
Abstract
The aim of the study was to determine whether it is possible to improve both maximum and rapid force production using resistance training that is typically used to induce muscle hypertrophy in previously untrained older men. Subjects (60–72 years) performed 20 weeks of “hypertrophic” resistance training twice weekly (n = 27) or control (n = 11). Maximum dynamic and isometric leg press, as well as isometric force over 0–100 ms, and maximum concentric power tests were performed pre- and post-intervention. Muscle activity was assessed during these tests by surface electromyogram of the vastus lateralis and medialis muscles. Muscle hypertrophy was assessed by panoramic ultrasound of the vastus lateralis. The intervention group increased their maximum isometric (from 2268 ± 544 to 2538 ± 701 N) and dynamic force production (from 137 ± 24 to 165 ± 29 kg), and these changes were significantly different to control (isometric 12 ± 16 vs. 1 ± 9 %; dynamic 21 ± 12 vs. 2 ± 4 %). No within- or between-group differences were observed in rapid isometric force or concentric power. Relative increases in vastus lateralis cross-sectional area trended to be statistically greater in the intervention group (10 ± 8 vs. 3 ± 6 %, P = 0.061). It is recommendable that resistance training programs for older individuals integrate protocols emphasizing maximum force/muscle hypertrophy and rapid force production in order to induce comprehensive health-related and functionally important improvements in this population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Healthy aging is associated with a decline in maximum force production at a rate of approx. 1.5 % per year, while decreases of 3.5 % have been observed in rapid force production after the age of 65 (Young and Skelton 1994). Furthermore, age-associated decreases in strength, power, and muscle mass (1) pose a threat to functional capacity (Raj et al. 2010), and (2) adversely affect the ability to prevent certain diseases and/or overcome the deleterious effects of certain treatments (Srikanthan and Karlamangla 2011; Wolfe 2006). Consequently, as a preventative measure to maintain functional capacity, aid in recovery of illness/disease, and preserve independency, it is of interest to improve maximum and rapid force production, as well as muscle mass in older adults. This is typically achieved through resistance training.
Improving both maximum and rapid force production, as well as increasing muscle mass from the same resistance training program, is an attractive model for older adults. Typically, as with all forms of training, resistance training follows the theory of specificity (Campos et al. 2002). Mixed training programs incorporating both heavy/slow and light/fast actions have led to increases in all aspects of force production and muscle mass (Häkkinen et al. 2001; Izquierdo et al. 2001). However, it is unclear what the effects of performing heavy/slow resistance training in isolation, which primarily increases muscle mass and maximum force production (Campos et al. 2002), on rapid force production in older adults will be (Pereira and Gomez 2003).
Previous findings in our laboratory suggest that medium-intensity, high-volume resistance training induces favorable adaptations in muscle activation in older men (Walker et al. 2014; Walker and Häkkinen 2014). These findings were based on increased muscle activity and voluntary action level during maximum force production as measured by surface electromyogram and the interpolated twitch technique (Merton 1954), respectively. As improved rapid force production has been shown to accompany increased rapid muscle activity (Häkkinen et al. 1985), there may be a transfer of gains to rapid force production from improved muscle activation in general.
According to Behm and Sale (1993) and Murray et al. (2007), the important element to increase rapid force production is the intention to produce fast movement. Furthermore, training using rapid isometric actions (where no external movement actually occurs) has led to improved rate of force development accompanied by increased motor unit firing rate (Van Cutsem et al. 1998). These findings would appear to suggest that improving rapid force production during medium-intensity, high-volume resistance training is unlikely, as movements are intentionally performed with relatively slow cadence (approx. 2–4 s in concentric and 2–6 s in eccentric actions) to create a constant mechanical stimulus for muscle growth.
Consequently, the aim of the present study was to determine whether it is possible to improve both maximum and rapid force production using resistance training that is typically used to induce muscle hypertrophy in previously untrained older men. It was hypothesized that the resistance training program would lead to increased maximum force production and muscle hypertrophy but would not induce improved rapid force production.
Methods
Subjects
Thirty-eight older men (age range 60–72) volunteered to participate in the study, 27 were selected to the intervention group (RT) and 11 were selected to the non-training control group (CON). Each subject was carefully informed of the study design and potential risks before the study, after which they provided written consent. The study was conducted according to the Declaration of Helsinki and was approved by the ethical committee of the Central Hospital, Jyväskylä. Subject characteristics at baseline are presented in Table 1. One subject was excluded from final analyses due to unavailability at post-training testing.
