were recorded for each patient at the final follow-up visit (SJE). Pain to palpation, recorded as either “yes” or “no,” was assessed over specific areas of the foot associated with the reconstruction including the distal fibula, lateral calcaneal graft insertion site, medial calcaneal fixation site, talar graft insertion site, and both the medial and lateral gutters. Ankle joint range of motion was measured with the knee straight and flexed with a goniometer [38]. Triple joint complex was assessed and compared with the opposite side except in the case of the patient with bilateral involvement. Standing heel alignment was measured with a goniometer.
The patients were asked if the reconstruction felt too tight (recorded as “yes” or “no”) or if they have had any recurrent injuries since the operation (“yes” or “no”). In addition, patients were asked if they noted ankle instability, stiffness, or swelling in the ankle or foot during walking, standing, and resting. Complications including superficial or deep wound infection and sural nerve injury were recorded.
A Student's t test was used to compare the preoperative and postoperative lateral ankle stress radiographic measurements. Significance was set at p < 0.05. Descriptive statistics were used for all other parameters. All analyses were performed using SAS software version 9.1 (SAS Institute Inc., Cary, NC).
Results
At the time of final assessment, ten of the 11 patients demonstrated good to excellent results. In one patient, only a fair outcome was achieved. The FAOS at final follow-up demonstrated a mean pain subscore of 85.2 (range, 58.3 to 100), symptoms subscore of 80.4 (range, 42.9 to 100), mean daily activities subscore of 93.4 (range, 77.9 to 100), mean sports activities subscore of 78.6 (range, 30 to 100), mean quality of life subscore of 74.4 (range, 18.8 to 100), and mean stiffness subscore of 1.8 (range 0 to 6; Table 4). The SF-36v2 bodily pain scale subscore was 72.8 (range, 41 to 100), physical health component was 50.4 (range, 30.6 to 65.7), and mental health component was 45.0 (range, 24.8 to 68.0). The VAS was 1.8 (range, 0 to 5). The mean Karlsson score was 82.3 (range, 55 to 100). An unaffected ankle has a score of 100. The mean BHJMI ligamentous laxity score was 2.6 (range, 0 to 10) with a mean for females of 3.29 and males of 1.33. The population norm for post-puberty females is 3.03 and post-puberty males is 1.3[39]. On the satisfaction scale, five patients (six feet) reported excellent, five patients good, and one foot fair results. On the activity restriction scale, four patients (five feet) reported no restriction, six patients reported mild restrictions, and one patient reported moderate restrictions. All but four patients were able to return to their sport of interest. One patient (patient 1) severely injured his ankle during a soccer match prior to surgery. He did not feel confidant to returning to soccer or engaging in kick boxing, his other major sport. Another patient (patient 4) was an avid roller skater and dancer who had sprained her ankle on multiple occasions. After the operation, she returned to skating, but did not feel completely stable while spinning during dancing. Another patient (patient 5), a martial arts instructor had also sustained multiple ankle sprains. After the operation, he did not feel that he could kick as well as before, but was able to return to this sport. Finally, one runner (patient 9) twisted her ankle many times during running. She reported much improvement, but did not run long distances anymore. No patients used a brace, and two patients wore orthotics.
Significant improvement was found after surgery for the lateral ankle stress exam (p < 0.01) with the tibiotalar tilt improving from 20.2° preoperatively to 4.6° postoperatively. The anterior displacement of the talus from the tibia was 6.5 mm postoperatively.
The most common site for postoperative pain to palpation was the medial gutter (three feet) and lateral calcaneal graft insertion site (three feet; Table 5). No patient reported pain outside of the areas specifically assessed. Ankle range of motion with the knee straight was found to total 47.7° (range, 30° to 55°). The mean dorsiflexion was 6.7° (range, 0° to 10°) and plantar flexion was 41.0° (range, 30° to 45°). With the knee bent, the dorsiflexion increased to a mean of 12.5° (range, 5° to 20°). Triple joint motion was normal in nine feet (eight patients) and reduced by 25% in two patients. In one patient, the triple joint complex motion was reduced to 50% of the normal motion. The mean heel alignment at the follow-up measured 2.3° valgus (range, 1° varus to 7° valgus).
