
Abstract
One of the greatest challenges of limb lengthening and deformity correction is deciding when the bone has healed enough to remove the external fixator. Standard radiography is the most common imaging method used to assess bone healing after distraction osteogenesis because it is widely available, cheap, and relatively safe. However, other imaging technologies and methods are being investigated that will help quantify bone healing after distraction osteogenesis, providing an objective method for deciding when it is appropriate to remove an external fixator. This review will examine the latest techniques used to assess bone healing after distraction osteogenesis including dual-energy X-ray absorptiometry scans, ultrasound, quantitative computed tomography, and digital radiography (X-ray). Recommendations for clinical practice will be outlined.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction and background
First introduced in the early twentieth century [1], distraction osteogenesis is a principle in which new bone (called the regenerate) develops in an area subjected to gradual tension. This technique was further developed and popularized by Professor Gavril Ilizarov during the 1950s for limb lengthening and reconstruction [2]. Distraction osteogenesis is now used worldwide for limb reconstruction particularly in cases of bone tumors, congenital deformities, bone defects, and osteomyelitis [3]. A minimally invasive, low-energy osteotomy is performed to fracture a bone into two segments. Usually, an external fixator is applied through percutaneously placed transosseus pins and/or wires that are connected to external scaffolding. The external fixator is used to stabilize the fragments and manipulate them to achieve lengthening or deformity correction.
External fixation rather than internal fixation is used for several reasons. The greatest advantage of external fixators is that they allow for control of movement of the bone fragments in multiple planes [4]. This postoperative adjustability is not possible using internal fixation. Additionally, external fixators are ideal for cases where soft tissue or bone is infected, tenuous, or poorly vascularized [5].
However, external fixation is not without its drawbacks. While there is an advantage to be able to place pins or wires through healthy-appearing skin, this ultimately creates a communicating tract between the skin and bone, increasing the potential for the development of pin tract infection which can lead to osteomyelitis [6, 7]. Prolonged periods of time in an external fixator can lead to multiple problems including osteopenia [8], an increased rate of persistent pain [9], and a considerable psychological burden [10, 11]. The importance of this issue has even been recognized by Professor Ilizarov who wrote that “leaving the apparatus on for longer than necessary is as harmful as removing the fixator too early” [12]. Orthopedic surgeons have taken direct aim at shortening the length of time required in the external fixator by creating new limb lengthening and deformity correction techniques, such as lengthening over nail and lengthening and then nailing [6, 13].
Determining the right time to remove the frame remains a challenge, and proper timing is extremely important to prevent regenerate refracture or deformation resulting in persistent deformity (see Fig. 1). Many argue that this is the most difficult and important decision the surgeon must make in limb lengthening and deformity correction. Several studies have attempted to model formulas to help predict the length of time one should remain in an external fixator. For example, Dinah [14] found after reviewing 27 tibia lengthenings in 24 patients that the required time in a frame could be estimated to be 54 days per desired centimeter of total limb lengthening centimeters on average for all patients. Unfortunately, formulas such as this do not work in many cases because bone healing is dependent on both biological and mechanical factors such as age, underlying pathology, mechanical load on and stiffness of the fixation device [15]. For this reason, all patients must be monitored individually for the assessment of progress of their bone formation.

AP and lateral digital radiographs of a 70-year-old woman who underwent knee fusion and femoral lengthening for a bone defect resulting from multiple failures of total knee arthroplasty. She presented with a collapsed regenerate 7 weeks after frame removal. AP (a) and lateral (b) radiographs before frame removal. AP (c) and lateral (d) radiographs at presentation of the regenerate collapse
Most surgeons balance qualitative and subjective assessments of bone healing against pressure from the patient (and the same surgeon) to have the frame removed. Many surgeons take into account variables such as whether the patient still has pain with weight bearing, examining gait with the external fixator, and/or dynamizing the frame for a period of time with observation. Even so, the main tool for healing assessment in clinical practice today is standard radiography in two planes. This standard comes from a study by Fischgrund et al. [15] who reported a low fracture rate of 3% when using guidelines that required three of four cortices in the anteroposterior and lateral radiographs to be continuous and at least 2 mm thick in order to have the external fixator removed. While using standard radiography is cheap and quick, the method of identifying three of four cortices does not produce reliable results. Anand et al. [16] found inter-observer agreement to be less than 50% between all involved orthopedic surgeons, suggesting that the assessment of bone healing by radiographs is subjective. Starr et al. [17] found that the decision to remove an external fixator based on radiographic assessment alone resulted in intra-observer and inter-observer variability moderately above chance. This high variability as to when surgeons find it appropriate to remove an external fixator may contribute, along with other factors (such as primary diagnosis), to the large cited rate of refracture after frame removal (3% to 50%) [18–22].