The subjects were healthy and physically active, participating in low-intensity exercise such as jogging, cycling, and cross-country skiing but did not have any previous experience with resistance training. Exclusion criteria included cardiovascular diseases, diabetes, musculoskeletal disorders, impaired endocrine function, or taking medication known to influence the neuromuscular or endocrine systems. Prior to measurements, the subjects were examined by a physician including a resting electrocardiogram and were cleared to perform rigorous exercise.
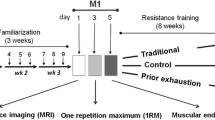
Familiarization session
Subjects visited the laboratory 7 days before their pre-training test measurement. The purpose of this visit was to position all devices to the specified settings for each individual and to locate and mark (by indelible ink tattoo) the electrode locations for electromyography (EMG) recordings. The subjects were given instructions on how to perform each test and allowed approx. five practice trials to become accustomed to the procedures and stabilize their maximum performance. Typically, the subjects’ performance in the familiarization session is approx. 90–95 % of that obtained in the pre-training performance test. The same instructions and performance requirements were followed in the familiarization session as the following performance tests.
Dynamic leg press performance
Bilateral one repetition maximum (1RM) was obtained for the concentric action using a modified leg press device (David 200, David Health Solutions, Helsinki, Finland). The device has been fitted with a linear displacement transducer. Subjects were required to lift the load to a fully extended position (i.e., 180° knee angle) from a starting knee angle of approx. 60°. Subjects performed sets with progressively increasing load in order to prepare for maximal concentric actions. These sets were 10 reps at 70 %, 7 reps at 75 %, 5 reps at 80 %, and 1 rep at 90 % of estimated 1RM. Thereafter, single repetitions using 5 kg increments were performed until the subject could no longer fully extend the hips and legs. Each maximum effort was separated by 1.5 min, and three to four attempts were performed to identify 1RM.
Maximal concentric leg press power using 50 % 1RM load was performed using the same leg press device immediately after the 1RM test. Subjects were instructed to extend the hips and knees “as fast as possible” throughout the range of motion until complete extension (180° knee angle). In-built algorithms identified the point at which the footplate left contact with the feet and the analysis was taken over the starting knee angle plus 5° until the point of contact loss (i.e., 180° knee angle). Maximum concentric power was calculated using a customized script from the known load in kilograms and the linear displacement of the footplate over a period of 50 ms using the following equation: Power = (load × 9.81) × (displacement / time). Three trials were performed separated by 1-min rest. The best trial was used in further analysis.
Isometric leg extension performance
Bilateral isometric leg extension (leg press action) was measured on a custom-built electromechanical dynamometer at a knee angle of 107° and a hip angle of approx. 110°. The subjects were instructed to push “as fast and as hard as possible” and maintain their maximum force production for 3 s while being verbally encouraged. At least three trials were performed and if the third trial was more than 5 % better than the previous trials, a fourth trial was performed. Leg extension force was sampled at 2000 Hz and filtered by a 10-Hz low-pass filter (fourth-order Butterworth) with analysis being performed by a customized script (Signal 4.04, Cambridge Electronic Design, UK). The maximum force was defined as the highest force minus the baseline. Force production over the initial 100 ms was also assessed for rapid isometric force production. The beginning of the force-time curve was defined as the baseline force plus 4 %. Between-trial rest period was 1 min. Performance tests were measured pre-training and 6 days after the last training session to allow full recovery.
Vastus lateralis and medialis EMG measurement and analysis
Bipolar Ag/AgCl electrodes (5-mm diameter, 20-mm inter-electrode distance, common mode rejection ratio >100 dB, input impedance > 100 MΩ, baseline noise <1 μV rms) were positioned following shaving and skin abrasion on the vastus lateralis (VL) and medialis (VM) of the right leg according to SENIAM guidelines (Hermans et al. 1999). Raw EMG signals were sampled at 2000 Hz and amplified at a gain of 500 (sampling bandwidth 10–500 Hz). Raw signals were sent from a hip-mounted pack to a receiving box (Telemyo 2400R, Noraxon, Scottsdale, USA), then were relayed to an AD converter (Micro1401, Cambridge Electronic Design, UK), and recorded by Signal 4.04 software (Cambridge Electronic Design, UK). Offline, EMG signals were band-pass filtered at 20–350 Hz, and root mean square was obtained from 0 to 100 and 500 to 1500 ms during isometric leg extension, as well as from approx. 65° to full leg extension (i.e., 180°) during dynamic leg press actions. The values from the best performance trial were used in further analysis where the data from VL and VM muscles were averaged [(VL + VM) / 2].