Three patients reported that they felt the reconstruction was too tight and limited their motion. Two of these patients had diminished triple joint motion, and one had diminished ankle joint flexion. No patient had a reinjury to the ankle. One patient (patient 10) had a Jones fracture of the fifth metatarsal 4.6 years out from surgery.
Two patients felt that their ankle was unstable. Two patients had stiffness in their ankle and two others felt stiffness for a few minutes in the morning. One patient felt she had constant swelling in the ankle, and two others reported swelling after intense physical activity. No patients had a superficial or deep infection, and no patients had an injury to the sural nerve.
Discussion
The purpose of this study was to assess the results of reconstructing the lateral ankle ligament complex using a technique previously described [23, 30], but whose results have not been reported in a cohort of patients. In the current study, good clinical and radiographic results after an anatomical reconstruction were demonstrated. Overall, all but one patient reported good to excellent satisfaction. There was significant improvement in the talar tilt as seen on radiographic stress exam.
The study is limited by its small patient cohort size and retrospective nature. Furthermore, the lack of a control group precludes important comparisons. Concomitant procedures represent confounding variables, making it more difficult to compare the results between patients. However, employing the same technique by the same surgeon did provide consistency among patients. Comparison between patients was also made more difficult given that it was not possible to determine from the charts or follow-up history how long patients had problems or symptoms prior to undergoing surgery. Patients may have had various durations of instability before their surgery. Though outcome scores were only available at latest follow-up, all but two patients had preoperative lateral tibiotalar tilt stress views which allowed for an objective assessment of the mechanical success of the reconstruction. Radiographic anterior translation of the talus is most commonly assessed by measuring the nearest distance from the posterior edge of the distal tibial plafond to the posterior edge of the joint surface on the talar dome [37]. The potential limitations of such a method and the fact that the contralateral side was not compared represent additional weaknesses of the study. Furthermore, the fact that anterior translation of the talus was not measured preoperatively is another limitation of the study.
Numerous outcome data scores including the satisfaction score [8], activity level [8], the Karlsson score [3], the BHJMI [40], SF-36v2, FAOS [41], and VAS were all collected, allowing comparison to other reports in the literature. The FAOS has been validated for lateral ankle ligament reconstructions [31] where as the satisfaction and activity levels and Karlsson score have previously been used in the literature to study lateral ankle ligament reconstruction [5, 8, 42]. The BHJMI has been proven reliable in a cohort of female patients [40]. The patients in this series did not seem to be more hypermobile than the population at large which suggests that the primary indication for the technique was not ligamentous laxity.
Anatomical reconstruction of the lateral ankle ligament complex replicates isometry, potentially preventing stiffness in the ankle and subtalar joints. Such techniques may offer increased strength compared with simple repair, particularly in cases of severely attenuated lateral ligaments. Non-anatomical reconstructions, such as the Chrisman-Snook [16], Watson-Jones [17], and Evans [18] risk donor site morbidity such as a reduction in eversion strength due to loss of peroneal tendon function and stiffness secondary to non-isometry. Anatomical reconstruction techniques with autograft, such as the gracilis [8], reproduce isometry, but concomitantly create donor site morbidity.