There is a need for a quick, inexpensive, and simple quantitative method to help orthopedic surgeons with determining when is it is appropriate to remove the frame after distraction osteogenesis. Direct stiffness measurements of the regenerate to assess healing using strain gauges attached to the fixator are often cumbersome and require the removal of the fixator. In addition, the equipment used for these direct tests are expensive and may not be available to all practices. Indirect methods are therefore of great interest to the orthopedic community. The literature has several individual reports of groups investigating methods such as dual-energy X-ray absorptiometry (DEXA) scan, ultrasound (US), quantitative computer tomography (QCT), and plain radiographs for this purpose. However, there is no current review in the literature. We therefore believe that a paper summarizing the literature on assessing bone healing after distraction osteogenesis would be useful.
Noninvasive methods
DEXA scans
DEXA is a scanning technique used to determine bone mineral density (BMD) and bone mineral content (BMC). DEXA scans are currently the most commonly used test for measuring BMD and BMC and one of the most accurate ways to diagnosis osteopenia or osteoporosis. While there have been numerous studies investigating DEXA use in assessing bone healing after fracture, very few studies have demonstrated a correlation between DEXA scan measurements and the biomechanical properties of bone after distraction osteogenesis. There have, however, been studies demonstrating that a tibia with a stiffness of 15 N m/degree or a femur with 20 N m/degree should be regarded as healed [23, 24]. For example, in one of these studies, Richardson et al. measured fracture stiffness in 212 patients with tibia fractures treated by external fixation. The researchers subsequently separated the patients into two groups. In one group, the decision to remove the fixator was based on clinical grounds (defined by Richardson et al. as when radiological and clinical findings were considered to show union). In the other group, the frames were removed when the measured fracture stiffness had reached 15 N m/degree in the sagittal plane. In the first group, there were eight refractures (6.8%), and in the second group, there were none. This result lead the group to state that a stiffness of 15 N m/degree provides a useful definition of union in tibia fractures and may be used to decide when to remove an external fixator. Unfortunately, to date no, studies have directly correlated the mechanical tests with DEXA measurements.
One study that identified a correlation between DEXA measurements and the biochemical properties of bone after distraction osteogenesis is by Reichel et al. [25] who performed mid-diaphyseal tibial corticotomies on 24 sheep. Reichel et al. showed that in lengthened ovine tibias, there was a correlation (R 2 = 0.60, p < 0.002) between the maximum torque and the bone mineral density in the regenerate region. The authors recommended that before fixator removal, the BMD of the callus region should reach 70% of the density in the contralateral side at the same region. However, these authors did not determine the 70% cutoff value based on their results but rather based this recommendation on an earlier study by Hamanishi et al. that recommended 70% as a cutoff [25, 26].
A clinical study correlating DEXA scan measurements to the biomechanical properties of bone after distraction osteogenesis was performed by Tselentakis et al. [27]. In this study, the authors monitored nine consecutive patients undergoing distraction osteogenesis of their tibia (six patients) or femur (three patients) by regularly measuring bending stiffness of the distraction segment and performing corresponding DEXA measurements starting 6 weeks after completing distraction. The authors found a high and significant correlation between fracture bending stiffness and the square of the BMC at the location of minimum bone density (R 2 = 0.77, p < 0.001). They concluded that DEXA scans may be used reliably and effectively to determine fracture bending stiffness and consequently may be valuable for determining the appropriate time for frame removal. Additionally, they found that linear densities of 2.8 and 3.2 g/cm correspond to stiffness levels of 15 and 20 N m/degree, respectively, and suggested that these numbers could be used as a cutoff. Although these findings are supportive of DEXA as a method for assessing bone healing after distraction osteogenesis, this study was significantly underpowered and thus failed to provide definitive evidence that DEXA can be used as a clinical method to decide when it is appropriate to remove an external fixator after distraction osteogenesis.
