
Abstract
Little is known about the effectiveness of interventions for families living with parental mental illness. Existing interventions offer information about successfully implemented treatments, which may demonstrate effectiveness in research. In the current study, directors of programs for parents with mental illness and their families were interviewed. Qualitative analyses revealed noteworthy similarities with respect to target population; funding; community context; agency context; mission, theoretical orientation, and assumptions; locus of care and essential services; desired outcomes; and moderators. Program similarities were identified to provide parameters for research, and to contribute to the development of testable hypotheses. Family-centered, strengths-based approaches were identified across program directors as critical to intervention success.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Two-thirds of adults who meet the criteria for psychiatric disorders are parents.1 This is true across diagnostic categories, including adults who meet the criteria for serious mental illness.1 The current emphasis on community-based programs and brief hospital stays for all persons with mental illness, rather than lengthy periods of institutionalization, means that millions of families living in the community may be affected by parental mental illness. Research indicates that parents with mental illness share the same stresses and joys of all parents, but that they also face additional challenges related to mental illness.2 These challenges include overcoming stigma and discrimination, and the threat of child custody loss, in addition to the difficulty of parenting while managing a mental illness and psychiatric symptoms.2 Studies of parents with mental illness have found that parenting can indeed be compromised by these conditions, and that both children3 – 5 and parents6 – 8 may be adversely affected.
Families in which parents have mental illnesses are also families in which children are likely to have emotional and behavioral problems. Children of parents with mental illness are at greater risk for developing psychiatric conditions, and for other psychosocial problems such as poor social skills and poor school performance.4 , 5 , 9 – 11 In addition, children may be victims of stigma and discrimination similar to their parents, and may experience the trauma of family disruption and out-of-home placement due to a parent’s hospitalization or inability to care for them on a day-to-day basis. Thus, it appears that the need for effective interventions to support families, when feasible, and to prevent potentially devastating and costly outcomes for both children and adults, is critical. However, there have been very few studies on programs for parents with mental illness and their families. This is an unfortunate gap, given the need, and the potentially far-reaching benefits of interventions.
The literature on programs for families in which a parent has a mental illness is primarily composed of descriptive studies and studies using quasi-experimental designs. For example, early research on joint inpatient admission programs for mothers and babies, followed by intensive, home-based aftercare services found that mothers in the joint admission programs were less likely to refuse inpatient admission,12 were able to address parenting issues and build parenting skills during their hospital stay,13 – 15 had lower relapse rates after discharge,16 more adequately cared for their babies at discharge,16 and were more likely to have custody of their children at 2 years follow-up15 than mothers who had been admitted alone without their babies. However, important differences between groups of mothers, eg, age, marital status, and diagnosis, and the lack of descriptive data regarding the interventions necessary to ascertain comparability make it difficult to draw conclusions about the relationship of particular interventions to positive outcomes.
More recent research on programs for parents is similarly equivocal. Several program types were identified in a review of intervention programs by Cohler and colleagues.17 These included: (1) specialized, acute inpatient services for women that focus on both stabilization of mental health symptoms, and the interface of psychiatry and reproductive health;18 (2) intensive, comprehensive, community-based programs that address a wide range of mental health, rehabilitation, and parenting needs;17 , 19 , 20 and (3) less comprehensive support and education services for parents and children.21 , 22 Several programs across subtypes reported positive outcomes for adherence to complex and demanding treatment plans,23 improved parenting knowledge and skills, child custody, and increased independence,22 as well as for child development outcomes.17 However, most studies lacked a control group and relied on provider report.20 , 22 , 23 One study, employing a quasi-experimental design and standardized measures, raised as many questions as it answered. Specifically, Cohler and colleagues17 compared mothers and young children (0–5 years of age) receiving a comprehensive clinical and psychoeducational program, to mothers and young children receiving weekly home visits. Despite increased intensity and comprehensiveness of the treatment condition, and improvement overall, there were no differences between groups on parenting or child development outcomes. Studies to date, therefore, have documented positive effects across a variety of interventions, but have neither: (1) described intervention practices or processes sysxtematically; nor (2) modeled or tested relationships adequately between practices and processes, and desired outcomes.
Thus, what is effective? What do parents and children living with parental mental illness need to support positive outcomes and avert negative long-term consequences? Which interventions are most effective with which parents and children? Policy makers and providers are left to “respond to concrete human needs and make decisions in the face of inadequate information” (p. 182).24 Rather than developing interventions based on established knowledge, defined by Shonkoff24 as knowledge generated by the scientific community, and embedded in the active interaction of theory and empiricism, policy makers and providers must work in the world of reasonable hypotheses. That is, reasonable inferences derived from the continuous refinement of theories of change, and the ongoing assessment of service impacts, provide the “converging agenda” for science, policy, and practice (p. 185).24 Current programs provide reasonable hypotheses, and suggest efficient starting points for more rigorous research and the development of an evidence base for the treatment of parents with mental illness and their families.
