
Abstract
The aim of this study is to investigate whether work-related stress symptoms in midlife are associated with a number of mobility limitations during three decades from midlife to late life. Data for the study come from the Finnish Longitudinal Study of Municipal Employees (FLAME). The study includes a total of 5429 public sector employees aged 44–58 years at baseline who had information available on work-related stress symptoms in 1981 and 1985 and mobility limitation score during the subsequent 28-year follow-up. Four midlife work-related stress profiles were identified: negative reactions to work and depressiveness, perceived decrease in cognition, sleep disturbances, and somatic symptoms. People with a high number of stress symptoms in 1981 and 1985 were categorized as having constant stress. The number of self-reported mobility limitations was computed based on an eight-item list of mobility tasks presented to the participants in 1992, 1997, and 2009. Data were analyzed using joint Poisson regression models. The study showed that depending on the stress profile, persons suffering from constant stress in midlife had a higher risk of 30–70 % for having one more mobility limitation during the following 28 years compared to persons without stress after adjusting for mortality, several lifestyle factors, and chronic conditions. A less pronounced risk increase (20–40 %) was observed for persons with occasional symptoms. The study suggests that effective interventions aiming to reduce work-related stress should focus on both primary and secondary prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mobility refers to a person’s self-reported or observed ability to move independently from one place to another within the environment (Shumway-Cook et al. 2005). In the International Classification of Functioning, Disability and Health (ICF), components of mobility include walking and moving; changing and maintaining body position; carrying, moving, and handling objects; and moving around using transportation (World Health Organisation 2001). Mobility declines with increasing age, and both intrapersonal and environmental risk factors for incident mobility limitations have been identified, including chronic diseases, physical inactivity, poor muscle strength, sensory impairments, and indoor and outdoor environment (Brown and Flood 2013; Rantakokko et al. 2013; Yeom et al. 2008). Also, psychosocial symptoms, such as depression earlier in life (Hybels et al. 2009) and lower social participation (Avlund et al. 2004), are linked to old age mobility limitations. However, longitudinal studies investigate the relation between stress-related symptoms present already in midlife and incident mobility limitations are still lacking.
Stress related to work can be defined as a “pattern of physiological, emotional, cognitive and behavioral reactions to some extremely taxing aspects of work content, work organization and work environment” (Houtman et al. 2007). Work-related stress is a common experience among middle-aged people with an estimated prevalence of nearly 30 % among adult workers in Europe (Houdmont et al. 2010). It is known that low job control, high job demands, and low work-related social support, which are common causes of stress (Nieuwenhuijsen et al. 2010), are cross-sectionally associated with poor health status and also predict subsequent functional decline (Cheng et al. 2000; Wahrendorf et al. 2012). Also, several musculoskeletal complaints are cross-sectionally linked to perceived low co-worker support, low job control, and role conflicts at the work place, which are acknowledged risk factors for stress (Eatough et al. 2012; Mehta and Parijat 2012; Toivanen 2011).
We have previously shown that stress symptoms in midlife predict self-care disability (ADL) and instrumental activities of daily living (IADL) disability in old age (Kulmala et al. 2013). Some other prospective studies have reported significant associations between psychosocial stressors and development of musculoskeletal problems, but the follow-up periods in those studies have been relatively short (Kraatz et al. 2013; Lang et al. 2012). Previous studies with follow-up periods of 10 years or more have suggested that work-related stress (Brage et al. 2007), low job control (Kaila-Kangas et al. 2004), and mental overstrain (Leino and Hänninen 1995) may lead to musculoskeletal pain and hospitalization, sickness absence, rehabilitation, or disability pension due to musculoskeletal disorders. Still, there are no studies investigating the effect of midlife work-related stress on mobility outcomes using a follow-up period extending up to several decades. Further, the unavailability of intermediate time points in previous studies has not allowed the researchers to take into account the loss to follow-up, for example, due to mortality potentially leading to underestimation of the predictive power of the independent variable. This study fills this gap by investigating work-related stress symptoms in midlife and their association to the number of mobility limitations at the latest available measure during the 28-year follow-up. In this study, we aim to take into account several lifestyle factors and mortality as a competing risk for mobility decline. As mobility limitations usually precede incident disability, we hypothesize that in the pathway from work-related stress to severe old age, disability mobility limitations may be an intermediate and potentially preventable phase.