Only three other allograft reconstruction techniques have been reported in the literature [7, 24, 25]. Autograft has also been used in the anatomical reconstruction of the lateral ankle ligaments [8]. The anatomical reconstruction techniques reported in the literature vary in terms of the drill hole configuration, graft insertion sites, choice of graft, and graft anchoring technique [7, 8, 23–25, 27, 29, 36, 43–45]. Three of the techniques use a single bone tunnel in the fibula [8, 24, 25, 36]. Three employ two bone tunnels in the fibula [7, 23, 27, 44], while two others use an incomplete bone tunnel and secure a split graft at the tendon–bone interface [29] or use biotenodesis screws, respectively [45]. The bone tunnel configuration used by the senior author is similar to that reported in several previous studies [7, 23, 30, 46]. In one [7], two separate fascia lata allografts were used. In two other studies [23, 46], a gracilis autograft was performed, but no clinical data was presented. The current study is therefore the first to present clinical data on a two fibula bone tunnel method using anterior tibial tendon allograft. In the early cases in the current study, a calcaneal screw post was used in addition to a biotenodesis screw to provide additional fixation for the graft and decrease the risk of the graft pulling out of the calcaneal tunnel. However, the senior author now uses only the biotenodesis screw which generally provides excellent fixation.
There are theoretical risks associated with this technique. First, the use of allograft could potentially be rejected by the host. However, the tendon grafts are hypocellular and are treated in an Allowash solution (LifeLink Tissue Bank, Tampa, FL) and sterilized with gamma irradiation, thereby minimizing the chance for disease transmission. Furthermore, strict tissue bank guidelines are followed at the investigators’ institution. The exposure for the reconstruction technique tends to require longer incisions and greater soft tissue dissection than for direct repair. This raises the chance of a sural nerve or vascular injury, though neither was reported in the current cohort of patients.
It is important to understand several aspects of the technique described. First, most lateral ankle instability does not severely disrupt the integrity of the ligaments which can therefore be addressed with direct repair. When ligamentous degeneration is too severe to preclude simple repair, reconstruction should be considered. Second, the fixation of the graft to bone can be performed with interference screws alone instead of adding traditional screw posts as performed in this study. Third, the allograft need not be the anterior tibial tendon, but rather can come from other sources including the Achilles tendon. Finally, when addressing ankle instability, it is our opinion that it is crucial to attend to the concomitant deformities. In patients with varus heel alignment, a lateralizing calcaneal osteotomy should be performed to reduce the stress on the lateral ankle ligaments. If the patient has a forefoot driven cavus deformity, it is important to address the first ray inclination. A dorsiflexion osteotomy through first metatarsal or a first tarsometatarsal fusion should be considered.
In conclusion, we have reported the results of lateral ankle ligament reconstruction using an anterior tibial tendon allograft in a small cohort of patients. This represents the first clinical assessment of this technique. All patients showed good to excellent activity level and significant improvement in radiographic ankle stability after the reconstructive procedure. Some level of stiffness was present yet most, but not all, returned to their preinjury level of sport. The current technique is indicated when endogenous tissue is too attenuated or disrupted to achieve substantial repair, after failed attempt at repair, and in ligamentously lax or high-demand patients.
References
Garrick JG. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains. Am J Sports Med. 1977;6:241–242.
Garrick JG. Epidemiology of sports injuries. Presented at Third Annual Sports Medicine Symposium. 1973.
Karlsson J, Bergsten T, Lansinger O, Peterson L. Reconstruction of the lateral ligaments of the ankle for chronic lateral instability. J Bone Joint Surg Am. 1988;4:581–588.
Karlsson J, Bergsten T, Lansinger O, Peterson L. Surgical treatment of chronic lateral instability of the ankle joint. A new procedure. Am J Sports Med. 1989;2:268–73; discussion 273–4.
Karlsson J, Eriksson BI, Bergsten T, Rudholm O, Sward L. Comparison of two anatomic reconstructions for chronic lateral instability of the ankle joint. Am J Sports Med. 1997;1:48–53.
Harrington KD. Degenerative arthritis of the ankle secondary to long-standing lateral ligament instability. J Bone Joint Surg Am. 1979;3:354–361.
Nakata K, Shino K, Horibe S, Natsu-ume T, Mae T, Ochi T. Reconstruction of the lateral ligaments of the ankle using solvent-dried and gamma-irradiated allogeneic fascia lata. J Bone Joint Surg Br. 2000;4:579–582.