The study of existing community interventions, as compared to those developed and tested in academic settings, is receiving increased attention and support for a variety of practical and methodological reasons.25 First, interventions developed in academic settings are often not effectively implemented in the community.26 As a result, researchers note the need for a “science of implementation” to define and describe the complex set of contextual factors that influence the dissemination of interventions and, in fact, moderate their effectiveness. Existing interventions, of necessity, already attend to these “real world” factors and, therefore, provide opportunities both to measure and to evaluate their influence, and to test effectiveness taking these factors into account.25 , 26 Second, existing interventions are already serving people, engaging and creating resources, and successfully negotiating the myriad of factors that influence implementation, eg, funding, staff training, and politics. From a practical and ethical perspective, it may be wiser to “fine-tune” a functioning intervention than to “start from scratch,” while parents and children remain unserved. The wisdom of service providers24 must be brought to bear in weighing the potential benefit of implementing untested interventions versus the potential risk or cost of implementing those that may ultimately be found to be ineffective or even harmful.
Similarities across programs may illuminate important intervention characteristics or mechanisms. For example, documented interventions for parents with mental illness and their families reflect common innovations in thinking and practice. Interventions appear to share: (1) the recognition that adults with mental illness bear and raise children; and (2) the assumption that, with the appropriate supports and services, many adults with mental illness can parent effectively.18 – 23 , 27 , 28 In addition, interventions described in the literature reflect the central values of preserving family integrity, and preventing family separation, disruption, and custody loss.23 , 27 Differences across existing programs may highlight the range of characteristics and variability in needs among parents with mental illness and their children at different ages, and provide definition to the continuum of potentially effective intervention strategies.
The goals of the current study were (1) to describe existing programs for parents with mental illness and their families across the United States as systematically as possible along dimensions of target population; funding; community context; agency context; mission, theoretical orientation, and assumptions; locus of care and essential services; desired outcomes; and moderators; and (2) to integrate these findings, using qualitative research methods, to identify intervention and contextual factors that suggest testable hypotheses. Program directors, whose interventions are specifically targeted to parents with mental illness and their families, were interviewed to contribute to the development of an evidence base for practice arising from the experiences of policy makers, service providers, consumers, and family members in existing interventions.
Methods
Sample of programs
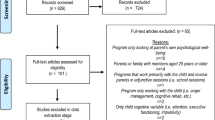
Snowball, convenience sampling was used to identify intervention programs for parents with mental illness and their families in the United States. An initial survey was sent to members of a mailing list (N = 300) compiled by the research team as part of their ongoing efforts to develop resources and provide technical assistance to policy makers, providers, advocates, and consumers concerned with parents with mental illness and their families. A letter explaining the study, and a stamped, self-addressed response card to indicate interest was included. The letter and card also included a request to forward information about any other known programs or providers working with families living with parental mental illness. Thirty-seven programs were identified as a result of the mailing. These programs were supplemented with the names of programs identified by state mental health authority directors in a prior study of interventions for parents with mental illness.29 Fifty-three programs were identified in total.
Based on information provided by initial survey respondents, the prior study,29 and brief telephone interviews with providers, programs were categorized into high, medium, and low specificity, with respect to focus on parents with mental illness. “High specificity” reflected programs designed and developed for parents with mental illness and their families (n = 23). “Medium specificity” reflected interventions that provided parenting-related services in which parents with mental illness participated, eg, parenting classes, but their specific needs were not the focus (n = 13). “Low-specificity” programs (n = 17) included programs for adults with mental illness, eg, psychosocial rehabilitation clubhouse programs, but that did not have specialized services for parents or children. In order to identify intervention practices and processes most relevant to families in which a parent has a mental illness, and most likely to contribute to the development of the evidence base, the current study focused on “high-specificity” programs.
Twenty of the 23 high-specificity programs were included in the current study. Two program directors did not respond to multiple requests for interviews, and one program director could not be interviewed due to staff changes and scheduling difficulties. Participating programs were located in 11 states and in the District of Columbia (see Table 1 for selected program characteristics). Five programs were located in New York, four in California, and two in Illinois. Alaska, District of Columbia, Colorado, Iowa, Massachusetts, Michigan, Missouri, New Mexico, and Rhode Island each had one program. The programs in Alaska and Colorado, however, were scheduled to close at the end of the current funding cycle due to lack of funding. The newest program participating in the study had been in operation for 4 years, whereas the oldest had been operating for 22 years.
Instruments
A semistructured telephone interview was developed to gather data from program directors on target population; funding; community context; agency context; mission, theoretical orientation, and assumptions; locus of care and essential services; desired outcomes; and moderators. These dimensions, initially derived from the literature on mental health services and programs, were selected to provide rich descriptive data about the programs. Interview items were based on items from a prior study of intervention programs for parents with mental illness,29 and from review of interviews and descriptions from similar accounts of relevant services and programs.18 , 19
Program directors were selected as the respondents best able to provide comprehensive information on the interventions. Program directors were contacted by telephone by the researchers, who explained the study and requested participation. Interviews were scheduled during the winter and spring of 1999 for program directors who consented to participation, and ranged in length from 1 to 2 h. Interview items focused on program characteristics and routine management information. No individual identifying information nor data regarding specific individuals were obtained.
Analyses
Interview data were coded by the researchers for concepts and themes, based on the underlying dimensional structure of the interview as defined above, eg, target population, funding, community context, etc. Within this framework, increasingly narrow and specific categories of concepts and themes were defined to condense extensive raw data30 , 31 and to identify common themes. The reliability of findings for the current study were enhanced by the coding of data by multiple researchers, comparison with findings in previous research on interventions for parents with mental illness, children, and families, and feedback from research participants.31
A logic model was constructed to illustrate the relationships between core dimensions as defined by interviews. Logic models are known to be useful for describing complex interventions and formulating hypotheses about relationships among inputs, processes, activities, eg, services and outcomes.32 As such, logic models provide a good framework for the development of testable intervention models.