In 2008, a study by Chotel et al. [28] aimed to correlate DEXA measurements to bending stiffness in children and to subsequently use DEXA parameters to aid in deciding when to remove the external fixator after distraction osteogenesis. By monitoring 16 consecutive children who had 22 limbs lengthened by distraction osteogenesis, the authors determined that a regenerate BMC that was 75% of the contralateral leg (which also happens to correlate to 75% of the AP stiffness measurements) is a safe value for removal of the fixator. In their study, four patients sustained post-removal fractures, and these were the patients with a regenerate BMC that was less than 75% of the contralateral leg, which further supports the validity of their cutoff. This study differed from the Reichel et al. and Tselentakis et al. studies in that it provided data to substantiate a cutoff point after which frame removal would be safe, and it involved clinical scenarios.
There have also been several studies that have solely investigated the use of DEXA scan in assessing bone healing after distraction osteogenesis without correlating DEXA measurements to biomechanical properties. Eyres et al. [29, 30] studied the quantity and rate of formation of new bone during lengthening of 17 limb segments in ten patients using DEXA, US, and X-ray. The authors found that DEXA scan was the only method that could analyze the bone from 1 to 2 weeks after distraction to the end of lengthening. X-ray visualized new bone starting at 4 to 8 weeks, while the usefulness of ultrasound reached it limits at higher bone densities. In a 1997 paper, Maffulli et al. [31] collected data on the rate of regenerate BMC acceleration using DEXA in 11 children undergoing lengthening. The authors found a direct correlation between early bone formation and subsequent BMC increases. From these data, the authors concluded that BMC allows for monitoring of the lengthening process and suggested that it may be used not only to predict the bone formation rates in patients but also may prove useful in the decision as to when to remove the fixator. In another study, Reiter et al. [32] provided additional support for the use of DEXA scans in monitoring bone healing. BMD values were monitored in 21 patients during and after limb lengthening procedures on the femur or tibia. The authors found that DEXA BMD measurements increased after distraction and ultimately reached approximately 85% of the pre-lengthening BMD measurement. Reiter et al. did not specify the conditions in which they found it appropriate to remove the external fixator, though the study reported no post-frame removal fractures or deformities.
The only study that has applied and evaluated a method of using DEXA to determine when it is appropriate to remove an external fixator after distraction osteogenesis is by Saran and Hamdy [33]. In this paper, the authors reviewed the records of 26 patients who underwent 28 limb lengthening procedures. The patients were followed with monthly DEXA scans and the fixator was removed when the scans stabilized to less than a 10% increase between monthly scans and the plain radiographs did not show any major deficiencies or transverse lucencies in the regenerate bone. This resulted in no regenerate fractures and only one fracture in the proximal segment of the lengthened bone in a patient after fixator removal. The authors were able to maintain a low rate of post-removal fractures (3.6%) without keeping patients in the fixator longer than the typical patient (average healing index was 47 days/cm; average age 12.3 years, range 3–20 years).
The evidence supporting the use of DEXA scans in determining the extent of bone healing after distraction osteogenesis is growing. In a 2008 article, Brallion et al. [34] wrote that from their experience, DEXA measurements have replaced approximately two thirds of the conventional plain X-rays in monitoring these procedures. The authors added that DEXA is not without its weaknesses as it does not give a precise image of the cortical bone, an important component to consider in assessing bone healing. While initial studies suggest that DEXA scan may be useful in evaluating bone quality after distraction osteogenesis, it is clear that additional research would help DEXA to become a clinical standard. First, additional studies confirming that DEXA measurements correlate well with the strength of regenerate bone are needed. Second, it is important that a protocol is created and compared with the effectiveness of the current standard of evaluating bone healing with standard radiographs. An advantage of DEXA is that it can produce a number that can be used to objectively evaluate the regenerate rather than the subjective assessment of cortical bridging with standard radiographs, a measurement that has become further complicated by the use of the oblique fixator struts which regularly block the lateral view. However, DEXA, like radiographs, suffers in that it converts a three-dimensional object into a two-dimensional image and finally into a one-dimensional number and could therefore miss small cortical gaps that may lead to fracture with loading after fixator removal.