Coughlin MJ, Schenck RC,Jr, Grebing BR, Treme G. Comprehensive reconstruction of the lateral ankle for chronic instability using a free gracilis graft. Foot Ankle Int. 2004;4:231–241.
Muijs SP, Dijkstra PD, Bos CF. Clinical outcome after anatomical reconstruction of the lateral ankle ligaments using the duquennoy technique in chronic lateral instability of the ankle: A long-term follow-up study. J Bone Joint Surg Br. 2008;1:50–56.
Sarrafian SK. Syndesmology. In: Anatomy of the Foot and Ankle. Philadelphia: J.B. Lippincott Company; 1983:143–198.
Holmer P, Sondergaard L, Konradsen L, Nielsen PT, Jorgensen LN. Epidemiology of sprains in the lateral ankle and foot. Foot Ankle Int. 1994;2:72–74.
Renstrom PA, Konradsen L. Ankle ligament injuries. Br J Sports Med. 1997;1:11–20.
Brostrom L. Sprained ankles. V. treatment and prognosis in recent ligament ruptures. Acta Chir Scand. 1966;5:537–550.
Brostrom L. Sprained ankles. VI. surgical treatment of “chronic” ligament ruptures. Acta Chir Scand. 1966;5:551–565.
Gould N, Seligson D, Gassman J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980;2:84–89.
Chrisman OD, Snook GA. Reconstruction of lateral ligament tears of the ankle. an experimental study and clinical evaluation of seven patients treated by a new modification of the elmslie procedure. J Bone Joint Surg Am. 1969;5:904–912.
Watson-Jones R. Recurrent forward dislocation of the ankle joint. J.Bone Joint Surg.Br. 1952;519.
Evans DL. Recurrent instability of the ankle; a method of surgical treatment. Proc R Soc Med. 1953;5:343–344.
Hollis JM, Blasier RD, Flahiff CM, Hofmann OE. Biomechanical comparison of reconstruction techniques in simulated lateral ankle ligament injury. Am J Sports Med. 1995;6:678–682.
Schmidt R, Cordier E, Bertsch C, Eils E, Neller S, Benesch S, Herbst A, Rosenbaum D, Claes L. Reconstruction of the lateral ligaments: Do the anatomical procedures restore physiologic ankle kinematics?. Foot Ankle Int. 2004;1:31–36.
Tohyama H, Beynnon BD, Pope MH, Haugh LD, Renstrom PA. Laxity and flexibility of the ankle following reconstruction with the chrisman-snook procedure. J Orthop Res. 1997;5:707–711.
Anderson ME. Reconstruction of the lateral ligaments of the ankle using the plantaris tendon. J Bone Joint Surg Am. 1985;6:930–934.
Boyer DS, Younger AS. Anatomic reconstruction of the lateral ligament complex of the ankle using a gracilis autograft. Foot Ankle Clin. 2006;3:585–595.
Caprio A, Oliva F, Treia F, Maffulli N. Reconstruction of the lateral ankle ligaments with allograft in patients with chronic ankle instability. Foot Ankle Clin. 2006;3:597–605.
Horibe S, Shino K, Taga I, Inoue M, Ono K. Reconstruction of lateral ligaments of the ankle with allogeneic tendon grafts. J Bone Joint Surg Br. 1991;5:802–805.
Okuda R, Kinoshita M, Morikawa J, Jotoku T, Abe M. Reconstruction for chronic lateral ankle instability using the palmaris longus tendon: Is reconstruction of the calcaneofibular ligament necessary?. Foot Ankle Int. 1999;11:714–720.
Pagenstert GI, Valderrabano V, Hintermann B. Lateral ankle ligament reconstruction with free plantaris tendon graft. Tech F and A Surg. 2005;2:104–112.
Paterson R, Cohen B, Taylor D, Bourne A, Black J. Reconstruction of the lateral ligaments of the ankle using semi-tendinosis graft. Foot Ankle Int. 2000;5:413–419.