Results
Target population
All programs served families affected by parent mental illness (Table 1). Twelve programs provided services for both parents and children, whereas the eight remaining programs served mothers and children or mothers only. Although programs served both parents and children, target population differed with respect to whether the parent diagnosed with a mental illness, or the child determined to be “at-risk” because of a parent’s illness, was the referred or “identified” client. Fifteen programs were defined by referral and primary funding that was “attached” to the parent (mother or father). Four programs were defined by child referral and related funding, and one program took referrals for both parents and children.
Parents
Parents with serious mental illness, eligible for state mental health services, and their children were the most commonly targeted population. Eligibility requirements for program participation defined differences across intervention programs. The most frequent requirements were age of parent (>18 years of age), age of child (eg, 0–5 years), and caregiving status (parent as caregiver). Four intervention programs were designed specifically for parents with mental illness who were also homeless. Program directors of programs open to fathers reported that relatively few were actually served. Only one program, which was developed as part of a research study on mothers with schizophrenia, limited enrollment by diagnosis. The most common diagnoses among parents as approximated by program directors were Schizophrenia, Major Depression, Bipolar Disorder, and Borderline Personality Disorder. Posttraumatic Stress Disorder and Substance Use Disorder were common as secondary diagnoses.
Racial and ethnic characteristics of program participants varied greatly by geographic location. Caucasian participants accounted for 4% to 98% of participants across intervention programs, with programs in Alaska, Colorado, Iowa, Montana, New York, and Rhode Island reporting at least 50% Caucasian participants. African American participants ranged from less than 1% to 95% of program participants, with programs in New York having 50% African American participants; and programs in Washington, DC, Illinois (Chicago), and Michigan (Detroit) having more than 90% African American participants. Participation among Hispanic parents ranged from less than 1% to 65%. Programs in New York City and New Mexico reflected the greatest proportion of Hispanic participants. Relatively small numbers of Asian parents participated in programs, with the exception of programs in California that reported approximately 11% Asian participants.
Children
Many intervention programs did not keep data on how many children they had served. Overall, children ranged in age from birth to 18 years; however, program directors reported that most child participants were school age or younger. Seven programs were limited to parents with young children (0–5). According to program directors, the emphasis on services for young children reflected funding sources that targeted early intervention and prevention, and the reality that many parents with mental illness were no longer caregivers of their children at later ages. One director of a program that provided supported housing in a staffed residence acknowledged that they could not provide appropriate supervision for potentially troubled adolescents, and were concerned for the sustainability of the larger program should they enroll families with older children.
Funding
Program funding reflected a variety of federal, state, local, and private sources, including Medicaid, Department of Housing and Urban Development (HUD), State or County Mental Health Authorities (S/C MHA), Early Intervention, Public Health, Child Welfare, McKinney, City Mental Health Authorities (eg, New York, NY funds), private foundations, and research grants. Thirteen programs reported more than one funding source. As can be seen in Table 1, Medicaid and S/C MHA were the most common sources of funding.
All program directors reported funding changes during the period of operation. Changes in funding often reflected changes in funding priorities and availability by funding sources (eg, Medicaid, S/C MHA); however, changes also often reflected changes in program priorities in response to experience with parents with mental illness and their families, and recognition of clients’ needs. Several program directors reported that they were often in the position of educating funders in order to advocate for change. For example, providers from a program originally supported by child welfare that targeted parents with mental illness involved in the child welfare system found that they were unable to serve parents effectively, or advocate for them appropriately within this structure. Child welfare support created a conflict of interest felt by parents and providers, given the mandates of the child welfare system and the roles and expectations for workers. Shifting funding, ie, securing State/County Mental Health dollars by advocating within their agency and S/C MHA, allowed the program to change its priorities, although not necessarily its practices.
Changes in funding were reported to offer both positive and negative influences, eg, an influx of HUD funding in one program allowed for additional housing subsidies for client families, whereas state budget cuts in another resulted in staff reductions. Overall, funding for programs was highly related to historical, experiential, and to community and agency context factors.
Community context
Program directors identified community context factors they perceived as highly relevant to program initiation, development, and sustainability, and that influenced the achievement of desired program and client outcomes. For example, directors noted that the wealth of the local economy and economic resources, progressive state and local politics, innovative state and local mental health systems, and the existence of collaborative relationships between providers and service sectors were highly influential in program development and sustainability, and as moderators of outcomes. Program directors highlighted two significant community factors in the development and sustainability of programs: the recognition of community needs and the contribution of influential advocates.
Programs for parents with mental illness and their families reflected two developmental trajectories reflecting the recognition of needs: (1) those initiated to serve adults with mental illness who were parents; and (2) those initiated to enhance child development and prevent developmental delays for children whose parents have mental illness. The majority of programs included in the current study reflect the first trajectory (n = 13). These adult-oriented interventions were initiated by adult mental health providers and policy makers who recognized that parents with mental illness comprised a meaningful subgroup of adults with mental illness, that as a group they required specialized services, and that these needs were not being met by existing services.