Vastus lateralis cross-sectional area
Muscle cross-sectional area (CSA) measurements were taken 1–2 days prior to performance tests and 4–5 days following the last training session to allow any exercise-induced swelling to dissipate. CSA of the VL was assessed by B-mode axial-plane ultrasound (model SSD-α10, Aloka Co Ltd, Tokyo, Japan) using a 10-MHz linear-array probe (60 mm width) with the extended-field-of-view mode (23-Hz sampling frequency). The validity (Ahtiainen et al. 2010) and reliability (Noorkoiv et al. 2010) of this method has been reported. Oriented in the axial-plane, the probe was moved manually with a slow and continuous movement from medial to lateral along a marked line on the skin. Great care was taken to diminish compression of the muscle tissue. Images were obtained throughout the movement. As the orientation of each image relative to adjacent images is known, the software builds a composite image. Three panoramic CSA images were taken at 50 % femur length from the lateral aspect of the distal diaphysis to the greater trochanter, and three images were taken 2 cm distally to this point. CSA was determined by manually tracing along the border of the VL muscle using ImageJ software (version 1.37, National Institute of Health, USA). The mean of the two closest values was taken as the CSA result at each site, and then the mean of these two sites was used for further analysis.
Resistance training program
The intervention group performed whole body resistance training twice per week for a total of 20 weeks, where each session was supervised by a qualified gym instructor. The program was divided into two identical cycles of 10 weeks. Each training session consisted of eight exercises that were performed bilaterally with resistance devices and cable cross-over machines (David Health Solutions, Helsinki, Finland). Lower limb exercises were always performed first and included the leg press, knee extension, and knee flexion exercises. Upper body and torso exercises included bench press, shoulder press, lat pull-down, seated row, biceps curl, triceps pushdown, abdominal crunch, and back raises. Inter-set rest periods were 1 min during weeks 1–4 and then 2 min for weeks 5–10. The subjects were instructed to perform all repetitions in a slow and controlled manner with approx. 2-s concentric and 2-s eccentric actions. All subjects were required to complete 36 out of a total of 40 training sessions prior to post-training testing. The training program for each 10-week cycle is reported in Table 2. Non-training control group subjects maintained their typical physical activities throughout the study.
Statistical analyses
Standardized procedures were used to calculate means, standard deviations, and correlation coefficients. Paired t tests were used to evaluate absolute changes over the study period, while independent t tests were used to assess both absolute values pre- and post-training and relative changes between groups. All statistical methods were performed using IBM SPSS statistics 20 software. Inter-day reliability values for the measurements were 1RM of 0.981 and 3.1 %, concentric power of 0.952 and 5.0 %, isometric leg extension of 0.958 and 6.7 %, and EMGrms of 0.939 and 15.1 % for intra-class correlation coefficient and coefficient of variation, respectively.
Results
Maximum force production
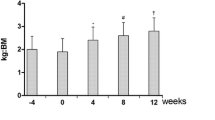
Significant increases were observed in maximum isometric leg extension force (12 ± 16 %, P = 0.002) and leg press 1RM (21 ± 12 %, P < 0.001) in the resistance training group (Fig. 1). No changes were observed in the control group. The relative changes over the study period in maximum force production were significantly different between the training and control group (Fig. 3). Also, the post-training 1RM load was significantly greater in the resistance training group compared to the control group (Fig. 1b).

Maximum isometric (a) and concentric (b) force production pre- and post-intervention and control periods. Significant increases were observed in the intervention group (* = P < 0.05), and the 1RM values were significantly different between the groups post-intervention (P < 0.05)
Rapid force production and power
No changes occurred in isometric force over the initial 100 ms or in maximum power using 50 % of 1RM (Fig. 2). Also, there were no differences between groups in either absolute values or relative changes (Fig. 3).