Sugimoto K, Takakura Y, Kumai T, Iwai M, Tanaka Y. Reconstruction of the lateral ankle ligaments with bone-patellar tendon graft in patients with chronic ankle instability: A preliminary report. Am J Sports Med. 2002;3:340–346.
McGarvey WC, Clanton TO. Lateral ankle ligament reconstruction using allograft and interference screw fixation. In: Easley ME, Weisel SW, eds. Operative Techniques in Foot and Ankle Surgery. Philadelphia: Wolters Kluwer, Lippincott Williams and Wilkins; 2010:851–859.
Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001;10:788–794.
Messer TM, Cummins CA, Ahn J, Kelikian AS. Outcome of the modified brostrom procedure for chronic lateral ankle instability using suture anchors. Foot Ankle Int. 2000;12:996–1003.
Nimon GA, Dobson PJ, Angel KR, Lewis PL, Stevenson TM. A long-term review of a modified evans procedure. J Bone Joint Surg Br. 2001;1:14–18.
Beighton P, Horan F. Orthopaedic aspects of the ehlers-danlos syndrome. J Bone Joint Surg Br. 1969;3:444–453.
Coughlin MJ. Arthrodesis of the first metatarsophalangeal joint with mini-fragment plate fixation. Orthopedics. 1990;9:1037–1044.
Schenck RC,Jr, Coughlin MJ. Lateral ankle instability and revision surgery alternatives in the athlete. Foot Ankle Clin. 2009;2:205–214.
Lohrer H, Nauck T, Arentz S, Scholl J. Observer reliability in ankle and calcaneocuboid stress radiography. Am J Sports Med. 2008;6:1143–1149.
Sarrafian SK. Functional anatomy of the foot and ankle. In: Anatomy of the Foot and Ankle. 1st ed. Philadelphia, PA: J.B. Lippincott Company; 1983:375–425.
Quatman CE, Ford KR, Myer GD, Paterno MV, Hewett TE. The effects of gender and pubertal status on generalized joint laxity in young athletes. J Sci Med Sport. 2008;3:257–263.
Boyle KL, Witt P, Riegger-Krugh C. Intrarater and interrater reliability of the beighton and horan joint mobility index. J Athl Train. 2003;4:281–285.
Goksel Karatepe A, Gunaydin R, Kaya T, Karlibas U, Ozbek G. Validation of the turkish version of the foot and ankle outcome score. Rheumatol Int. 2009.
Krips R, van Dijk CN, Halasi PT, Lehtonen H, Corradini C, Moyen B, Karlsson J. Long-term outcome of anatomical reconstruction versus tenodesis for the treatment of chronic anterolateral instability of the ankle joint: A multicenter study. Foot Ankle Int. 2001;5:415–421.
Ferran NA, Oliva F, Maffulli N. Ankle instability. Sports Med Arthrosc. 2009;2:139–145.
Pagenstert GI, Hintermann B, Knupp M. Operative management of chronic ankle instability: Plantaris graft. Foot Ankle Clin. 2006;3:567–583.
Takao M, Oae K, Uchio Y, Ochi M, Yamamoto H. Anatomical reconstruction of the lateral ligaments of the ankle with a gracilis autograft: A new technique using an interference fit anchoring system. Am J Sports Med. 2005;6:814–823.
Boyer MI, Bowen V, Weiler P. Reconstruction of a severe grinding injury to the medial malleolus and the deltoid ligament of the ankle using a free plantaris tendon graft and vascularized gracilis free muscle transfer: Case report. J Trauma. 1994;3:454–457.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Level of Evidence: Level IV, Case Series
Rights and permissions
About this article
Cite this article
Ellis, S.J., Williams, B.R., Pavlov, H. et al. Results of Anatomic Lateral Ankle Ligament Reconstruction with Tendon Allograft. HSS Jrnl 7, 134–140 (2011). https://doi.org/10.1007/s11420-011-9199-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-011-9199-y