Methods
Participants
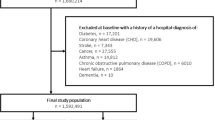
The data for this study come from the Finnish Longitudinal Study on Municipal Employees (FLAME), which was initiated by the Finnish Institute of Occupational Health and targeted 7344 individuals aged 44–58 years at baseline in 1981. Four-year follow-up data were collected in 1985 (n = 5556) (Ilmarinen et al. 1991; Tuomi et al. 1997; von Bonsdorff et al. 2011). The study population includes 5429 persons (3108 women and 2321 men) who had information available on work-related stress symptoms in 1981 and 1985 and a number of mobility limitations during the follow-up (74 % of target population). The study was approved by the Ethical Committee of the Finnish Institute of Occupational Health, and the research was conducted in accordance with the Helsinki Declaration.
Measures
Work-related stress symptoms
Work-related stress symptoms were assessed with postal questionnaires at baseline in 1981 and 4 years later in 1985 (Elo et al. 1992; Huuhtanen et al. 1997; Kulmala et al. 2013). The participants were informed that the purpose of the FLAME study was to assess health, work ability, and working conditions, and they were advised to consider their responses from this perspective. The stress questionnaire used in this study was constructed for the present study by a panel of occupational health experts at the Finnish Institute of Occupational Health using the best knowledge available in the late 1970s and early 1980s when the study was launched. We have previously reported the analytical process underlying the identification of the four midlife stress profiles in detail (Kulmala et al. 2013). Briefly, negative reactions to work and depressiveness included self-reported urge to stay home instead of going to work, lack of energy and vitality, inability to enjoy daily life, inclination to be off work without reason, general reluctance, gloomy outlook for the future, and depression (each symptom was measured using five-point Likert-type scale (range 0–4), total range in this profile 0–28 with higher scores indicating more stress). Perceived decrease in cognition included difficulty remembering, remembering that requires effort, and blackouts (range 0–12). Sleep disturbances included difficulty falling asleep, several awakenings during the night, and difficulty falling asleep after awakenings (range 0–12). Somatic symptoms included chest pain, stomachache, and dizziness (range 0–12). Persons with a stress score in the lowest tertile in 1981 and 1985 were categorized as having no stress. Those whose score was in the highest tertile in both 1981 and 1985 were categorized as having constant stress, while all others were considered to have occasional stress.
Mobility and mortality
Mobility limitations were assessed by self-reported questionnaires in 1992, 1997, and 2009. The participants’ latest available measure was used in the analyses. In the International Classification of Functioning, Disability and Health (ICF), “activities and participation” component, the “mobility” chapter includes four sets of categories: walking and moving; changing and maintaining body position; carrying, moving, and handling objects; and moving around using transportation. The eight mobility questions in this study covered three of these four sets of categories. Walking and moving included information on walking 2 km, running 100 m, and climbing three flights of stairs; changing and maintaining body position included information on squatting down and standing up again and bending down deep (e.g., to reach the feet); and carrying, moving, and handling objects included information on lifting and carrying heavy loads of more than 10 kg, performing precise movements with hands and fingers (e.g., potato peeling, using a screwdriver) and lifting hands over the head. Data were collected on the levels of difficulty encountered while performing the respective activity. If participants reported to have “no difficulty,” they scored 0, and if they reported to have at least “some difficulty,” they scored 1 in the respective item. A summary score was then calculated, ranging from 0 (no difficulty in any activity) to 8 (at least some difficulties in all activities) (Hinrichs et al. 2014). This score does not include any grading of severity within the single items, but the simplicity of counting the number of difficulties has proven its worth in a number of previous studies on functional limitations (Lawrence and Jette 1996; Lee et al. 2012; Netuveli et al. 2006). The cohort was followed for mortality between 1 January 1985 and 31 July 2009. Mortality data were received from the Finnish National Population Register. Table 1 shows the mobility limitation data available for each follow-up.