Rapid isometric force over 100 ms (a) and concentric power (b) pre- and post-intervention and control periods. No within- or between-group differences were observed

Relative changes in maximum and rapid force production during the intervention and control periods. Significant differences were observed between the groups in maximum isometric force and 1RM improvements (P < 0.05). MaxF maximum isometric force, 100 F isometric force over 100 ms, MaxP maximum leg press power
Muscle activity during maximum and rapid force production
Resistance training led to increased muscle activity (VL + VM/2) during maximum isometric leg extension (38 ± 49 %, P = 0.004) and concentric 1RM (107 ± 33 %, P < 0.001) actions, and these increases were greater than in control (Table 3). No changes were observed in the control group in any test.
Over the first 100 ms of isometric leg extension, significant increases in muscle activity (VL + VM/2) were observed in the resistance training group (46 ± 75 %, P = 0.021), but this increase was not different to control. During rapid concentric contractions using 50 % of 1RM, the resistance training group demonstrated increased muscle activity of the VL and VM muscles (11 ± 17 %, P = 0.021) but was not different from control (Table 3).
Vastus lateralis cross-sectional area
The resistance training group increased their VL CSA over the resistance training period (P < 0.001). The relative changes in VL CSA reached the level of a trend between groups (RT = 10 ± 8 % vs. CON = 3 ± 6 %, P = 0.061).
Discussion
In healthy, physically active older men, medium-intensity “hypertrophic” resistance training favored by bodybuilders led to statistically significant increases in maximum leg extensor force production, maximal muscle activity during these actions, and also cross-sectional area of the vastus lateralis muscle. There were no changes in either isometric or concentric rapid force production.
Maximum force production in older adults has been repeatedly shown to be lower than young adults in different muscle groups (McDonaugh et al. 1984; Häkkinen et al. 1998; Kraemer et al. 1999). It has been suggested that age-associated muscle weakness has consequences for function in daily activities, such as walking (van der Krogt et al. 2012) and stair climbing (Holsgaard-Larsen et al. 2011) and prevention of falls (Carty et al. 2012). Therefore, it is of benefit to increase maximum force production in older adults. Since loss of maximum force production occurs at a rate of approx. 5 % per decade following the age of 45 (Aoyagi and Shephard 1992), the ∼21 % increase in maximum concentric force production of the present study represents counteracting ∼20 years of aging.
Since the control group did not demonstrate a significant increase in maximum force production, it can be assumed that one familiarization session was sufficient in ensuring stable performance at baseline in the present study, despite some authors suggesting that multiple sessions may be needed in older adults (Amarante do Nascimento et al. 2013). This enables us to discount learning as a viable factor contributing to improved performance, which has been shown in the absence of training (Kamen and Knight 2004; Knight and Marmon 2008). Also, the magnitude of the improvement in the present study is in-line with those reported previously (Moritani and deVries 1980; Häkkinen et al. 1998, 2001). An ∼21 % increase in 1RM performance represents an increase of approx. 0.5 % per training session, despite the main aim of the training protocol to increase muscle mass and not maximum force production per se. In accordance with expected training specificity, improvements in maximum isometric force production were slightly lower at approx. 0.3 % per training session (∼12 % over the training period). These results show that, although the subjects were healthy and relatively active, robust improvements in maximum force production are achievable during systematic resistance training in older adults. However, it should be noted that inferences to improved functional capacity should not be extrapolated from the present study’s findings as no measures of daily function were taken.
Concomitant increases in surface EMG amplitude were observed during maximum force production in the RT group, and these increases were statistically greater than changes observed in CON. Previously, increased muscle activity (Moritani and deVries 1980; Häkkinen et al. 1998) and voluntary activation level as assessed by interpolated twitch technique (Knight and Kamen 2001; Walker et al. 2014) have been observed in older adults following resistance training. Although one earlier study (Harridge et al. 1999) did not observe improved voluntary activation, there was a significant relationship between improved force production and voluntary activation level. Methodological challenges in these methods have been noted regarding sensitivity to detect changes (Herbert and Gandevia 1999) as well as ability to interpret increased EMG amplitude as evidence of neural adaptation (Farina et al. 2004). Nevertheless, it appears that medium-intensity resistance training is capable of improving maximal muscle activation in older adults, and this is observed quite readily. These findings may be slightly different in young subject, as mixed results regarding the effects of medium-intensity resistance training on muscle activation have been observed (Narici et al. 1989; Häkkinen et al. 1998; Walker et al. 2013; Erskine et al. 2014). Indeed, muscle hypertrophy may be the dominant mechanism for improved maximum force production in the young during this type of training (Walker and Häkkinen 2014) and may indicate a greater potential for neural adaptations (i.e., a sign of neural deficiency) in older adults.