Ultrasound
Ultrasound is another noninvasive method that researchers have investigated for its usefulness in assessing bone healing after distraction osteogenesis. Ultrasound is inexpensive, readily available, and does not expose patients to any radiation. Ultrasound also has been shown to reveal new bone formation up to 3 weeks earlier when compared with standard radiography or DEXA scan [29, 35].
However, ultrasound has two disadvantages that ultimately limit its clinical effectiveness in assessing bone healing after distraction osteogenesis. First, a few studies have shown that ultrasound cannot differentiate changes in bone stiffness and strength after a certain point during healing [29, 36]. In 1993, Eyers et al. [29] studied the quantity and rate of formation of new bone during lengthening of 17 limb segments in ten patients using DEXA, ultrasonography, and radiography. The investigators found that the distraction gap appeared as an echolucent window which narrowed progressively and subsequently produced a hyper-reflecting line after which further consolidation could not be assessed. Second, ultrasound techniques are not reliable because there are many variables that cannot be controlled from one measurement to another. For example, the site of measurement may not be identical at different times of healing; thus, different path lengths would be used for the calculation of bone healing. Additionally, because most of the energy of ultrasound is transmitted through soft tissue, variable amounts of soft tissue overlying the bone may lead to fluctuations in measurements [37].
Likely as a result of these limitations described above, there are no studies in the literature investigating the use of ultrasound as a method determining whether the regenerate bone has healed enough to remove an external fixator. Studies have ultimately focused on the use of ultrasound in the early stages of distraction osteogenesis.
Quantitative computed tomography
QCT is another noninvasive method that can be used to measure bone healing after distraction osteogenesis. QCT is based on the differential absorption of ionizing radiation by calcified tissue or bone. Using standard CT scanners, physicians can compare attenuation measurements with a standard reference to calculate bone mineral equivalents. As discussed earlier in the DEXA section of this paper, Reichel et al. [25] demonstrated that there is a strong correlation between DEXA scan bone mineral density measurements and maximum torque resistance of the regenerate bone. Several studies have also shown that QCT bone measurements have a similar correlation.
In 1993, Markel et al. [37–40] compared QCT, single-photon absorptiometry, and DEXA measurements and showed that all three techniques had strong correlations with the torsional properties of healing canine tibial osteotomies. Markel et al. found that QCT had stronger correlations with local gap tissue properties than DEXA but suggested that the low resolution of the DEXA scanner used in the study could explain this result. In another study, Harp et al. [41] demonstrated a strong correlation between the apparent density of canine tibial specimens to QCT bone mineral density measurements. The authors derived an equation that accurately predicted the stiffness of tubular bones, including cortical and heterogeneous cancellous zones using measurements collected by noninvasive QCT. In 2003, Aronson and Shin [42] compared QCT, radiography, quantitative technetium scintigraphy with histology, and mechanical testing properties in an experimental series of 65 dogs undergoing unilateral tibial lengthening. The authors found that QCT was helpful in quantitatively demonstrating by bone mineral density and cross-sectional distribution that the regenerate bone was strong enough for fixator removal.
QCT analysis of healing bone after distraction osteogenesis has been slow to be adopted by the orthopedic community, but the research supporting its clinical use suggests that this method has much promise. QCT has the unique advantage in that it can provide high-resolution imaging of the healing bone while providing quantitative analysis of this area to help the clinician make an objective assessment of whether the bone has healed enough to remove the external fixator. The major disadvantage of QCT is its limited availability, high cost, and relatively higher relative radiation exposure to patients (compared to DEXA, ultrasound, and standard radiography). However, as technology improves, the availability of this method may increase and the cost should likely drop. Additionally, researchers are actively looking for ways to decrease radiation exposure of these scans.