The second developmental trajectory is reflected in two subgroups of interventions. One subgroup (n = 5) was initiated by early intervention or child welfare providers, who recognized that a high proportion of the “high-risk” families referred for services included a parent with a mental illness whose needs were not adequately met by existing programs. The second subgroup (n = 2) included researchers and providers interested in risk and resilience processes among children of adults with mental illness, who developed family interventions targeting risk factors.
A second factor in the development and sustainability of an intervention program was the existence of one or more devoted and impassioned advocates who saw parental mental illness as an important issue. These advocates, who included providers, administrators, and policy makers, were generally positioned to be able to engage sufficient political and economic support within a human service agency, and within the larger political and economic community, to procure funding and continued support.
Agency context
Agency factors, such as size of agency and staffing, were also reported to be relevant to intervention development, implementation, and sustainability, and to client outcomes. Several program directors reported that affiliation with larger agencies that supported an array of services and staffing was beneficial. Most program directors reported that their programs were small, and insufficient relative to need. Program capacity was reported in different ways across programs, due both to type of program and data collection procedures (Table 1). Most programs described the number of parents and/or families able to be served at a given time, whereas other programs reported the number of individuals or families seen in a year. For programs reporting number of families seen at a given time, capacity ranged from 6 to 60 families. One program that provided services for women seen during tenure in homeless shelters reported serving 300 women with children in a year. A second program seeing women with mental illness receiving obstetrical and gynecological care at an outpatient community clinic reported serving between 75 and 100 women each year. Three programs reported variable capacity depending upon clinician or inpatient bed availability, and three had unknown capacityFootnote 1 (Table 1).
Staffing for programs was relative to both the numbers of parents served and the comprehensiveness of the program. All programs had a director; and some had an additional coordinator or supervisor, in addition to direct care providers. For many programs, directors and supervisors also provided direct services. Case managers from programs reflecting a comprehensive case management model worked with between four and 12 families.
Mission, theoretical orientation, and assumptions
Mission
All intervention programs shared the mission of enhancing functioning and supporting development for adults, children, and families. Mission statements were divided by emphasis on serving adults with mental illness as parents, or their children at risk for developmental delays.
Theoretical Orientation
Programs reflected a range of theoretical orientations. When asked about primary theoretical orientation, eight program directors identified psychosocial rehabilitation or psychosocial rehabilitation in combination with child development, three identified child attachment/psychodynamic theory, three identified psychoeducational alone or in combination with child development, or research-based psychoeducational approaches. Two programs each reported family-centered/strengths-based approaches, feminist theory, and one program each reported trauma informed cognitive behavioral, and narrative therapy. In most cases, program directors reported that programs actually reflected multiple theoretical orientations and approaches to treatment that resulted from changes in conceptualization and practice in response to experience with parents and families, and more accurate recognition of needs. Program directors also noted that in addition to whatever primary theoretical orientation they relied upon, interventions were, of necessity, defined by pragmatic approaches, ie, providers were willing to do “whatever it takes” to help families achieve their goals.
Assumptions
Although interventions reflected a diversity of theoretical underpinnings, all program directors talked about the concepts of “family-centered” and “strengths-based” as key assumptions upon which interventions were built. As shown in Table 1, two programs actually reported that these assumptions defined their primary theoretical orientation. Program directors further stated that family-centered, strengths-based approaches related directly and indirectly, through enhanced parent self-esteem and parenting efficacy, to achievement of positive outcomes for parents and children.
Locus of care and essential services
Locus of Care
Programs fell into three broad categories: inpatient programs (n = 2) comprehensive community-based programs (n = 10), and circumscribed community-based programs (n = 9). One program that had both an inpatient and outpatient service was included in two categories (inpatient and circumscribed community-based). Inpatient programs were hospital units with providers trained to address both mental and reproductive health, as well as medical and mental health issues prevalent among women, eg, trauma and domestic violence. These interventions were, by definition, intensive and short term, targeting acute stabilization and referral to community-based services for longer-term follow-up. Inpatient programs were distinguished by their recognition of and attention to reproductive health issues among women with mental illness, and by specialized cross-training for providers on psychiatry and Obstetrical/Gynecological (OB/GYN) inpatient units.
Comprehensive community-based interventions were defined by an array of essential services offered to meet the needs of families, eg, case management, care coordination, etc. Several of the comprehensive community-based programs had residential components (n = 3); the majority provided services on an outpatient basis (n = 7). Circumscribed community-based programs generally offered a more targeted treatment, eg, dyadic therapy for parent and child, parent education, and support groups, and did not provide formal case management or access to a continuum of services.
Locus of care was related to the length of time clients participated in programs, with inpatient programs reflecting the shortest length of service (2–4 weeks); circumscribed community-based programs reflecting a middle length of service (3 months to 1 year); and comprehensive community interventions the longest (9 months to 3 years). Length of participation, however, was reported to vary greatly across families within any program. For example, some women could remain on an inpatient unit beyond the brief timeframe, some parents participated repeatedly in the same circumscribed program, such as psychoeducational or support groups, and some families were involved with comprehensive interventions for briefer or longer tenures according to family need.
Essential Services
A wide array of interventions or treatment types were provided across programs. All program directors reported that parent education and support was a central and critical aspect of their program. However, this service was not always formalized but delivered as part of case management or dyadic therapy. As can be seen in Table 1, seven programs offered parent education and support as part of a structured group therapy service. Formal comprehensive case management services were also provided by seven programs. Three of these programs also provided residential services. It is important to note that directors of programs in which formal case management was not provided reported the need for such services, and acknowledged that staff often functioned as case managers out of necessity.