Caution should be used when interpreting increases in surface EMG amplitude. Simulation studies have shown that peripheral factors seem to have a larger effect on the gross EMG signal than neural factors (Arabadzhiev et al. 2014) and that lower amplitude cancellation could account for an increased EMGrms independent to neural drive (Keenan et al. 2006). There is some experimental evidence to suggest that this is possible (Maffiuletti and Martin 2001) due to relatively slow, submaximal load training such as that used in the present study. However, whether the increases in EMG amplitude were due to improved neural activation, the influence of peripheral factors, or both, systematic alterations occurred in the RT group, whereas no changes occurred in CON and this provides evidence for training-induced adaptation.
Rapid force production (i.e., force over the initial 100 ms and maximum concentric power) did not improve during the present study despite training for 20 weeks. Twelve weeks of combined heavy (approx. 80 % volume) and rapid action (approx. 20 % volume) resistance training improved rapid force production in middle-aged and older individuals (Häkkinen and Häkkinen 1995). Using an undulating resistance training program, Newton et al. (2002) observed significant improvements in jump squat performance in older men. Four weeks of rapid pneumatic resistance training with 40 % of MVC induced increased isometric knee extensor performance and EMG amplitude over the initial 200 ms in older men (Piirainen et al. 2014). Furthermore, 8 weeks of fast concentric actions using 35, 55, and 75 % 1RM improved knee extension power in older adults (Henwood and Taaffe 2005). However, improved rapid isometric knee extension torque was not observed by Häkkinen and colleagues (1998) over 10 weeks of training despite containing rapid force production exercises. In older women, rapid force production was improved when using a plyometric training program for 6 weeks and also in a group training with fast concentric actions, but no changes were observed when using a similar resistance training program to the present study (Correa et al. 2012). Overall, it appears that older individuals are capable to achieve increased rapid force production as long as the training program includes rapid actions and that the tests are most specific to the training exercises used (i.e., dynamic versus isometric, similar external load, etc.).
The relatively slow (2 s concentric and 2 s eccentric) actions used in the present study, purportedly beneficial for muscle hypertrophy (Campos et al. 2002; Burd et al. 2012), was perhaps not enough of a stimuli to induce increases in rapid force production. The use of rapid actions in training older individuals may be particularly important for improving functional capacity (Miszko et al. 2003) and should, therefore, be incorporated into the resistance training program along with hypertrophic resistance training. It remains unclear, nevertheless, as to the required amount of rapid actions to induce improved rapid force production and muscle activation. Future studies could focus some attention on whether it is necessary/more beneficial to alternate between hypertrophic and rapid force resistance training periodically or perform these training programs concurrently—i.e., within the same session or using an undulating design.
It is not clear why muscle activity showed statistically significant increases during rapid force production (i.e., 100 ms of isometric leg extension action and during rapid concentric contractions using 50 % of 1RM) in the present study. One explanation could be that the influences of peripheral factors, as discussed above, are apparent in these data. Another partial explanation with regard concentric contraction using 50 % 1RM is that a larger external load was used after the training period, and it has been shown that greater muscle activation is required to overcome inertia (Alkner et al. 2000). It should also be stated that the increases were not significantly different to the control group, whereas the increases during maximum force production reached statistical significance.
One potential weakness of the present study’s rapid force production tests is highlighted by the variance in isometric force over the initial 100 ms (Fig. 3). Whereas maximal force demonstrated stable values, there may be a need to perform multiple baseline tests to ensure stable rapid force production in the elderly. The reduced SD during the study (∼240 N pre- vs. ∼160 N post-intervention) along with the increase in the lower bound 95 % confidence interval (∼240 N pre- vs. ∼390 N post-intervention) suggest that learning or perhaps also a reduction in fear to produce isometric force rapidly in the subjects of the present study occurred during testing. Furthermore, the variance in performance demonstrated by the control group (Δ% range −22 to 66) suggests that this variable may not be sensitive to detect changes over time—although the test-retest reliability of this variable was acceptable. Therefore, it is suggested that future studies assess these possible weaknesses by performing multiple familiarization sessions and assessing different time windows for rapid force development in this age group (e.g., 0–100 vs. 0–200 ms). Nevertheless, the results obtained should be considered valid since the present study utilized two measures of rapid force production, both showing no improvement due to training, and that the sample size used in the present study was sufficient for statistical power (required n = 5–14 for 0.80 power).