Standard radiography
Standard radiography is the current clinical standard for assessing whether the bone has healed adequately for safe fixator removal after distraction osteogenesis. The presence of three out of four continuous cortices at least 2 mm thick on anteroposterior and lateral radiographs is a commonly cited criterion for the removal of the external fixator. This cortex-based recommendation comes from a retrospective study of femoral fractures treated with external fixation by Skaggs et al. [43]. The authors found a statistically significant association (p < 0.05) between the number of cortices demonstrating bridging callus at the time of fixator removal and the rate of refracture. They stated that fractures showing fewer than three cortices of bridging callus had a 33% rate of refracture, whereas fractures with three or four cortices of bridging callus had a 4% rate. Fischgrund et al. [15] noted that the same criteria were true for neocortical formation in a distraction osteogenesis model and specified that the three cortices should be continuous and at least 2 mm thick. Using this as a criterion for the removal of the external fixator, they achieved a low refracture rate of 3%.
However, Anand et al. [16] found inter-observer percentage agreement to be less than half between all involved orthopedic surgeons, supporting the observation that assessment of bone healing by radiography after distraction osteogenesis is subjective. Starr et al. [16] investigated the reliability of using radiographs as a method to assess bone healing and determined that the variation in the assessment of the number of cortices was slightly better than chance. The authors concluded that low refracture rates after removal of an external fixator may be more an indicator of clinical judgment by experienced practitioners than the accuracy of using radiographic evaluation.
With the advent of digital radiography, there has been an attempt to measure the X-ray in a more objective manner. There have only been two studies that have attempted to investigate a quantitative method using radiography to assess bone healing after distraction osteogenesis. The first paper was by Kolbeck et al. [44] who performed tibia distractions in 24 micropigs and developed a calibration curve for digital radiographic measurements of regenerate bone using graded aluminum blocks for calibration. The authors found a high correlation between the radiographic measurements using their calibration curve and the biomechanical measurements. They concluded that their method was a useful tool for the in vivo assessment of the regenerate bone during the consolidation period in distraction osteogenesis. A strength of the Kolbeck et al. study was that it correlated actual mechanical measurements to radiographic readings. However, a weakness of their study was that it did not look at patients in a clinical setting. The next paper by Hazra et al. [45] accomplished this by retrospectively looking at 70 patient charts and correlating their BMD measurements (measured with a Hologic QDR 1000 instrument) to calculate pixel density ratios. Hazra et al. calculated average pixel density values for each of the regenerate and a proximal segment on the same side by taking values from the cortical and medullary bone on both anteroposterior and lateral views. The average of the regenerate segment and the proximal segment was used to calculate the pixel density ratio. The authors used the ratio of proximal bone pixel density to regenerate pixel density because their raw pixel value which was inversely related to radiopacity (i.e., with an increase in radiopacity, the raw pixel value decreased). They were careful to avoid metal with all measurements and did not use the distal segment because it often undergoes severe osteoporosis during lengthening. In the end, Hazra et al. found a high correlation between measured BMD ratios and calculated pixel value ratio (R 2 = 0.79). Their scatter plot also showed good correlation and limited variability. The authors did not determine a cutoff point but concluded that pixel values measured on standard radiographs appear to indicate callus stiffness and may obviate the use of DEXA.
With the recent adaptation and spread of digital radiography, a quantitative method of using radiography to assess bone healing after distraction osteogenesis appears to be very possible. This technique would have the advantage of being readily available in many clinical centers, relatively cheap, and exposing patients to relatively little radiation. The major disadvantage of this method would be that it would be converting a three-dimensional object into a one-dimensional number; however, it is not entirely clear as to how important the three-dimensional visualization or assessment is with respect to bone strength assessment after distraction osteogenesis. Another important limitation with this method is the possible interference with hardware in the measurement areas.
Discussion
The decision of when is it appropriate to remove an external fixator after distraction osteogenesis is a challenging one. There have been several studies in the literature that have investigated different modalities and methods for the quantification of bone healing after distraction osteogenesis in order to help clinicians with this decision. In this paper, we have reviewed the literature of bone assessment after distraction osteogenesis with regards to various techniques including DEXA, ultrasound, QCT, and standard radiography. From this review, it is clear that more research is needed in this field, but the current work suggests that an improved objective method for this analysis is on the horizon.