Case management reflected two types: (1) “care coordination” models, and (2) “clinical” models. Care coordination models, by far the more prevalent type, focused on access to and coordination of multiple services and providers, and parent education and role modeling in the context of a highly supportive provider–consumer relationship. Clinical models also focused on access to and coordination of services and providers; in these programs, however, case managers were licensed clinicians who also provided individual and/or family therapy in the context of case management.
Most programs did not provide traditional mental health services as part of their program, but referred to external providers. Three programs, however, provided dyadic parent–child therapy as the central program service. Three programs provided medication management. Two programs each provided parent coaching and supervised visitation. One provided psychiatric consultation to an outpatient OB/GYN clinic and one provided financial support. Although only one program defined financial support as an essential service, many program directors reported that programs provided emergency financial assistance and concrete support, eg, furniture and clothing on occasion. Four programs had therapeutic nurseries that focused on child development in conjunction with services for parents. In addition to direct services for young children, therapeutic nurseries offer opportunities for parents to observe developmentally supportive teacher–child relationships and to participate in the child’s learning experience.
Finally, two specialized inpatient services addressed the unique reproductive health and parenting needs of women admitted during a psychiatric crisis. This included medication evaluation, crisis stabilization, group and individual therapy, occupational therapy, consultation from all medical services in the hospital, and referral for follow-up in the community.
Desired outcomes
Directors reported on desired outcomes defined both by the intervention orientation and funding and by parents and families themselves. Desired outcomes for inpatient programs were crisis stabilization, medication adjustment, medical and reproductive care, and appropriate referral for follow-up in the community. Desired outcomes for comprehensive community-based interventions were family-inclusive. That is, the central objective was improved functioning across multiple domains for all family members. For parents, this included access to stable and safe housing, entitlements, mental health and medical care; improved employment/education, medication management, and problem solving/crisis management; increased social support network and community resources, knowledge about child development, and the impact of mental illness on family life; and enhanced parenting skills and child safety. For children, this included achievement of development milestones, school readiness, school performance, and emotional and behavioral adjustment.
Although directors of circumscribed community-based programs recognized the need for the same desired outcomes as comprehensive programs to support effective parenting, their programs identified circumscribed outcomes consistent with the particular intervention. For example, programs offering parent education and support groups focused on the desired outcomes of improved knowledge of child development, enhanced parenting skills, and parenting efficacy. Programs providing dyadic therapy focused on similar desired outcomes, but emphasized parent responsiveness and parent–child attachment. Differences in explicit goals across all types of programs were unified by the central underlying objective of supporting family integrity, parenting knowledge and skills, parent self-efficacy, and child safety.
Parent- and family-defined outcomes, as reported by program directors, were remarkably similar across programs. First and foremost, parents expressed the desire to retain or regain caregiving responsibility for their children, and the wish to be free of the involvement of child protective services. Consistent with these goals, parents were reported to want access to safe and affordable housing, parent education and support, and mental health services for themselves and their children.
Outcome data
None of the programs included in the current study had formal, aggregate outcome data available at the time of our interview. Two programs reported they were collecting and tracking standardized outcome data, but did not yet have results. Most programs tracked and evaluated outcomes for parents and children with respect to individual and family service and treatment plans. Progress on identified goals was monitored and recorded in family files. Outcomes routinely assessed included housing, tenure in the community, treatment adherence, number of hospitalizations, mental health symptoms, sobriety, employment, parenting knowledge and skills, parent–child relationship, child custody, and child development and adjustment. In addition to individualized progress evaluations, most programs collected satisfaction data and reported very high rates of satisfaction with services.
Moderators
Although the current study did not explicitly assess moderating factors, program directors spontaneously identified several common moderators—factors “outside” the intervention that affected outcomes. Both individual (ie, parent and child) and contextual factors were reported. With respect to individual moderators, program directors reported that availability of natural supports (eg, church), better cognitive functioning, and good symptom management all related to better outcomes for parents, children, and families. Severity of a parent’s mental illness, presence of a parental substance abuse disorder or Axis II pathology (personality disorders), illegal immigration status, and severity of child emotional and behavioral problems were associated with poorer outcomes.
Contextual factors paralleled community and agency factors already listed above. Specifically, the extent of community resources, such as the availability of affordable housing, public transportation, childcare, and other social services, was related to better outcomes for parents and families; the lack of these resources, in addition to living in crime- and substance abuse-ridden neighborhoods, were related to poorer outcomes. Innovation in mental health systems, such as flexible funding and interagency collaboration, and the availability of a wide array of funded mental health services contributed to better outcomes for families. Finally, agency factors such as supportive leadership and affiliation with a comprehensive human service agency where multiple services could be quickly accessed, and interprovider cooperation and teamwork were greater, were reported to facilitate better outcomes.
Logic model
Figure 1 displays a logic model illustrating hypothesized relationships between key intervention and contextual components as defined by interviews with program directors. These components include target population; funding; community context; agency context; mission, theoretical orientation, and assumptions; locus of care and essential services; desired outcomes; and moderators. Characteristics showing high similarity across interventions were included in the appropriate boxes to suggest elements that may reflect critical or core factors. Contextual factors, represented by the boxes reflecting community context, agency context, and moderators, are set off by boxes with dashed lines to distinguish them from the intervention, but are included to emphasize their hypothesized influence on program development, implementation, and effectiveness, and their importance to the development of testable intervention models.