The present study’s resistance training protocol was successful in promoting muscle hypertrophy as determined by VL CSA. This data supports previous findings that older adults are capable of achieving muscle hypertrophy due to resistance training (Moritani and deVries 1980; Häkkinen and Häkkinen 1995; Häkkinen et al. 1998; Kraemer et al. 1999; Mayhew et al. 2009). Muscle hypertrophy may also have contributed to the observed improvements in maximum force production since a large component of maximum force has been shown to be related to muscle size (Maughan et al. 1983). Increased muscle size is an important adaptation to resistance training, particularly for older adults, to prevent the age-associated loss in muscle mass (Aoyagi and Shephard 1992) and the proposed loss in muscle function (Raj et al. 2010) that accompanies sarcopenia. Therefore, the resistance training-induced hypertrophy of the present study represents a partial reversal of the aging processes experienced over the past few years by these subjects. Furthermore, maintenance of muscle mass may well be positive to maintain normal metabolic functioning (Dela and Kjaer 2006), as well as healthy body composition, and provide benefit if the individual was to suffer deleterious (treatment of) disease (Wolfe 2006).
One limitation of the muscle hypertrophy measurement used in the present study was that only one quadriceps muscle was quantified and at only one point along the muscle length. While this may not fully describe the phenomena related to the present study’s training protocol, large differences in CSA growth between quadriceps muscles would seem unlikely (Häkkinen et al. 1998). Furthermore, since it was not the intention of the present study to quantify muscle hypertrophy per se, it may be considered sufficient to demonstrate that resistance training led to increased CSA in the trained muscles, while normal daily activities performed by the control group did not.
The training program was twice per week in accordance with recommendations for this age group (World Health Organization 2010 p. 31), and all muscle groups were trained during each session. Furthermore, resistance machines were used for all exercises, with exception of some trunk exercises, and the training loads were progressively increased from 60 to 85 % 1RM during each 10-week training period as recommended by the American College of Sports Medicine (Garber et al. 2011) for beginners. Also, the number of sets performed for each exercise was increased from 2 to 5 depending on the exercise (see Table 2). This type of resistance training is favored by bodybuilders whose aim is to increase muscle mass. The training program was well tolerated by the subjects, who were healthy and free from cardiovascular or joint diseases, with no incidences of injury due to training reported.
Conclusions
The present study did not observe training-induced improvements in rapid force production, which likely provides benefit in older adults in maintaining muscle function and prevention against falls. However, the resistance training-induced adaptations during the present study’s medium-intensity, high-volume protocol were specific to increased maximum force production accompanied by increased muscle activity and vastus lateralis cross-sectional area. Therefore, it is recommendable that resistance training programs for older individuals alternate between protocols emphasizing maximum force/muscle hypertrophy and rapid force production periodically in order to induce health-related and functionally important improvements in this target population.