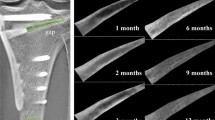
From our experience, we recommend that conventional radiography should be obtained monthly at each visit. While the beginning clinician may believe that the presence of three of four potential cortical bridges seen on orthogonal radiographs is an adequate criterion for fixator removal, it is important to note that despite this finding, overall bone density may still be significantly reduced. QCT is a modality that is and will be more and more helpful in quantitatively demonstrating by mineral density and cross-sectional distribution that the regenerate bone is strong enough for fixator removal. DEXA scan is unlikely to be as useful as it does not have the resolution or three-dimensional qualities of QCT. Ultrasound’s role in limb reconstruction is currently limited to the early stages of distraction osteogenesis. Digital radiography with pixel density ratio measurement shows much promise and may be a more accurate means for assessing the regenerate bone quality after distraction osteogenesis than current visualization of cortical bridging methods. For this reason, we have started to investigate the use of digital acquisition radiography as a method for assessing bone healing after distraction osteogenesis by comparing clinical outcomes rather than BMD ratio numbers as was done by Hazra et al. [45]. Using recent advances in medical imaging software, we are now able to sample and calculate the mean pixel values of large sections of bone, allowing for a more accurate assessment of the quantity and quality of the regenerate bone (see Fig. 2). There are two phases of our investigation. The first is a retrospective study that compares the mean pixel density ratios of two groups (refractured vs not refractured) that are matched by (gender, age, primary diagnosis, and amount of lengthening). With this study, we hope to establish a cutoff that we can use in a prospective study in which we use our radiographic method to determine when it is appropriate to remove a fixator. This second study will randomly place patients in a group in which the time to remove the fixator is determined by clinician judgment only or in a group in which it is determined by meeting the cutoff that we had defined in our retrospective study. Although studies correlating bone density may be helpful, only a study based on subsequent fractures after hardware removal would prove the usefulness of a particular method. With an outcome study based on fracture rates after external fixator removal, we aim to establish a simple, quick, inexpensive, and reliable method of assessing regenerate bone after distraction osteogenesis that will help reduce the occurrences of post-frame removal fractures and/or deformities.

Example of our sampling pixel density technique using AP and lateral digital radiographs from a 10-year-old child who underwent 4 cm of lengthening. The patient did not have any complications after frame removal. AP (a) and lateral (b) radiographs at the appointment before frame removal with pixel density measurements. Measurements on each radiograph demonstrate the mean pixel value for each segment (regenerate and the adjacent diaphyseal and metaphyseal bone). Higher pixel values correlate with more opaque sections on radiograph and denser bone. AP (c) and lateral (d) radiographs at the 1-month follow-up showing a well-healed regenerate
References
Codivilla A (1994) On the means of lengthening, in the lower limbs, the muscles and tissues which are shortened through deformity. 1904. Clin. Orthop. Relat. Res 301:4–9
Bertram C, Nielander KH, Konig DP (1999) Pioneers in the lengthening of the extremities. Chirurg 70 no. 11, 1374–1378