Baseline covariates
Data on baseline covariates were collected using a self-report questionnaire in 1981. Leisure time physical activity during the previous year was categorized into the following levels: inactive, moderate (at least some form of exercise once or less a week), and vigorous (brisk exercise once or more a week). Occupational status (blue-collar, e.g., maintenance work, home care, cleaning, nursing assistant; lower white-collar, e.g., transport work, dental care, nursing; and upper white-collar, e.g., administrator, physician, teacher) was defined as the participants’ position of employment at baseline (Ilmarinen et al. 1991). Net family income was categorized into ≤3400 vs. >3400 Finnish markka (∼570 €). Also, elicited at baseline were alcohol consumption (never, once or twice a month, once or more per week) and smoking (never smoked, former or current smoker). Self-reported chronic conditions included physician-diagnosed musculoskeletal diseases (e.g., arthritis, degenerative diseases of the back and extremities), heart and circulatory diseases (e.g., hypertension and angina pectoris), respiratory diseases (e.g., chronic obstructive pulmonary disease and asthma), cancer, and diabetes. Chronic conditions included also obesity, which was defined as a body mass index (BMI) of ≥30 kg/m2.
Statistical analysis
Baseline characteristics of men and women are reported in mean values and standard deviations for continuous variables and percentage distributions for categorical variables. Statistical differences were tested with independent samples t test for continuous variables and chi-square tests for categorical variables. Descriptive statistics were computed in SPSS Statistics for Windows Version 19.0 (IMB Corp., Armonk, NY, USA).
Survival time was calculated as the interval (number of days) from 1985 examination to death or final follow-up. The mixed Poisson model was used for the outcomes of mobility and mortality, where a random effect U adjusts for the frailty-type dependency between the two outcomes. We can write the logarithm of mobility limitation risk and mortality hazard, respectively, as
where γ are the vectors of regression coefficients for the mobility limitation outcome and β is the vector of mortality risk regression coefficient. We assumed the random effect to be normally distributed with mean zero and variance estimated from data. In model 1, the mobility outcome was adjusted for age, and the hazard component was not included. We included the hazard component in model 2 to address the competing risk of mortality for mobility limitations, both of which were adjusted for leisure-time physical activity, occupational class, income, smoking, alcohol consumption, and chronic diseases. We report model effects as incidence rate ratios (IRRs) with 95 % confidence intervals (CIs) using no symptoms as the reference. The model parameters were estimated in Mplus Version 7 (Muthen & Muthen, Los Angeles, CA, USA).
Results
Participants’ age at baseline ranged from 44 to 58 years with a mean age of 50.4 (SD 3.6), and 57.2 % were women. Baseline characteristics for men and women are reported in Table 1. The proportion of participants reporting no stress in midlife ranged between 21.3 and 31.2 %, while the proportion of those with constant stress ranged between 13.4 and 23.3 %, depending on gender and the stress profile. Women reported to have less constant symptoms in perceived decrease in cognition (p < 0.001) but more sleep disturbances (p = 0.011) than men. Minor gender differences were also observed in negative reactions to work and depressiveness (p = 0.033) (Table 2).
The mean follow-up time was 9453 days. The latest available mobility data, ascertained in 1992, 1997, or 2009, were used for analyses. Incident rate of mobility limitation (number of limitations per 1000 person-years) for all participants was 0.433, men 0.438 and women 0.430.
Of the 5429 persons in this study, 30.1 % (1632 persons) died during the follow-up. Those who died were older at baseline (mean 51.5, SD 3.6, vs. mean 49.9, SD 3.4; p < 0.001), more often men (58.7 vs. 35.9 %, p < 0.001), current or former smokers (58.7 vs. 36.6 %, p < 0.001), blue-collars (56.9 vs. 38.5 %, p < 0.001), and more likely to be physically inactive (10.5 vs. 6.7 %, p < 0.001) and had more chronic diseases compared to the survivors. Persons who died also reported to have more constant stress in midlife.
Work-related stress in midlife predicted a higher number of mobility limitations during the follow-up, presented in Table 3. Men and women who suffered from occasional stress in midlife had 20–40 % higher age-adjusted IRR for each unit increase in the mobility limitation score compared to participants with no stress, depending on the stress profile. Constant stress increased the age-adjusted IRR for mobility limitation by 40–100 % in men and 50–70 % in women, depending on the profile. The highest age-adjusted IRR for mobility limitation was observed among men and women, who had suffered from constant somatic symptoms in midlife. When the models were additionally adjusted for leisure-time physical activity, occupational class, income, smoking, alcohol consumption, and chronic diseases and the model also included the hazard component to address mortality as a competing risk for mobility limitations, the IRRs did not significantly change. The associations between all types of constant work-related stress in midlife and mobility limitation in old age remained statistically significant (Table 2). In joint Poisson regression models, where mobility, lifestyle factors, and comorbidities were taken into account, stress did not predict higher mortality in men or in women.