References
Ahtiainen JP, Hoffren M, Hulmi JJ, Pietikäinen M, Mero AA, Avela J, Häkkinen K (2010) Panoramic ultrasonography is a valid method to measure changes in skeletal muscle cross-sectional area. Eur J Appl Physiol 108:273–279
Alkner BA, Tesch PA, Berg HE (2000) Quadriceps EMG/force relationship in knee extension and leg press. Med Sci Sports Exerc 32:459–463
Amarante do Nascimento M, Januario RS, Gerage AM, Mayhew JL, Cheche Pina FL, Cyrino ES (2013) Familiarization and reliability of one repetition maximum strength testing in older women. J Strength Cond Res 27:1636–1642
Aoyagi Y, Shephard RJ (1992) Aging and muscle function. Sports Med 14:376–396
Arabadzhiev TI, Dimitrov VG, Dimitrov GV (2014) The increase in surface EMG could be a misleading measure of neural adapatation during the early gains in strength. Eur J Appl Physiol 114:1645–1655
Burd NA, Andrews RJ, West DW, Little JP, Cochran AJ, Hector AJ, Cashaback JG, Gibala MJ, Potvin JR, Baker SK, Phillips SM (2012) Muscle time under tension during resistance exercise stimulates differential muscle protein sub-fractional synthetic responses in men. J Physiol 590:351–362
Campos GE, Luecke TJ, Wendeln HK et al (2002) Muscular adaptations in response to three different resistance-training regimens: specificity of repetition maximum training zones. Eur J Appl Physiol 88:50–60
Carty CP, Barrett RS, Cronin NJ, Lichtwark GA, Mills PM (2012) Lowerlimb muscle weakness predicts use of a multiple- versus single-step strategy to recovery from forward loss of balance in older adults. J Gerontol A Biol Sci Med Sci 67:1246–1252
Correa CS, Baroni BM, Radaelli R, Lanferdini FJ, Cunha Gdos S, Reischak-Oliveira A, Vaz MA, Pinto RS (2012) Effects of strength training and detraining on knee extensor strength, muscle volume and muscle quality in elderly women. Age 35:1899–1904
Dela F, Kjaer M (2006) Resistance training, insulin sensitivity and muscle function in the elderly. Essays Biochem 42:75–88
Erskine RM, Fletcher G, Folland JP (2014) The contribution of muscle hypertrophy to strength changes following resistance training. Eur J Appl Physiol 114:1239–1249
Farina D, Merletti R, Enoka RM (2004) The extraction of neural strategies from the surface EMG. J Appl Physiol 96:1486–1495
Garber CE, Blissmer B, Deschennes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP (2011) American College of Sports Medicine position stand. quantity and quality of exercise for developing and maintaining cardiorespiratory, musculskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43:1334–1359
Häkkinen K, Häkkinen A (1995) Neuromuscular adaptations during intensive strength training in middle-aged and elderly males and females. Electromyogr Clin Neurophysiol 35:137–147
Häkkinen K, Komi PV, Alen M (1985) Effect of explosive type strength training on isometric force- and relaxation-time, electromyographic and muscle fibre characteristics of leg extensor muscles. Acta Physiol Scand 125:587–600
Häkkinen K, Newton RU, Gordon SE et al (1998) Changes in muscle morphology, electromyographic activity, and force production characteristics during progressive strength training in young and older men. J Gerontol A Biol Sci Med Sci 53:B415–B423
Häkkinen K, Kraemer WJ, Newton RU, Alen M (2001) Changes in electromyographic activity, muscle fibre and force production characteristics during heavy resistance/power strength training in middle-aged and older men and women. Acta Physiol Scand 171:51–62
Harridge SD, Kryger A, Stensgaard A (1999) Knee extensor strength, activation, and size in very elderly people following strength training. Muscle Nerve 22:831–839
Henwood TR, Taaffe DR (2005) Improved physical performance in older adults undertaking a short-term programme of high-velocity resistance training. Gerontology 51:108–115
Herbert RD, Gandevia SC (1999) Twitch interpolation in human muscles: mechanisms and implications for measurement of voluntary activation. J Neurophysiol 82:2271–2283
Hermens HJ, Freriks B, Merletti R, Stegeman D, Blok J, Rau G, Disselhorst-Klug C (1999) European recommendations for surface electromyography: result of the SENIAM project. Roessingh Research and Development, Enschede
Holsgaard-Larsen A, Caserotti P, Puggaard L, Aagaard P (2011) Stair-ascent performance in elederly women: effect of explosive strength training. J Aging Phys Act 19:117–136
Izquierdo M, Häkkinen K, Ibanez J, Garrues M, Anton A, Zuniga A, Larrion JL, Gorostiaga EM (2001) Effects of strength training on muscle power and serum hormones in middle-aged and older men. J Appl Physiol 90:1497–1507