Birch JG, Samchukov ML (2004) Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J. Am. Acad. Orthop. Surg. 12 no. 3, 144–154
Fragomen AT, Rozbruch SR (2007) The mechanics of external fixation. HSS J. 3 no. 1, 13–29
Marsh DR, Shah S, Elliott J, Kurdy N (1997) The Ilizarov method in nonunion, malunion and infection of fractures. J. Bone Jt. Surg. Br. 79 no. 2, 273–279
Paley D, Herzenberg JE, Paremain G, Bhave A (1997) Femoral lengthening over an intramedullary nail. A matched-case comparison with Ilizarov femoral lengthening. J. Bone Jt. Surg. Am. 79 no. 10, 1464–1480
Velazquez RJ, Bell DF, Armstrong PF, Babyn P, Tibshirani R (1993) Complications of use of the Ilizarov technique in the correction of limb deformities in children. J. Bone Jt. Surg. Am 75 no. 8, 1148–1156
Cattermole HC, Cook JE, Fordham JN, Muckle DS, Cunningham JL (1997) Bone mineral changes during tibial fracture healing. Clin. Orthop. Relat. Res 339:190–196
Garcia-Cimbrelo E, Olsen B, Ruiz-Yague M, Fernandez-Baillo N, Munuera-Martinez L (1992) Ilizarov technique. Results and difficulties. Clin. Orthop. Relat. Res. 283:116–123
Eldridge JC, Bell DF (1991) Problems with substantial limb lengthening. Orthop. Clin. North Am. 22 no. 4, 625–631
Ghoneem HF, Wright JG, Cole WG, Rang M (1996) The Ilizarov method for correction of complex deformities. Psychological and functional outcomes. J. Bone Jt. Surg. Am. 78 no. 10, 1480–1485
Ilizarov GA (1990) Clinical application of the tension-stress effect for limb lengthening. Clin. Orthop. Relat. Res. 250:8–26
Rozbruch SR, Kleinman D, Fragomen AT, Ilizarov S (2008) Limb lengthening and then insertion of an intramedullary nail: a case-matched comparison. Clin. Orthop. Relat. Res. 466:2923–2932
Dinah AF (2004) Predicting duration of Ilizarov frame treatment for tibial lengthening. Bone 34 no. 5, 845–848
Fischgrund J, Paley D, Suter C (1994) Variables affecting time to bone healing during limb lengthening. Clin. Orthop. Relat. Res. 301:31–37
Anand A, Feldman DS, Patel RJ, Lehman WB, Bosse HJvan, Badra MI, Sala DA (2006) Interobserver and intraobserver reliability of radiographic evidence of bone healing at osteotomy sites. J. Pediatr. Orthop. B. 15 no. 4, 271–272
Starr KA, Fillman R, Raney EM (2004) Reliability of radiographic assessment of distraction osteogenesis site. J. Pediatr. Orthop. 24 no. 1, 26–29
Dahl MT, Gulli B, Berg T (1994) Complications of limb lengthening. A learning curve. Clin. Orthop. Relat. Res. 301:10–18
Danziger MB, Kumar A, DeWeese J (1995) Fractures after femoral lengthening using the Ilizarov method. J. Pediatr. Orthop. 15 no. 2, 220–223
Simpson AH, Kenwright J (2000) Fracture after distraction osteogenesis. J. Bone Jt. Surg. Br. 82 no. 5, 659–665
Aquerreta JD, Forriol F, Canadell J (1994) Complications of bone lengthening. Int. Orthop. 18 no. 5, 299–303
Forriol F, Iglesias A, Arias M, Aquerreta D, Canadell J (1999) Relationship between radiologic morphology of the bone lengthening formation and its complications. J. Pediatr. Orthop. B. 8 no. 4, 292–298
Dwyer JS, Owen PJ, Evans GA, Kuiper JH, Richardson JB (1996) Stiffness measurements to assess healing during leg lengthening. A preliminary report. J. Bone Jt. Surg. Br. 78 no. 2, 286–289
Richardson JB, Cunningham JL, Goodship AE, O’Connor BT, Kenwright J (1994) Measuring stiffness can define healing of tibial fractures. J. Bone Jt. Surg. Br. 76 no. 3, 389–394
Reichel H, Lebek S, Alter C, Hein W (1998) Biomechanical and densitometric bone properties after callus distraction in sheep. Clin. Orthop. Relat. Res. 357:237–246
Hamanishi C, Yasuwaki Y, Kikuchi H, Tanaka S, Tamura K (1992) Classification of the callus in limb lengthening. Radiographic study of 35 limbs. Acta Orthop. Scand. 63 no. 4, 430–433