For 253 men and 411 women, the latest available measure of mobility limitation score was found to be lower than that at some earlier point during the follow-up, meaning that they had suffered from more severe mobility difficulties during the follow-up but then subsequently recovered. To investigate the effect of this on the results, we conducted sensitivity analyses excluding these persons. There were no significant changes in the estimates (results not shown).
Discussion
This study showed that work stress in midlife is associated with an increased risk of mobility limitation during the following three decades. The highest risks for subsequent mobility limitations were found for men and women, who reported to have constant negative reactions to work and depressiveness or constant somatic symptoms in midlife. All investigated associations were significant for both men and women. Work-related stress was not associated with higher mortality when chronic conditions, mobility, and several lifestyle factors were taken into account.
Previously, we have shown that stress symptoms in midlife increased the likelihood of difficulties in basic activities in daily living as well as in more demanding instrumental activities of daily living and walking 2 km (Kulmala et al. 2013). The present study is in concordance with these previous associations and further expands the knowledge about the adverse effects of stress on old age physical functioning and mobility.
Although several studies have reported that work-related mental stress is associated with poor health and musculoskeletal complaints in cross-sectional studies (Barzideh et al. 2013; Sembajwe et al. 2013), longitudinal studies using mobility-related outcomes are scarce. It has been shown that high job demands, low job control and social support, as well as job strain are associated with the development of neck and/or shoulder disorders (Kraatz et al. 2013). Additionally, psychosocial stressors have significant effects on the development of musculoskeletal problems in longitudinal studies with follow-ups ranging from 1 to almost 30 years (Lang et al. 2012). However, to the best of our knowledge, this is the first study reporting on work-related stress in midlife in relation to mobility limitations over the following three decades.
Several mechanisms may explain the association between stress and incident mobility limitations. Mental stress causes neuromuscular tension and correlates with musculoskeletal complaints, such as pain (Kopec and Sayre 2004). In cross-sectional studies, perceived pain was found to be associated with poorer physical functioning (Lihavainen et al. 2010), and perceived pain also predicts subsequent disabilities (Hughes et al. 1994). Stress is also associated with cardiovascular risk factors, such as higher smoking rates and metabolic indicators including higher blood cholesterol and glucose levels (Vrijkotte et al. 1999), and thus consequently with incident cardiovascular disease (Greenwood et al. 1996) and diabetes (Nyberg et al. 2013). These chronic conditions significantly influence mobility (Brown and Flood 2013). Also, higher inflammation levels and impaired immunity functions have been observed among stressed individuals (Emeny et al. 2013). Inflammation may predispose to subsequent mobility limitations, for example, through its adverse effects on the cardiovascular system (Emeny et al. 2013).
Stress has also been linked to several adverse health behaviors (Lallukka et al. 2008; Nyberg et al. 2013). Besides the previously mentioned higher smoking rates, it has been reported that persons suffering from work-related stress are physically less active and more frequently obese compared to non-stressed persons (Nyberg et al. 2013). The association between midlife obesity and old age mobility limitations, mainly due to joint degeneration and pain, is well acknowledged (Vincent et al. 2010). Also, dietary factors may mediate the association, since stress may be associated with an unhealthier diet (Ng and Jeffery 2003), which is a risk factor for mobility limitations (Milaneschi et al. 2010). Although we adjusted the analyses for several chronic conditions and lifestyle factors, we cannot completely rule out the possibility that other unfavorable lifestyle factors not measured in this study, including other aspects of socioeconomic status, dietary factors, or others, may partly explain the association. Thus, the mechanisms explaining the association observed in the present study warrant further investigation.
The association between work-related stress and all-cause mortality was not significant after adjusting for several confounding factors. Similar results have been presented by Hange et al. (2013) who did not find a relationship between stress and mortality in a 37-year follow-up, although contrasting results have been presented (Ahola et al. 2010). Although our results suggested that constant perceived decrease in cognition was associated with lower mortality, these estimates should be interpreted cautiously due to a limited number of participants in the subgroups.