Hypothesize logic model for interventions for families affected by parental mental illness.
The logic model suggests that for an intervention targeting parents with mental illness and their children, desired outcomes result from the application of two essential services—parent education and support, and case management. Although case management was not uniformly provided, program directors consistently reported the need for case management to support access to and coordination of multiple needed services.
The logic model further specifies that these services are influenced by the availability and source of funding, the presence of particular community and agency contextual factors noted by program directors, and the application of family-centered, strengths-based approaches. Finally, the logic model identifies potential moderators of outcomes, including individual characteristics such as the availability of supports and severity and chronicity of a parent’s mental illness, and contextual characteristics of the community and agency in which the intervention is developed and delivered.
Discussion
Development of effective, evidence-based interventions for families in which a parent has a mental illness is critical. Millions of adults and children are affected by parental mental illness and the potential for poor and potentially devastating outcomes for both children and adults is great. Although prior research has lacked methodological rigor, results suggest that existing interventions may provide a good foundation for rigorous study and the development of evidenced-based practices. As recently articulated by Shonkoff,24 service delivery is a science of trial and error in the real world where data are not always available to support action with respect to a present problem. Clinical practice therefore, provides “wisdom”24 (p. 182) from which “reasonable hypotheses” can be generated for more scientific testing24 (p. 183).
The central goal of the present study was to take the first steps in this direction by systematically describing existing practices and processes. Results defined characteristics and practices that can be further operationalized and tested for effectiveness. In addition, because the current study used a “service to science” approach,33 findings reflected intervention practices and related processes successfully sustained in the “real world,” taking many of the contextual variables that affect implementation into account.24
Results revealed that interventions reflected both remarkable diversity and similarity. Similarities are particularly noteworthy considering the lack of an existing evidence base upon which to base practice, the relative isolation of programs from each other, diverse local contexts, different funding sources, and divergent theoretical orientations. Specifically, programs were united by a common underlying orientation to parents with mental illness and their children that promoted the use of “family-centered,” “strengths-based,” approaches, and parent education and support as a central intervention, to meet the complex needs of the families with whom they worked. Case management was also reported by program directors to be a desirable and necessary service for most families. Program directors from programs that offered case management and from those which did not agreed that need for case management services exceeded current availability. These common principles and strategies were reported to influence positive outcomes both directly and indirectly. Unfortunately, a lack of formal evaluation data to support these impressions was also common across programs.
In the absence of rigorous empirical data, the common themes and practices identified in the current study may define core processes and practices upon which to base the development of testable models. The logic model constructed from the current findings (see Fig 1) illustrates these core processes and practices with respect to outcomes, and offers a preliminary framework for testing which will require: (1) specification of the components of particular interventions with respect to processes, practices and outcomes; (2) manualization; and (3) the development of appropriate instruments to measure intervention fidelity.
Research on children’s mental health services and early intervention, which have emphasized family-centered, strengths-based approaches, can provide guidance for future research efforts.34 – 36 Validated instruments such as the Family-Centered Behavior Scale,37 developed to assess these processes and practices within child service systems, can be modified for research when parents with mental illness are initially identified as the clients. Care must be taken to translate these constructs appropriately, and to recognize where further innovation in measurement and methodology is necessary.
The current study has several limitations. First, by design, the authors focused on programs in the United States only. Innovative services for parents and families exist in other parts of the world,38 and examination of cross-cultural differences and similarities may prove illuminating and important with respect to both research and practice. Second, although the authors cast a wide net using both prior research and well-established mailing lists of providers and policy makers in the field, the current study may have inadvertently excluded some high-specificity programs within the United States in a way that compromises generalizability of the findings.
Third, it is important to note that the current study identified and focused on public sector services. It is unclear whether the lack of identification of private sector programs reflects a shortcoming in recruitment methods or the absence of such programs. Questions regarding differences in needs, services, and outcomes for parents and families served in the public and private sectors remain unanswered. Finally, the current study used interview data from a single informant across sites—program directors. Future research would benefit greatly from the integration of data from multiple sources including program staff, program participants, ie, parents and children, mental health system administrators, and policy makers, and collaborators from other service system sectors, eg, child welfare.
Implications for Behavioral Health
The current study advances knowledge about interventions for families in which a parent has a mental illness, and provides the groundwork for taking the next steps in the development of an evidence base regarding existing practices. The current study identified common program processes and practices that may be “key ingredients” with respect to positive outcomes, and offers a model “template” for future refinement and testing. Rigorous testing of interventions will inform practice and policy.
Family-centered, strengths-based approaches reflect general principles that guide practices. Specifically, these approaches focus on the family rather than the individual as the unit of intervention, and emphasize strengths rather than deficits.34 – 36 Within this framework, treatment begins with a thorough assessment of the entire family, and the development of an intervention tailored to the family’s specific and unique culture, needs, and goals. Family culture includes a family’s ethnic and cultural background, as well as the more specific “family culture” that defines and reflects relationships and patterns of behavior within a particular family, and incorporates changing child developmental needs, child–parent “fit,” and the interaction of parent and child mental health needs.