Kamen G, Knight CA (2004) Training-related adaptations in motor unit discharge rate in young and older adults. J Gerontol A Biol Sci Med Sci 59:1334–1338
Keenan KG, Farina D, Merletti R, Enoka RM (2006) Amplitude cancellation reduces the size of motor unit potentials averaged from the surface EMG. J Appl Physiol 100:1928–1937
Knight CA, Kamen G (2001) Adaptations in muscular activation of the knee extensor muscles with strength training in young and older adults. J Electromyogr Kinesiol 11:405–412
Knight CA, Marmon AR (2008) Neural training for quick strength gains in the elderly: strength as a learned skill. J Strength Cond Res 22:1869–1875
Kraemer WJ, Häkkinen K, Newton RU et al (1999) Effects of heavy-resistance training on hormonal response patterns in younger vs older men. J Appl Physiol 87:982–992
Maffiuletti NA, Martin A (2001) Progressive versus rapid rate of contraction during 7 wk of isometric resistance training. Med Sci Sports Exerc 33:1220–1227
Maughan RJ, Watson JS, Weir J (1983) Strength and cross-sectional area of human skeletal muscle. J Physiol 338:37–49
Mayhew DL, Kim JS, Cross JM, Ferrando AA, Bamman MM (2009) Translational signalling responses preceding resistance training-mediated myofiber hypertrophy in young and old humans. J Appl Physiol 107:1655–1662
McDonaugh MJ, White MJ, Davies CT (1984) Different effects of ageing on the mechanical properties of human arm and leg muscles. Gerontology 30:49–54
Merton PA (1954) Voluntary strength and fatigue. J Physiol 123:553–564
Miszko TA, Cress ME, Slade JM, Covey CJ, Agrawal SK, Doerr CE (2003) Effect of strength and power training on physical function in community-dwelling older adults. J Gerontol A Biol Sci Med Sci 58:171–175
Moritani T, deVries HA (1980) Potential for gross muscle hypertrophy in older men. J Gerontol 35:672–682
Narici MV, Roi GS, Landoni L, Minetti AE, Cerretelli P (1989) Changes in force, cross-sectional area and neural activation during strength training and detraining of the human quadriceps. Eur J Appl Physiol Occup Physiol 59:310–319
Newton RU, Häkkinen K, Häkkinen A, McCormick M, Volek J, Kraemer WJ (2002) Mixed-methods resistance training increases power and strength of young and older men. Med Sci Sports Exerc 34:1367–1375
Noorkoiv M, Nosaka K, Balzevich AJ (2010) Assessment of quadriceps muscle cross-sectional area by ultrasound extended-field-of-view imaging. Eur J Appl Physiol 109:631–639
Pereira MI, Gomez PS (2003) Movement velocity in resistance training. Sports Med 33:427–438
Piirainen JM, Cronin NJ, Avela J, Linnamo V (2014) Effects of plyometric and pneumatic explosive strength training on neuromuscular function and dynamic balance control in 60–70 year old males. J Electromyogr Kinesiol 24:246–252
Raj IS, Bird SR, Shield AJ (2010) Aging and the force-velocity relationship of muscles. Exp Gerotol 45:81–90
Van Cutsem M, Duchateau J, Hainaut K (1998) Changes in single motor unit behavior contribute to the increase in contraction speed after dynamic training in humans. J Physiol 513:295–305
Van der Krogt MM, Delp SL, Schwartz MH (2012) How robust is human gait to muscle weakness? Gait Post 36:113–119
Walker S, Häkkinen K (2014) Similar increases in strength after short-term resistance training due to different neuromuscular adaptations in young and older men. J Strength Cond Res 28:3041–3048
Walker S, Hulmi JJ, Wernbom M, Nyman K, Kraemer WJ, Ahtiainen JP, Häkkinen K (2013) Variable resistance training promotes greater fatigue resistance but not hypertrophy versus constant resistance training. Eur J Appl Physiol 113:2233–2244
Walker S, Peltonen H, Sautel J, Scaramella C, Kraemer WJ, Avela J, Häkkinen K (2014) Neuromuscular adaptations to constant vs. variable resistance training in older men. Int J Sports Med 35:69–74
World Health Organization (2010) Global recommendations on physical activity for health. http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf?ua=1. Accessed January 22 2015
Acknowledgments
The authors would like to thank the contribution of Mrs. Pirkko Puttonen, as well as the dedication and effort of the subjects.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Walker, S., Peltonen, H. & Häkkinen, K. Medium-intensity, high-volume “hypertrophic” resistance training did not induce improvements in rapid force production in healthy older men. AGE 37, 41 (2015). https://doi.org/10.1007/s11357-015-9786-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11357-015-9786-9