Strengths of this study include a large study population and follow-up period extending up to nearly 30 years. We were also able to identify persons with occasional and constant stress, which provided additional information about a dose–response association between work-related stress and mobility limitations in old age. We had detailed information on mobility ascertained at several time points, and the latest available measurement was used in the analyses. This significantly diminished the dropout rate. Although dropout was small, it may have affected the results, since persons with poor health and more stress at baseline dropped out of the study before the second baseline measurement point in 1985. This could have resulted in a healthy worker effect, meaning that those who remain in the profession, and also in the study, tend to be healthier than those who dropped out, consequently causing underestimation of the risks (Shah 2009). After the retirement of the participants, work-related stress questions were modified since the participants were no longer occupationally active. Therefore, we were unable to take into account their subsequent stress levels in the analyses. Long-term stress may start a process of health deterioration, which later manifests in mobility limitations, but we cannot completely rule out the possibility that similar symptoms after retirement caused by other than work-related factors may directly relate to functional limitations. Another limitation of the present study is that data on mobility limitations were not available at baseline, and we cannot rule out that some participants had some mobility limitation at baseline. We do not believe that this would have influenced the results markedly, because all participants were occupationally active at baseline and most probably had only a minimal level on mobility limitations. We also adjusted the analyses for baseline variables which correlate with mobility, including leisure-time physical activity, occupational class, income, smoking, alcohol consumption, and chronic diseases.
This study provided further information on the longitudinal adverse effects of work-related stress in midlife on later health and functioning. Both occasional and constant work-related stress was strongly associated with incident mobility limitations, which is a vital factor in active aging. Preventing work-related stress may lead to more healthy and independent old age, which is preferable not only for the individual but also for the society. Effective interventions aiming to address this problem should focus on both primary and secondary prevention of work stress.
References
Ahola K, Väänänen A, Koskinen A, Kouvonen A, Shirom A (2010) Burnout as a predictor of all-cause mortality among industrial employees: a 10-year prospective register-linkage study. J Psychosom Res 69:51–57
Avlund K, Lund R, Holstein BE, Due P (2004) Social relations as determinant of onset of disability in aging. Arch Gerontol Geriatr 38:85–99
Barzideh M, Choobineh AR, Tabatabaee HR (2013) Job stress dimensions and their relationship to musculoskeletal disorders in Iranian nurses. Work. doi:10.3233/WOR-121585
Brage S, Sandanger I, Nygard JF (2007) Emotional distress as a predictor for low back disability: a prospective 12-year population-based study. Spine (Phila Pa 1976) 32:269–274
Brown CJ, Flood KL (2013) Mobility limitation in the older patient: a clinical review. JAMA 310:1168–1177
Cheng Y, Kawachi I, Coakley EH, Schwartz J, Colditz G (2000) Association between psychosocial work characteristics and health functioning in American women: prospective study. BMJ 320:1432–1436
Eatough EM, Way JD, Chang CH (2012) Understanding the link between psychosocial work stressors and work-related musculoskeletal complaints. Appl Ergon 43:554–563
Elo A, Leppänen A, Lindstrom K, Ropponen T (1992) Occupational stress questionnaire: user’s instructions. Review 19. Finnish Institute of Occupational Health, Helsinki
Emeny RT, Zierer A, Lacruz ME, Baumert J, Herder C, Gornitzka G, Koenig W, Thorand B, Ladwig KH, KORA Investigators (2013) Job strain-associated inflammatory burden and long-term risk of coronary events: findings from the MONICA/KORA Augsburg case-cohort study. Psychosom Med 75:317–325