Family-centered, strengths-based approaches, however, do not fit with traditional clinical or funding paradigms, eg, fee for service, reimbursement for medically necessary services targeted to individual clients. Collaboration between and integration of adult and child service systems will have to be advanced, and reimbursement structures will have to be modified to accommodate such integration.
As noted above, prior research on children’s mental health services can provide guidance with respect to content and methods,34 , 35 but may not be an exact fit for families in which the parent is diagnosed with a mental illness. For example, the service needs and required level of interagency collaboration may offer challenges that children’s mental health services have yet to consider. Specifically, the need for integration across adult and child service sectors, and the emphasis on parenting and primary prevention may require a new level of innovation within mental health and social services systems. In addition, the dynamics around presenting for and receiving services is likely to reflect different tensions and require novel approaches when the parent rather than the child is the person with mental health needs, eg, concerns about stigma and loss of child custody. Finally, family-centered, strengths-based interventions for parents with mental illness will have to respond to the need for, and support a variety of child custody and caregiving arrangements from a strengths-based perspective. Collaborative relationships between adult mental health systems and child welfare authorities may be particularly salient in this regard.
The current study additionally underscores the very small number of interventions available for families affected by mental illness generally, and for families in which the father has a mental illness in particular. Although slightly more than half of the programs identified offer services to school-age and older children, program directors reported that the majority of children served are less than 5 years of age. The dearth of high-specificity interventions in contrast to the high prevalence figures indicates that most parents with mental illness and their families are either served by less parent-specific interventions or meet their needs by “stringing together” an uncoordinated and nonspecific array of services. Sadly, it is likely that many families receive no services at all.
In summary, the news on parents with mental illness and their children is both hopeful and challenging. Existing interventions may be very helpful to families who can access them, but the need for services exceeds availability, and empirical evidence supporting impressions of effectiveness is limited. The current study, along with others, provide information about what may work; however, research is needed to better define and test key ingredients and theoretical models. Current data indicate that intervention models are likely to be complex, requiring sophisticated research and analytic designs to test. Ultimately, evidenced-based models will have to be brought to scale and sustained across diverse communities. Despite these challenges, the potential for promoting quality of life, preventing adverse outcomes, and addressing an important public health issue requires us to move science and service forward on behalf of families living with parental mental illness.
Notes
As seen in Table 1, program capacity is “Unknown” for three programs. The item assessing program capacity was not included on the earliest interviews, and so is missing for these programs.
References
Nicholson J, Biebel K, Katz-Leavy J, et al. Prevalence of parenthood among adults with severe mental illness. In: Manderscheid RW, Henderson MJ, eds. Mental health, United States, 2002. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services; 2004.
Nicholson J, Sweeney EM, Geller JL. Mothers with mental illness: I. The competing demands of parenting and living with mental illness. Psychiatric Services. 1998;49:635–642.
Goodman SH, Brumley HE: Schizophrenic and depressed mothers: relational deficits in parenting. Developmental Psychology. 1990;26:31–39.
Goodman SH, Gotlib IH. Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission. Psychological Review. 1999;106:458–490.
Oyserman D, Mowbray CT, Meares PA, et al. Parenting among mothers with a serious mental illness. American Journal of Orthopsychiatric. 2000;70:296–315.
Cox AD, Puckering C, Pound A, et al. The impact of maternal depression in young children. Journal of Child Psychology and Psychiatry. 1987;28:917–928.
Hammen C, Burge D, Stansbury K. Relationship of mother and child variables to child outcomes in a high-risk sample: a causal modeling analysis. Developmental Psychology. 1990;26:24–30.
Keitner GI, Miller IW. Family functioning and major depression: an overview. American Journal of Psychiatry. 1990;147:1128–1137.
Barocas R, Seifer R, Sameroff AJ. Defining environmental risk: multiple dimensions of psychological vulnerability. American Journal of Community Psychology. 1985;13:433–447.
Sameroff AJ, Seifer R. Familial risk and child competence. Child Development. 1983;54:1254–1268.
Weintraub S, Neal JM. Social behavior of children at risk for schizophrenia. In: Watt N, Anthony EJ, Wynne LC, Rolf JE, eds. Children at Risk for Schizophrenia: A Longitudinal Perspective. New York: Cambridge University Press; 1984:243–263.
Fowler DB, Brandon RE. A psychiatric mother and baby unit. Lancet. 1965;I:160–161.
Bardon D, Glaser YIM, Prothero D, et al. Mothers and baby unit: psychiatric survey of 115 cases. British Medical Journal. 1968;2:755–758.
Margison F, Brockington IF. Psychiatric mother and baby units. In: Brockington IF, Kumar R, eds. Motherhood and Mental Illness. London: Academic Press; 1982:223–238.
Stewart DE. Psychiatric admission of mentally ill mothers with their infants. Canadian Journal of Psychiatry. 1989;34:34–38.
Barker AA, Morrison M, Game JA, et al. Admitting schizophrenic mothers with their babies. Lance. 1961;ii:237–239.
Cohler BJ, Stott FM, Musick J. Distressed parents and their young children: interventions for families at risk. In: Goepfert M, Webster J, eds. Parental Psychiatric Disorder: Distressed Parents and their Families. Liverpool, England: Liverpool Psychotherapy & Consultation Service; 1996:107–134.
Gold Award. Comprehensive prenatal and postpartum psychiatric care for women with severe mental illness—University of Illinois at Chicago Women’s Program, Chicago. Psychiatric Services. 1996;47:1108–1111.