Tselentakis G, Owen PJ, Richardson JB, Kuiper JH, Haddaway MJ, Dwyer JS, Evans GA (2001) Fracture stiffness in callotasis determined by dual-energy X-ray absorptiometry scanning. J. Pediatr. Orthop. B. 10 no. 3, 248–254
Chotel F, Braillon P, Sailhan F, Gadeyne S, Gellon JO, Panczer G, Pedrini C, Berard J (2008) Bone stiffness in children: Part II. Objectives criteria for children to assess healing during leg lengthening. J. Pediatr. Orthop 28 no. 5, 538–543
Eyres KS, Bell MJ, Kanis JA (1993) Methods of assessing new bone formation during limb lengthening. Ultrasonography, dual energy X-ray absorptiometry and radiography compared. J. Bone Jt. Surg. Br. 75 no. 3, 358–364
Eyres KS, Bell MJ, Kanis JA (1993) New bone formation during leg lengthening: evaluated by dual energy X-ray absorptiometry. J. Bone Jt. Surg. Br. 75 no. 1, 96–106
Maffulli N, Cheng JC, Sher A, Lam TP (1997) Dual-energy X-ray absorptiometry predicts bone formation in lower limb callotasis lengthening. Ann. R. Coll. Surg. Engl. 79 no. 4, 250–256
Reiter A, Sabo D, Pfeil J, Cotta H (1997) Quantitative assessment of callus distraction using dual energy X-ray absorptiometry. Int. Orthop. 21 no. 1, 35–40
Saran N, Hamdy RC (2008) DEXA as a predictor of fixator removal in distraction osteogenesis. Clin. Orthop. Relat. Res. 466:2955–2961
Braillon P, Chotel F, Berard J (2008) Limb lengthening: contribution of dual energy X-ray absorptiometry. J. Musculoskelet. Neuronal. Interact. 8 no. 1, 32
Young JW, Kostrubiak IS, Resnik CS, Paley D (1990) Sonographic evaluation of bone production at the distraction site in Ilizarov limb-lengthening procedures. AJR. Am. J. Roentgenol. 154 no. 1, 125–128
Bail HJ, Kolbeck S, Krummrey G, Weiler A, Windhagen HJ, Hennies K, Raun K, Raschke MJ (2002) Ultrasound can predict regenerate stiffness in distraction osteogenesis. Clin. Orthop. Relat. Res. 404:362–367
Markel MD, Chao EY (1993) Noninvasive monitoring techniques for quantitative description of callus mineral content and mechanical properties. Clin. Orthop. Relat. Res. 293:37–45
Markel MD, Wikenheiser MA, Morin RL, Lewallen DG, Chao EY (1990) Quantification of bone healing. Comparison of QCT, SPA, MRI, and DEXA in dog osteotomies. Acta Orthop. Scand. 61 no. 6, 487–498
Markel MD, Morin RL, Wikenheiser MA, Robb RA, Chao EY (1991) Multiplanar quantitative computed tomography for bone mineral analysis in dogs. Am. J. Vet. Res. 52 no. 9, 1479–1483
Markel MD, Morin RL, Wikenheiser MA, Lewallen DG, Chao EY (1991) Quantitative CT for the evaluation of bone healing. Calcif. Tissue Int. 49 no. 6, 427–432
Harp JH, Aronson J, Hollis M (1994) Noninvasive determination of bone stiffness for distraction osteogenesis by quantitative computed tomography scans. Clin. Orthop. Relat. Res. 301:42–48
Aronson J, Shin HD (2003) Imaging techniques for bone regenerate analysis during distraction osteogenesis. J. Pediatr. Orthop. 23 no. 4, 550–560
Skaggs DL, Leet AI, Money MD, Shaw BA, Hale JM, Tolo VT (1999) Secondary fractures associated with external fixation in pediatric femur fractures. J. Pediatr. Orthop. 19 no. 5, 582–586
Kolbeck S, Bail H, Weiler A, Windhagen H, Haas N, Raschke M (1999) Digital radiography. A predictor of regenerate bone stiffness in distraction osteogenesis. Clin. Orthop. Relat. Res. 366:221–228
Hazra S, Song HR, Biswal S, Lee SH, Lee SH, Jang KM, Modi HN (2008) Quantitative assessment of mineralization in distraction osteogenesis. Skelet. Radiol. 37 no. 9, 843–847
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Rights and permissions
About this article
Cite this article
Babatunde, O.M., Fragomen, A.T. & Rozbruch, S.R. Noninvasive Quantitative Assessment of Bone Healing After Distraction Osteogenesis. HSS Jrnl 6, 71–78 (2010). https://doi.org/10.1007/s11420-009-9130-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-009-9130-y