Greenwood DC, Muir KR, Packham CJ, Madeley RJ (1996) Coronary heart disease: a review of the role of psychosocial stress and social support. J Public Health Med 18:221–231
Hange D, Mehlig K, Lissner L, Guo X, Bengtsson C, Skoog I, Bjorkelund C (2013) Perceived mental stress in women associated with psychosomatic symptoms, but not mortality: observations from the population study of women in Gothenburg, Sweden. Int J Gen Med 6:307–315
Hinrichs T, von Bonsdorff MB, Törmäkangas T, von Bonsdorff ME, Kulmala J, Seitsamo J, Nygård CH, Ilmarinen J, Rantanen T (2014) Inverse effects of midlife occupational and leisure time physical activity on mobility limitation in old age-a 28-year prospective follow-up study. J Am Geriatr Soc. doi:10.1111/jgs.12793
Houdmont J, Cox T, Griffiths A (2010) Work-related stress case definitions and prevalence rates in national surveys. Occup Med (Lond) 60:658–661
Houtman IL, Jettinghoff K, Cedillo L (2007) Raising awareness of stress in developing countries: a modern hazard in a traditional working environment. Protecting Workers’ Health Series no. 6. WHO, Geneva
Hughes SL, Dunlop D, Edelman P, Chang RW, Singer RH (1994) Impact of joint impairment on longitudinal disability in elderly persons. J Gerontol 49:S291–S300
Huuhtanen P, Nygård CH, Tuomi K, Martikainen R (1997) Changes in stress symptoms and their relationship to changes at work in 1981–1992 among elderly workers in municipal occupations. Scand J Work Environ Health 23(Suppl 1):36–48
Hybels CF, Pieper CF, Blazer DG (2009) The complex relationship between depressive symptoms and functional limitations in community-dwelling older adults: the impact of subthreshold depression. Psychol Med 39:1677–1688
Ilmarinen J, Suurnäkki T, Nygård CH, Landau K (1991) Classification of municipal occupations. Scand J Work Environ Health 17(Suppl 1):12–29
Kaila-Kangas L, Kivimäki M, Riihimäki H, Luukkonen R, Kirjonen J, Leino-Arjas P (2004) Psychosocial factors at work as predictors of hospitalization for back disorders: a 28-year follow-up of industrial employees. Spine (Phila Pa 1976) 29:1823–1830
Kopec JA, Sayre EC (2004) Work-related psychosocial factors and chronic pain: a prospective cohort study in Canadian workers. J Occup Environ Med 46:1263–1271
Kraatz S, Lang J, Kraus T, Munster E, Ochsmann E (2013) The incremental effect of psychosocial workplace factors on the development of neck and shoulder disorders: a systematic review of longitudinal studies. Int Arch Occup Environ Health 86:375–395
Kulmala J, von Bonsdorff MB, Stenholm S, Törmäkangas T, von Bonsdorff ME, Nygård CH, Klockars M, Seitsamo J, Ilmarinen J, Rantanen T (2013) Perceived stress symptoms in midlife predict disability in old age: a 28-year prospective cohort study. J Gerontol A Biol Sci Med Sci 68:984–991
Lallukka T, Lahelma E, Rahkonen O, Roos E, Laaksonen E, Martikainen P, Head J, Brunner E, Mosdol A, Marmot M, Sekine M, Nasermoaddeli A, Kagamimori S (2008) Associations of job strain and working overtime with adverse health behaviors and obesity: evidence from the Whitehall II Study, Helsinki Health Study, and the Japanese Civil Servants Study. Soc Sci Med 66:1681–1698
Lang J, Ochsmann E, Kraus T, Lang JW (2012) Psychosocial work stressors as antecedents of musculoskeletal problems: a systematic review and meta-analysis of stability-adjusted longitudinal studies. Soc Sci Med 75:1163–1174
Lawrence RH, Jette AM (1996) Disentangling the disablement process. J Gerontol B Psychol Sci Soc Sci 51:S173–S182
Lee CT, Yeh CJ, Lee MC, Lin HS, Chen VC, Hsieh MH, Yen CH, Lai TJ (2012) Leisure activity, mobility limitation and stress as modifiable risk factors for depressive symptoms in the elderly: results of a National Longitudinal Study. Arch Gerontol Geriatr 54:e221–e229
Leino PI, Hänninen V (1995) Psychosocial factors at work in relation to back and limb disorders. Scand J Work Environ Health 21:134–142
Lihavainen K, Sipilä S, Rantanen T, Sihvonen S, Sulkava R, Hartikainen S (2010) Contribution of musculoskeletal pain to postural balance in community-dwelling people aged 75 years and older. J Gerontol A Biol Sci Med Sci 65:990–996