Gold Award. Supportive residential services to reunite homeless mentally ill single parents with their children — The Emerson–Davis Family Development Center in Brooklyn, New York City. Psychiatric Services. 2000;51:433–1435.
Mohit DL. Management and care of mentally ill mothers of young children: an innovative program. Archives of Psychiatric Nursing. 1996;X:49–54.
Bassett H, Lampe J, Lloyd C. Living with under fives: a programme for parents with mental illness. British Journal of Occupational Therapy. 2001;64:23–28.
Waldo MC, Roath M, Levin W, et al. A model program to teach parenting skills to schizophrenic mothers. Hospital and Community Psychiatry. 1987;38:1110–1112.
Lieberman HJ, Campanelli PC, Ades Y, et al. Reunifying single-parent families with special needs. Psychiatric Rehabilitation Journal. 1999;23:42–46.
Shonkoff JP. Science, policy, and practice: three cultures in search of a shared mission. Child Development. 2000;71:181–187.
Hoagwood K, Burns BJ, Weisz JR. A profitable conjunction: from science to service in children’s mental health. In: Burns B, Hoagwood K, eds. Community Treatment for Youth. New York: Oxford University Press; 2002:327–376.
Weisz, JR. Lab–clinic differences and what we can do about them. Clinical Child Psychology Newsletter Spring 2000;15, No. 1.
Munk BD. Providing integrated treatment for parent/infant dyads at risk because of parental emotional and mental illness. National Center for Clinical Infant Program. April/May 1993;13:29–35.
Rubovits PC: Project Child. An intervention programme for psychotic mothers and their young children. In: Goepfert M, Webster J, et al., eds. Parental Psychiatric Disorder: Distressed Parents and their Families. 1996:161–168.
Nicholson J, Geller JL, Fisher WH. State policies and programs that address the needs of mentally ill mothers in the public sector. Hospital and Community Psychiatry. 1993;44:484–489.
Guba EG, Lincoln YS. Competing paradigms in qualitative research. In: Denzin NK, Lincoln YS, eds. Handbook of Qualitative Research. Thousand Oaks, CA: Sage Publications; 1994:105–117.
Thomas DR. A general inductive approach for qualitative data analysis. School of Population Health, University of Auckland, New Zealand. URL: http://www.health.auckland.ac.nz/hrmas/resources/qualdatanalysis.html. Date accessed: February 1, 2004.
Millar A, Simeone RS, Carnevale JT. Logic models: a systems tool for performance management. Evaluation and Program Planning. 2001;24:73–81.
Katz-Leavy J, Faenza M, Ringeisen H, et al. From Science to Service and Service to Science: A Two-Way Street. Topical discussion presented at the 16th annual research conference: a System of Care for Children’s Mental Health: Expanding the Research Base, Tampa, FL, March 2–5, 2003.
Friesen B, Karoloff N. Family-centered services: implications for mental health administration and research. Journal Mental Health Administration. 1990;17:13–25.
Koroloff NM, Friesen BJ. Challenges in conducting family-centered mental health services research. Journal of Emotional and Behavioral Disorders. 1997;5:130–137.
Stroul BJ, Friedman RM. A System of Care for Severely Emotionally Disturbed Children and Youth. Washington, DC: CASSP Technical Assistance Center, Georgetown University; 1986.
Allen RI, Petr CG, Brown BFC. Family-Centered Behavior Scale and User’s Manual. Lawrence, KS: University of Kansas Beach Center on Families and Disability; 1995.
Cowling V (Ed). Children of Parents with Mental Illness (1st ed.). Melbourne: Axis Publishing Services; 1999.
Acknowledgments
This research was supported by a contract from the Center for Mental Health Services, Substance Abuse and Mental Health Services Administration (CMHS-99M00481801D). Data from this article were presented at the Tampa meeting of the 15th Annual Research Conference for Children’s Mental Health in March 2002. The authors would like to thank our colleague from the UMMS Center for Mental Health Services Research, Valerie Williams, for her comments on earlier drafts. We would also like to acknowledge research assistant Ying Xiong for her assistance in completing the current manuscript. Finally, our greatest thanks go to the many program directors who agreed to participate in this study and gave generously of their time to support the effort.
Author information
Authors and Affiliations
Corresponding author
Additional information
Kathleen Biebel, PhD, is a research instructor at Center for Mental Health Services Research, Department of Psychiatry, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA 01655, USA.
Joanne Nicholson, PhD, is a associate professor of psychiatry and family medicine at Center for Mental Health Services Research, Department of Psychiatry, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA 01655, USA.
Alexis Henry, ScD, OTR/L is a research assistant professor at Center for Health Policy and Research, UMass Medical School- Shrewsbury Campus (Worcester Foundation Campus), 222 Maple Avenue, Higgins Building Shrewsbury, MA 01545.
Judith Katz-Leavy, MEd, is a mental health consultant at 3053 Porter Street NW, Washington, D.C. 20008, USA.
Rights and permissions
About this article
Cite this article
Hinden, B.R., Biebel, K., Nicholson, J. et al. A Survey of Programs for Parents with Mental Illness and their Families: Identifying Common Elements to Build the Evidence Base. JBHSR 33, 21–38 (2006). https://doi.org/10.1007/s11414-005-9007-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11414-005-9007-x