Mehta RK, Parijat P (2012) Associations between psychosocial risk factors and musculoskeletal disorders: application to the IT profession in India. Work 41(Suppl 1):2438–2444
Milaneschi Y, Tanaka T, Ferrucci L (2010) Nutritional determinants of mobility. Curr Opin Clin Nutr Metab Care 13:625–629
Netuveli G, Wiggins RD, Hildon Z, Montgomery SM, Blane D (2006) Quality of life at older ages: evidence from the English longitudinal study of aging (wave 1). J Epidemiol Community Health 60:357–363
Ng DM, Jeffery RW (2003) Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychol 22:638–642
Nieuwenhuijsen K, Bruinvels D, Frings-Dresen M (2010) Psychosocial work environment and stress-related disorders, a systematic review. Occup Med (Lond) 60:277–286
Nyberg ST, Fransson EI, Heikkilä K, Alfredsson L, Casini A, Clays E, De Bacquer D, Dragano N, Erbel R, Ferrie JE, Hamer M, Jockel KH, Kittel F, Knutsson A, Ladwig KH, Lunau T, Marmot MG, Nordin M, Rugulies R, Siegrist J, Steptoe A, Westerholm PJ, Westerlund H, Theorell T, Brunner EJ, Singh-Manoux A, Batty GD, Kivimäki M, IPD-Work Consortium (2013) Job strain and cardiovascular disease risk factors: meta-analysis of individual-participant data from 47,000 men and women. PLoS One 8:e67323
Rantakokko M, Mänty M, Rantanen T (2013) Mobility decline in old age. Exerc Sport Sci Rev 41:19–25
Sembajwe G, Tveito TH, Hopcia K, Kenwood C, O’Day ET, Stoddard AM, Dennerlein JT, Hashimoto D, Sorensen G (2013) Psychosocial stress and multi-site musculoskeletal pain: a cross-sectional survey of patient care workers. Workplace Health Saf 61:117–125
Shah D (2009) Healthy worker effect phenomenon. Indian J Occup Environ Med 13:77–79
Shumway-Cook A, Ciol MA, Yorkston KM, Hoffman JM, Chan L (2005) Mobility limitations in the medicare population: prevalence and sociodemographic and clinical correlates. J Am Geriatr Soc 53:1217–1221
Toivanen S (2011) Exploring the interplay between work stress and socioeconomic position in relation to common health complaints: the role of interaction. Am J Ind Med 54:780–790
Tuomi K, Ilmarinen J, Klockars M, Nygård CH, Seitsamo J, Huuhtanen P, Martikainen R, Aalto L (1997) Finnish research project on aging workers in 1981–1992. Scand J Work Environ Health 23(Suppl 1):7–11
Vincent HK, Vincent KR, Lamb KM (2010) Obesity and mobility disability in the older adult. Obes Rev 11:568–579
von Bonsdorff MB, Seitsamo J, Ilmarinen J, Nygård CH, von Bonsdorff ME, Rantanen T (2011) Work ability in midlife as a predictor of mortality and disability in later life: a 28-year prospective follow-up study. CMAJ 183:E235–E242
Vrijkotte TG, van Doornen LJ, de Geus EJ (1999) Work stress and metabolic and hemostatic risk factors. Psychosom Med 61:796–805
Wahrendorf M, Sembajwe G, Zins M, Berkman L, Goldberg M, Siegrist J (2012) Long-term effects of psychosocial work stress in midlife on health functioning after labor market exit—results from the GAZEL study. J Gerontol B Psychol Sci Soc Sci 67:471–480
World Health Organisation (2001) International Classification of Functioning, Disability and Health (ICF). WHO, Geneva
Yeom HA, Fleury J, Keller C (2008) Risk factors for mobility limitation in community-dwelling older adults: a social ecological perspective. Geriatr Nurs 29:133–140
Acknowledgments
Gerontology Research Center is a joint effort between the University of Jyväskylä and the University of Tampere. FLAME was supported by the Finnish Institute of Occupational Health and the Local Governments Pension Institution. J. Kulmala was supported by grant 250385 from the Academy of Finland. M.B. von Bonsdorff was supported by grant 257239 from the Academy of Finland. M.E. von Bonsdorff was supported by grant 250681 from the Academy of Finland. T. Rantanen was supported by grant 132597 from the Academy of Finland.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Kulmala, J., Hinrichs, T., Törmäkangas, T. et al. Work-related stress in midlife is associated with higher number of mobility limitation in older age—results from the FLAME study. AGE 36, 9722 (2014). https://doi.org/10.1007/s11357-014-9722-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11357-014-9722-4